


Introduction
Continuous ambulatory peritoneal dialysis (CAPD) is an important treatment option for patients who are at the end stage of renal disease. Although the rate of peritonitis has declined in recent years because of improvements in the CAPD technique, peritonitis remains the leading cause for discontinuation of CAPD [1].
Sphingomonas paucimobilis is frequently isolated from environmental sources such as soil and water, and it is found on hospital equipment such as ventilators, nebulizers, and humidifiers [2], [3]. Although S. paucimobilis plays an extremely limited role as an infectious agent [4], it is responsible for two types of human infections: community-acquired infection and nosocomial infection [5]. Cases of peritonitis by S. paucimobilis have been reported rarely. The clinical outcomes were diverse in previously reported peritoneal dialysis (PD)-associated peritonitis cases [2], [5], [6], [7]. Furthermore, definitive guidelines do not exist for treating S. paucimobilis.
Cases of PD-associated peritonitis caused by S. paucimobilis have been reported worldwide, and one case caused by coinfection with S. paucimobilis and Chryseobacterium indologenes was reported in Korea [8]. However, this is the first case report of peritonitis due to S. paucimobilis as a single pathogen in Korea. We describe a case of PD-associated peritonitis due to S. paucimobilis that was resolved after catheter removal.
Case report
A 63-year-old man who had been treated with CAPD for 6 years was admitted to our hospital because of a turbid peritoneal effluent accompanied by constant abdominal pain that began 2 days prior to his admission. The underlying cause of the patientŌĆÖs end-stage renal disease was diabetes mellitus and hypertension, and his dialysis treatment consisted of four exchanges of 2 L dialysate per day. He had been engaged in rice farming and lived in the countryside. He had been treated for peritonitis with Pseudomonas aeruginosa and Staphylococcus epidermidis 7 months previously.
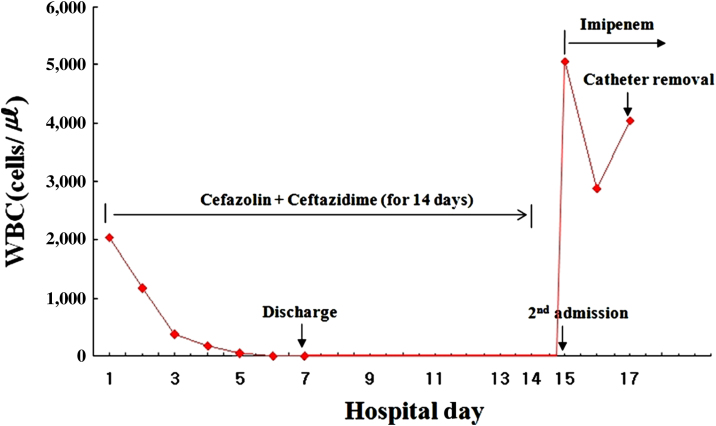
On admission, his blood pressure was 165/80 mmHg, heart rate was 84 beats/min, respiratory rate was 19/min, and body temperature was 36.8┬Ā┬░C. His abdomen was diffusely tender with normal bowel sounds, and infection was not found around the catheter exit site. The laboratory findings showed PD peritonitis: the white blood cell (WBC) count of the peritoneal effluent was 2,040/mm3 with a neutrophil predominance (85%). His hemoglobin was 11.3┬Āg/dL, WBC count was 7.6├Ś109/L, and C-reactive protein was 5.9┬Āmg/dL (normal: <0.8┬Āmg/dL). Bacteria were not observed on Gram stain examination. After peritoneal fluid was sent for bacterial culture, a single 1-g dose of cefazolin and a single 1-g dose of ceftazidime were given intraperitoneally per day. Two peritoneal fluid samples were inoculated into a BACTEC plus Aerobic/F culture bottle (Becton Dickinson Diagnostic Instrument System, Drogheda, Ireland) and incubated in a BACT/ALERT 3D Blood Culture System (Biomerieux, Marcy l├©toile, France). Culture of the peritoneal dialysate revealed S. paucimobilis, which was susceptible to ceftazidime, cefotaxime, imipenem, meropenem, gentamicin, ciprofloxacin, and minocycline, and resistant to piperacillin, aztreonam, and colistin.
The peritoneal WBC decreased to 30/mm3 and the patientŌĆÖs clinical condition improved on the fifth day after starting intraperitoneal ceftazidime. The patient was discharged on Day 7 with 7-day intraperitoneal antibiotics. The next day after 14 days of intraperitoneal ceftazidime, abdominal pain developed again, and the effluent became turbid. The peritoneal effluent contained 2,880 WBC/mm3, of which 75% were neutrophils. Abdominal computed tomography and ultrasonography were normal. We started a 1-g dose of intraperitoneal imipenem twice daily instead of cefazolin and ceftazidime. The culture of the peritoneal dialysate at second admission showed S. paucimobilis that was resistant to ceftazidime, ampicillin/sulbactam, piperacillin, cefotaxime, cefepime, aztreonam, and amikacin, and susceptible to imipenem, meropenem, ciprofloxacin, minocycline, and trimethoprim-sulfamethoxazole. However, the patientŌĆÖs abdominal pain persisted and the WBC count of the peritoneal effluents became elevated to 4,300/mm3 (Figure 1). Therefore, we removed the Tenckhoff catheter 3 days later despite continued imipenem therapy, and PD was switched to hemodialysis. The culture of the catheter tip was negative. Imipenem was continued for another week and the patientŌĆÖs clinical condition improved. The patient has been maintained on hemodialysis after catheter removal.
Discussion
PD-associated peritonitis caused by S. paucimobilis is rare, and this bacillus has not been reported as the single causative pathogen of PD-associated peritonitis in Korea. We report a case of peritonitis due to S. paucimobilis that required catheter removal.
S. paucimobilis is a yellow-pigmented, gram-negative bacillus that has a single polar flagellum with slow mobility. These bacteria are aerobic, nonfermentative, oxidase positive, and catalase-positive [9]. Although human infections caused by S. paucimobilis are generally rare [4], these infections appear to have increased in humans in recent years [10]. Such a finding was probably considered to be associated with hospital-acquired infection due to indwelling intravascular devices [3], [10]. Peritonitis caused by S. paucimobilis has been reported in patients undergoing peritoneal dialysis. In Korea, only one case of peritonitis caused by S. paucimobilis and C. indologenes has been reported [8]. However, this is the first case report of PD-associated peritonitis due to S. paucimobilis as a single pathogen in Korea.
Since the first two cases of PD-associated peritonitis by S. paucimobilis were described by Glupczynski et al [2], several other cases have been reported, with diverse clinical courses and outcomes [2], [5], [6], [7]. Although Hsueh et al [3] suggested that imipenem alone or an aminoglycoside plus a third-generation cephalosporin could effectively treat infections caused by S. paucimobilis, no definitive guideline exists for the treatment of this organism. In previous reports, half of the reported cases were treated successfully with antibiotics alone, but the other half underwent catheter removal [2], [5], [6], [7]. In our case, S. paucimobilis continued to grow in peritoneal effluent cultures upon the patientŌĆÖs second admission, and the peritoneal WBC count was increased despite the use of antibiotics such as imipenem for 3 days. Therefore, we removed the Tenckhoff catheter and PD was switched to hemodialysis.
In the case discussed here, at first admission, the dialysate was clear and abdominal pain disappeared following intraperitoneal administration of ceftazidime, which was effective against S. paucimobilis. However, peritonitis by the same organism recurred on the 15th day during antibiotic treatment. In this circumstance, adding aminoglycoside or changing antibiotics to imipenem was helpful for treatment of peritonitis caused by S. paucimobilis
[3], so we decided to use imipenem because the patient had a urine output of more than 1,000┬ĀmL per day. According to International Society for Peritoneal Dialysis guidelines, antibiotics dose should be empirically increased by 25% in patients with residual renal function [11]. However, residual renal function was not considered in deciding the antibiotic dose. Thus, inadequate dosage of antibiotics might be one of the possible causes of treatment failures in this case.
In summary, we report a case of PD-associated peritonitis caused by S. paucimobilis that was treated by catheter removal. Therefore, catheter removal could be considered in cases of PD-associated peritonitis caused by S. paucimobilis. Adequate antibiotics dosage is essential to treat this rare peritonitis, especially in patients with residual renal function.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









