


Introduction
Chronic kidney disease (CKD) is the leading cause of global public health problems. Mortality due to CKD has increased globally by 41.5% since 1990 [1]. Identifying high-risk patients who will progress to CKD is crucial, and these individuals need strict monitoring to improve outcomes in routine clinical practice [2]. The major risk factors for CKD are cardiovascular disease (CVD), diabetes mellitus (DM), hypertension (HTN), and atherosclerosis [2]. CVD is usually chronic, and individuals with these factors are frequently found in a state of advanced CKD [2]. Dietary habit has been recognized as a modifiable factor for the development of advanced CKD.
Smoking and dietary sodium intake have been reported as risk factors for HTN, CVD, and CKD [3]. However, data on the effect of smoking and sodium intake on renal outcomes are conflicting. Smoking was significantly associated with CKD in a meta-analysis [4]. In some cohort studies, smoking was not related to CKD development [5,6]. The amount of smoking and sodium intake could be inaccurate because they largely depend on the subject’s answer to the questionnaire.
Smoking could be indirectly associated with CKD because smoking is also a risk factor for coronary artery disease, stroke, or male sex [7]. In addition, several studies have shown that smoking directly exerts a harmful effect on the kidney by worsening oxidative stress, endothelial dysfunction, and activation of fibrotic mediators [7,8]. On the other hand, smoking has been reported to influence sodium intake and food habits through the altered perception of salty taste and socioeconomic and psychological factors [9]. However, it is largely unknown whether smoking could influence sodium intake, and this increased sodium intake could affect the progression of CKD.
Herein, we investigated whether 1) smoking is directly associated with albuminuria, 2) smoking is related to high sodium intake, and 3) smoking influences albuminuria through an increase in sodium intake by an objective marker of smoking and sodium intake: cotinine and estimated urine sodium excretion.
Methods
Study population
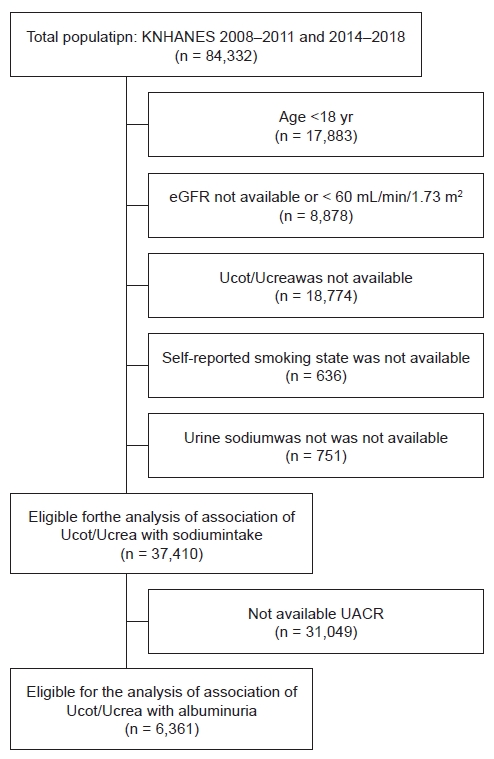
We collected data from the Korea National Health and Nutrition Examination Survey (KNHANES) conducted in 2008–2011 and 2014–2018 (conducted by the Korea Centers for Disease Control and Prevention since 1998). The KNHANES is a nationwide health examination survey that applies a stratified multistage probability sampling design to select a representative sample of the Korean population. Among 84,332 participants, we excluded 46,297 participants aged <18 years, those with an estimated glomerular filtration rate (eGFR) of <60 mL/min/1.73 m2, those with missing data on urine cotinine (Ucot), and those with self-reported smoking status. Finally, 37,410 individuals were included in the present study. The urine albumin-creatinine ratio (UACR) was available for 6,361 participants (Fig. 1). We divided participants into quartile groups according to the dietary sodium intake and tertile groups according to Ucot/urine creatinine ratio (Ucrea).
Participants in KNHANES provided informed consent. The survey was approved by the Institutional Review Board of the Centers for Disease Control and Prevention in Korea (IRB No. 2008-04EXP-01-C, 2010-02CON-21-C, 2011-02CON-06-C, 2013-12EXP-03-5C, 2015-01-02-6C, 2018-01-03-P-A).
Measurement of urine cotinine/creatinine ratio
Spot urine samples were collected from the participants in the morning from a midstream void. Ucot levels were measured by gas chromatography-mass spectrometry with a PerkinElmer Clarus 600 T gas chromatograph/mass spectrometer (PerkinElmer) between 2008 and 2015 or by liquid chromatography-mass spectrometry with an Agilent 1100 series coupled with API 4000 liquid chromatography/mass spectrometer (AB Sciex) between 2016 and 2018. Ucrea levels were measured by the Jaffé rate-blanked compensated method using a Hitachi Automatic Analyzer 7600-210 (Hitachi). Ucot/Ucrea was expressed as nanograms of Ucot per milligram of Ucrea (ng/mg).
Measurement and definition of dietary sodium intake
Sodium intake was assessed using the spot urine sodium concentration with two formulas proposed by Kawasaki and Tanaka and assumed from the food intake questionnaire. The calculations of sodium intake are described in a previous study [10,11]. Urinary sodium (UNa) levels were measured by the ion-selective electrode method using a Hitachi Automatic Analyzer 7600-210. For the estimation of sodium intake by the 24-hour recall, we adapted sodium intake calculated from the food intake frequency survey of KNHANES data.
Measurement and definition of albuminuria
Spot urine samples were collected from the subjects in the morning from a midstream void. Urinary albumin levels were measured by the turbidimetric assay using the Hitachi Automatic Analyzer 7600. UACR was expressed as milligrams of urinary albumin per gram of Ucrea (mg/g). Albuminuria was defined as a UACR of ≥30 mg/g.
Demographic and biological measurements
Information on age, sex, smoking status, and comorbidities was obtained using a health questionnaire. Pack-years of smoking was calculated by multiplying the number of cigarette packs smoked per day by the number of years the person has smoked. Body mass index (BMI) was calculated as body weight in kilograms divided by height in meters squared, both of which were measured by trained medical technicians following standardized protocols. Obesity was defined as a BMI of ≥25 kg/m2. Blood pressure (BP) was measured using a mercury sphygmomanometer, with the participants in a sitting position, having rested for 5 minutes. After three measurements, the average of the latter two measurements was used as the final data. HTN was defined as a systolic BP of ≥140 mmHg or diastolic BP of ≥90 mmHg or those following a course of antihypertensive medication at the time of the interview. DM was defined as participants who fulfilled at least one of the following four criteria: fasting blood glucose of ≥126 mg/dL; those following a course of medication or insulin to decrease blood glucose level at the time of interview; and self-report of having received a physician’s diagnosis of DM. Dyslipidemia was defined as a fasting total cholesterol level of ≥240 mg/dL or when participants were taking lipid-lowering agents. Myocardial infarction, angina, and stroke were defined based on self-reported history. Blood samples were obtained after ≥8 hours of fasting, transported in cold storage to the Central Testing Institute, and analyzed within 24 hours. Serum creatinine levels were measured by the Jaffé rate-blanked compensated method using the Hitachi Automatic Analyzer 7600-210 (Hitachi). The eGFR was estimated using the CKD Epidemiology Collaboration equation [12].
Statistical analysis
All analyses were performed using IBM SPSS version 25.0 (IBM Corp.). Data are presented as mean ± standard deviation or standard error for continuous variables and numbers with percentages for categorical variables. Differences were analyzed using the chi-square test for categorical variables and analysis of variance for continuous variables. The R coefficient was estimated to measure the degree of association between the amount of smoking and Ucot/Ucrea. Multivariable logistic regression analysis was performed to evaluate the relationship between dietary sodium intake and albuminuria. Odds ratios (ORs) and 95% confidence intervals (CIs) were assessed after adjusting for multiple covariates. A p-value of <0.05 was considered significant.
Results
Baseline characteristics
A total of 37,410 participants were included in the study. We divided the participants into tertiles based on the Ucot/Ucrea. The characteristics of the study participants are listed in Table 1. Participants in the highest tertile were predominantly male and the youngest (p < 0.001). This group had the highest BMI, fasting glucose, hemoglobin A1c, aspartate transaminase, alanine aminotransferase, and triglyceride (p < 0.001). In addition, the participants in the highest tertile had the highest hemoglobin and eGFR. Participants in the second tertile were the oldest and exhibited the highest prevalence of HTN DM, angina, and malignancy (p < 0.001) (Table 1; Supplementary Table 1, available online).
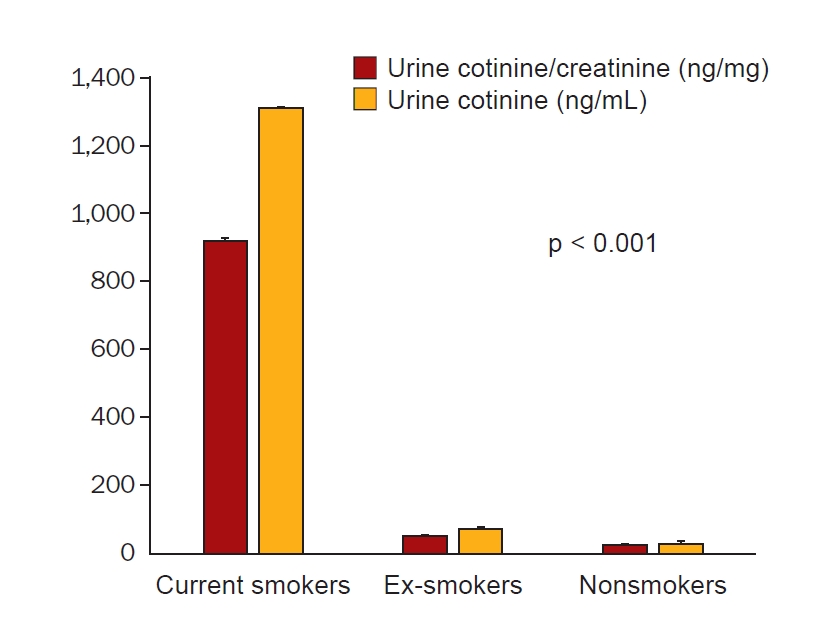
Association of smoking with urine cotinine/creatinine ratio and urine cotinine concentration
Associations of Ucot/Ucrea and Ucot with the amount of smoking in pack-years were evaluated. There was a moderate correlation between Ucot/Ucrea and the amount of self-reported smoking expressed in pack-years (r = 0.44, p < 0.001). The mean values of Ucot/Ucrea and Ucot were significantly higher in current smokers than in ex-smokers and nonsmokers (918.18 ± 9.08 ng/mg vs. 48.10 ± 2.48 ng/mg, 23.18 ± 1.28 ng/mg, p < 0.001; 1,308.62 ± 10.01 ng/mL vs. 68.55 ± 3.28 ng/mL, 25.70 ± 1.18 ng/mL, p < 0.001) (Fig. 2).
Association of passive smoking with urine cotinine/creatinine ratio and urine cotinine
Those who were exposed to second-hand smoke (SHS) presented with significantly higher Ucot/Ucrea and Ucot levels compared with those who were not exposed to SHS (345.47 ± 6.93 ng/mg vs. 174.20 ± 3.00 ng/mg, p < 0.001 and 492.30 ± 8.68 ng/mL vs. 243.60 ± 3.77 ng/mL, p < 0.001). Nonsmokers who were exposed to SHS showed significantly higher Ucot/Ucrea and Ucot levels than those who were not exposed to SHS (41.83 ± 4.01 ng/mg vs. 17.64 ± 1.28 ng/mg, p < 0.001 and 43.32 ± 3.39 ng/mL vs. 20.09 ± 1.22 ng/mL, p < 0.001).
Association of dietary sodium intake and urine cotinine-verified smoking status
The association between dietary sodium intake and Ucot/Ucrea levels was analyzed. Ucot/Ucrea levels were positively associated with sodium intake (p for trend < 0.001). The second and third tertiles of Ucot/Ucrea showed significantly higher dietary sodium intake assessed by various methods (Kawasaki formula: 4.34 ± 1.31 g, 3.91 ± 1.37 g vs. 3.75 ± 1.18 g, p < 0.001; Tanaka formula: 3.33 ± 0.80 g, 3.21 ± 0.84 g vs. 2.99 ± 0.74 g, p < 0.001; and 24-hour recall: 3.85 ± 3.40 g, 4.54 ± 2.96 g vs. 3.64 ± 2.48 g, p < 0.001) (Table 2).
Association of urine cotinine-verified smoking status with albuminuria
The prevalence of albuminuria was not associated with Ucot/Ucrea (p = 0.87) or self-reported smoking status (p = 0.37). Unadjusted and multivariate analyses showed that the risk of albuminuria was not associated with the levels of Ucot/Ucrea (Supplementary Table 2, available online).
Association of dietary sodium intake and albuminuria
The sodium intake quartile group had a linear relationship with the UACR (p for trend < 0.001) (n = 6,361). The prevalence of albuminuria increased according to the sodium intake quartiles (5.3%, 5.7%, 7.1%, and 9.9%; p < 0.001). The highest quartile of sodium intake was significantly associated with an increased risk of albuminuria in the unadjusted analysis (OR, 1.97; 95% CI, 1.50–2.56; p < 0.001). When risks were adjusted by multiple factors, the highest quartile of sodium intake showed a significant 1.49-fold risk in the presence of albuminuria compared with the corresponding risk in the lowest quartile (95% CI, 1.09–2.04; p = 0.01) (Supplementary Table 3, available online). We investigated the interaction between sodium intake and Ucot/Ucr for the risk of albuminuria. The interaction was not significant (p = 0.88).
Association of dietary sodium intake and albuminuria according to urine cotinine-verified smoking status
Stratified analysis was conducted using the Ucot/Ucrea tertile. The prevalence of albuminuria increased in all the Ucot/Ucrea tertile groups according to the sodium intake quartile (Supplementary Table 4, available online). In the second and third Ucot/Ucrea tertile groups, the highest sodium intake quartile indicated a significantly higher risk of albuminuria compared with that in the lowest quartile in the unadjusted analysis (OR, 2.18; 95% CI, 1.24–3.83; p = 0.007 and OR, 2.65; 95% CI, 1.65–4.25; p < 0.001), whereas there was no significant difference in the risk of albuminuria in the first Ucot/Ucrea tertile. When risks were adjusted by multiple factors, only the highest quartile of sodium intake showed a significant risk of albuminuria compared with the corresponding risk in the lowest quartile (OR, 2.22; 95% CI, 1.26–3.91; p = 0.006) (Table 3).
Discussion
In this study, smoking was not directly related to albuminuria. However, smoking was associated with a high sodium intake. In individuals with higher cotinine excretion, high sodium intake was associated with an increased risk of albuminuria, although sodium intake was not associated with albuminuria in individuals with lower excretion of cotinine. Smoking acts as a risk amplifier for the association between sodium intake and albuminuria.
Smoking causes more than 480,000 deaths annually in the United States. It increases the risk of coronary artery disease and stroke by 2 to 4 times [3]. It leads to the development of atherosclerosis with narrowing of the vascular lumen and a hypercoagulable state, which increases the risk of acute thrombosis [7,8]. Smoking can cause endothelial damage and is associated with the development of HTN and type 2 DM. Nicotine has vasoconstrictive, proinflammatory, and prooxidant properties and promotes the development of kidney fibrosis [13]. However, data regarding the association between smoking and CKD showed conflicting results. Current smokers were associated with an increased risk of albuminuria in a cross-sectional study [14]. Smokers had significantly higher risk factor for the development of CKD [4,15,16]. In contrast, smoking status was the only significant risk factor for the development of end-stage kidney disease (ESKD) in men, not in women [17]. Smoking status was not associated with incident proteinuria [6,18]. Among 1,306 patients with stage III–V CKD, current and former smokers were not independently related to the development of ESKD or 50% eGFR decline [5]. These conflicting results could be explained by several factors such as patient demographics, inaccuracy of questionnaire-based smoking status, heterogeneous measurement of albuminuria, or adjusted confounding factors.
Cotinine is the major metabolite of nicotine that has a long biological half-life of 18 hours in the body and is considered the gold standard measure of smoking exposure [19–21]. Cotinine was effective in evaluating exposure to SHS [22]. A previous study reported high Ucot levels in participants with SHS exposure. In this study, we noted a significantly high level of Ucot or Ucot/Ucrea in participants without a smoking history. The association of the cotinine-verified smoking status with albuminuria was analyzed; however, this association was significant in middle-aged and older populations [23]. We evaluated the association between the cotinine-verified smoking status and albuminuria in a large general population with central laboratory measurements.
Food habits change in individuals who smoke. Current smokers were more likely to have a higher salt concentration than nonsmokers [9]. In an experimental study, smokers showed a higher tendency to eat salty food [24]. Nicotine plays a role in the modulation of taste signals [25]. In addition, emotional and uncontrolled eating is related to a high intake of salty food [26]. In this study, higher tertile of cotinine excretion was significantly associated with higher sodium intake. High salt intake was associated with an increased risk of CKD progression in patients with CKD [27]. The adverse effects of increased sodium intake on target organs are thought to be linked to elevated BP. High dietary sodium increases oxidative stress and intrarenal expression of transforming growth factor-β and decreases nitric oxide, thereby having direct effects on the endothelium [28,29]. Moreover, studies have shown that dietary sodium influences insulin resistance and metabolic syndrome [11]. Therefore, smokers who eat salty food are at double the risk for kidney damage.
Salt intake more than two-fold increases the risk of rheumatoid arthritis in smokers; however, this finding was not significant in nonsmokers [30]. Smoking was not directly related to renal outcomes but served as a risk amplifier for the association between renal outcomes and other risk factors [5]. In this study, we revealed that smokers who consumed a high-sodium diet were associated with a 2.22-fold increase in the risk of albuminuria (95% CI, 1.26–3.92). This was not significant among participants in the middle and lowest tertiles of Ucot/Ucrea after adjustment for multiple risk factors.
The strength of this study is that we used a large, nationwide dataset representative of the general population, and UNa, cotinine excretion, and other values were measured consistently among all participants using an identical method. Second, we defined sodium intake and smoking status based on objective laboratory parameters. Finally, we adjusted the data for multiple confounding variables, including major comorbidities.
Despite its strengths, this study has certain limitations. First, the study population comprised only Koreans, and race differences were not assessed in this study. Second, the data were not adjusted for the participants’ medication histories. Sodium excretion can be affected by antihypertensive medications such as diuretics. Third, the interaction between smoking and sodium intake was not statistically significant. Therefore, the additive effect between smoking and sodium intake could not be concluded in this study. Finally, this was a cross-sectional study; therefore, causality could not be assessed.
Smokers consume higher dietary sodium, and dietary sodium intake is positively related to the risk of albuminuria. Smoking is not a direct risk factor for albuminuria. The risk of albuminuria is doubled in smokers who have a high sodium intake. The results shed light on smoking and high sodium intake as significant modifiable risk factors for renal outcome.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









