


Introduction
Estimation of the glomerular filtration rate (GFR) is the most important step in the diagnosis of chronic kidney disease (CKD), and significant research has been directed toward developing the most accurate, convenient, and reproducible equation. Traditionally, the Modification of Diet in Renal Disease (MDRD) [1], CockcroftŌĆōGault [2], and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) [3] equations have been considered the most acceptable creatinine-based equations for estimating GFR. The Kidney Disease Outcome Quality Initiative (K/DOQI) recommends using an abbreviated form of the MDRD equation (aMDRD) for clinical purposes [4]. A recent publication by Lee et al [5] adapted the aMDRD equation for a Korean population by adding a coefficient (K-aMDRD), which improved the estimated GFR (eGFR) performance and more closely approximated inulin clearance. However, there are a number of disadvantages in using serum creatinine itself as a filtration marker [6], [7]. Therefore, identifying a new endogenous filtration marker is necessary for the accurate and convenient estimation of GFR.
Serum cystatin C is a cationic nonglycosylated low-molecular-weight cysteine proteinase inhibitor produced at a constant rate by all nucleated cells and freely filtered at the glomerulus [8]. Approximately 99% of filtered cystatin C is reabsorbed in the proximal tubule, where it undergoes near-complete catabolization [9], [10]. Because of these features, serum cystatin C was proposed as a superior marker of GFR, and its superiority over serum creatinine in the early detection of acute kidney injury is already well established [11], [12]. However, its role as a filtration marker is still conflicting [13], [14], [15], and there is no validated cystatin C-based eGFR equation in predicting the glomerular rate in CKD patients [16], [17], [18], [19], [20].
Thus, in this study, we aimed to determine the performance of cystatin C in estimating GFR and the accuracy of six different cystatin C-based eGFR equations and compared the results with that of the K-aMDRD equation according to the CKD stage.
Methods
Patients
Serum creatinine and cystatin C levels were measured in 615 CKD patients who visited the Pusan National University Hospital between January 2011 and December 2011. The recruited patients were aged Ōēź18 years. Patients with thyroid dysfunction, inflammation, severe liver disease, or a history of steroid therapy were excluded [21], [22], [23]. Patients with extremely high eGFR calculated using the MDRD equation (eGFR>130┬ĀmL/minute/1.73┬Ām2) [5] and patients with end-stage renal disease on maintenance dialysis were also excluded. The local Ethics Committee approved this study to analyze anonymous, routinely collected clinical data and waived the requirement of informed consent.
Laboratory methods
Serum creatinine and serum cystatin C levels were measured in the same serum sample. Serum creatinine values were measured by the alkaline picrate Jaffe kinetic method, and cystatin C values were determined by turbidimetry-based immunoassays using reagents from Healthcare Innovation (HBI Co, Anyang, Korea). The ratio of serum cystatin C to creatinine (mg/L to mg/dL) was calculated without adjustment of the unit for ease of application.
GFR measurement and estimation
Measured GFR
The measured GFR (mGFR) was obtained by Tc-99m-diethylenetriamine pentaacetate (Tc-99m-DTPA) renal scintigraphy. After a bolus injection of 10-mCi Tc-99m-DTPA, GFR was obtained using the Gates method [24] during a renal scan with VERTEX (EPIC) gamma camera equipped with ADAC's DUAL DETECTOR (ADAC, Milpitas, CA, USA).
eGFR by serum creatinine
Serum creatinine-based eGFR was calculated by the CKD-EPI [3] and K-aMDRD equations [GFR=107.904 ├Ś ScrŌłÆ1.009 ├Ś ageŌłÆ0.02 (├Ś0.667 if woman)] [5]. The CKD stage was classified according to the recommendation of the Kidney Disease Improving Global Outcomes and National Kidney Foundation-K/DOQI guideline using the K-aMDRD equation [25].
eGFR by serum cystatin C
Serum cystatin C-based eGFR was calculated using six different equations published previously.
ŌĆó Larsson A et al [16]: GFR=99.43 ├Ś ScytCŌłÆ1.5837 (mL/minute/1.73┬Ām2)
ŌĆó Hoek FJ et al [17]: GFR=80.35/ScytCŌłÆ4.32 (mL/minute/1.73┬Ām2)
ŌĆó Le Bricon T et al [18]: GFR=78/ScytC+4 (mL/minute/1.73┬Ām2)
ŌĆó Filler G and Lepage N [19]: GFR=91.62 ├Ś ScytCŌłÆ1.123 (mL/minute/1.73┬Ām2)
ŌĆó Orebro-cystatin (DAKO) [19]: GFR=119/ScytC ŌĆō 33 (mL/minute/1.73┬Ām2)
ŌĆó Orebro-cystatin (Gentian) [19]: GFR=100/ScytC ŌĆō 14 (mL/minute/1.73┬Ām2)
Statistical analysis
Data were analyzed using SPSS for Windows, version 17.0 (SPSS Inc., Chicago, IL, USA). The Student t test was used for analysis of continuous variables and results are presented as mean┬▒standard deviation (SD). The Chi-square test was used for analysis of categorical variables. Differences in eGFR in each of the CKD stage were compared using a paired t test. The mean difference (bias) between the paired observation is given with SD (precision) and P values. The BlandŌĆōAltman plot was used to test the agreement between eGFRs from the K-aMDRD formula and the cystatin C-based equations, as well as between the K-aMDRD and mGFR [26]. Values of P<0.05 were considered statistically significant.
Results
Baseline characteristics
A total of 615 patients were enrolled in this study. The mean age of the recruited patients was 53.21┬▒14.45 years with 56.3% of patients being male. Patients with diabetes mellitus comprised 23.9% of the study population and hypertensive patients comprised 35.1%. The mean serum creatinine level was 2.52┬▒3.14┬Āmg/dL and the mean serum cystatin C level was 1.79┬▒1.18┬Āmg/L. The mean and upper 99th percentile serum cystatin C, respectively, according to the stages of CKD were as follows: CKD 1, 0.87┬▒0.20┬Āmg/L and 1.45┬Āmg/L; CKD 2, 1.20┬▒0.43┬Āmg/L and 2.20┬Āmg/L; CKD 3, 1.94┬▒0.49┬Āmg/L and 3.08┬Āmg/L; CKD 4, 3.13┬▒0.61┬Āmg/L and 4.29┬Āmg/L; CKD 5 4.25┬▒0.74┬Āmg/L and 6.08┬Āmg/L. Other baseline characteristics according to the CKD stage are summarized in Table 1.
Validation of the aMDRD equation with Korean coefficient
Of the 615 patients, 21 patients (CKD 4=16, CKD 5=5) underwent a nuclear medicine renal scan using DTPA. The mean mGFR was 19.18┬▒8.72┬ĀmL/minute/1.73┬Ām2 in CKD 4 and 13.19┬▒6.74┬ĀmL/minute/1.73┬Ām2 in CKD 5. The correlation coefficient between mGFR and eGFR was 0.5 (P=0.03). The BlandŌĆōAltman plot analysis of the degree of correspondence between the eGFR calculated by the K-aMDRD formula and the mGFR using DTPA scan revealed that the majority of results fell within the 95% confidence interval (Table 2, Fig. 1).
Cystatin C-to-creatinine ratio according to the CKD stage
Fig. 2A shows the cystatin C-to-creatinine ratios; the mean ratio was 0.95┬▒0.33 (mg/L to mg/dL). In CKD Stages 1ŌĆō3, the serum cystatin C level nearly coincided with the serum creatinine level. However, in CKD Stages 4 and 5, the serum cystatin C level did not increase as expected, and the cystatin C-to-creatinine ratio decreased to 0.75┬▒0.16 (mg/L to mg/dL) in CKD Stage 4, and to 0.49┬▒0.16 (mg/L to mg/dL) in CKD Stage 5 (Fig. 2B).
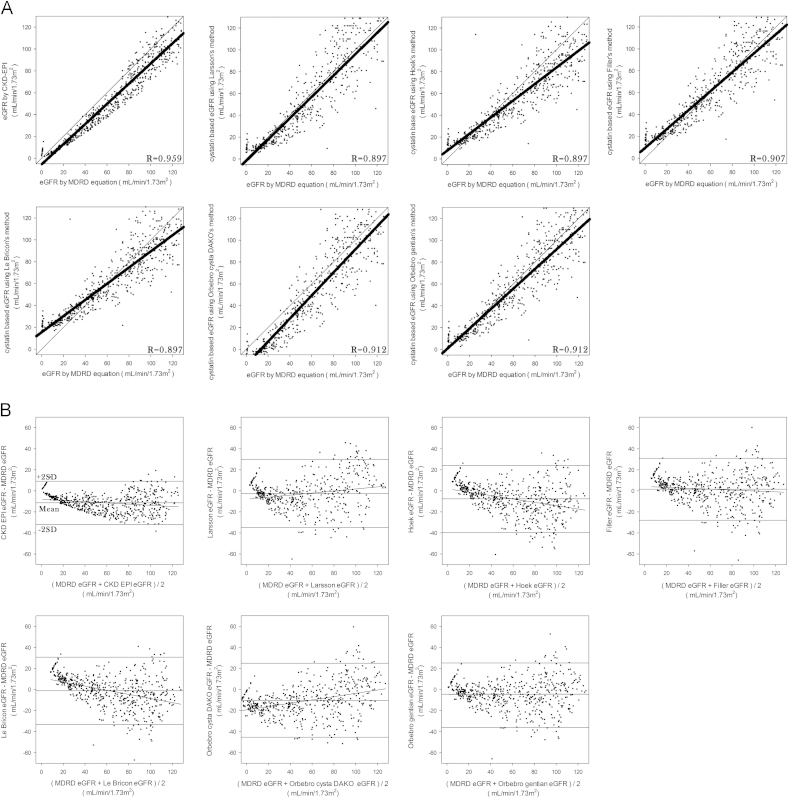
Comparison of cystatin C-based eGFRs
Compared with the results of the K-aMDRD equation, the cystatin C-based equations estimated a lower GFR in CKD Stages 1ŌĆō3, but presented differing results in Stages 4 and 5. Compared with the results of CKD-EPI, cystatin C-based eGFRs were higher in all the CKD stages (Table 3).
The eGFRs using serum cystatin C with the six different equations were slightly different when the GFR got lower. In particular, when compared with the K-aMDRD equation, the Hoek, Filler, and Le BriconŌĆÖs equations yielded higher eGFRs, whereas the Orebro-cystatin (DAKO) equation yielded lower eGFRs (Fig. 3).
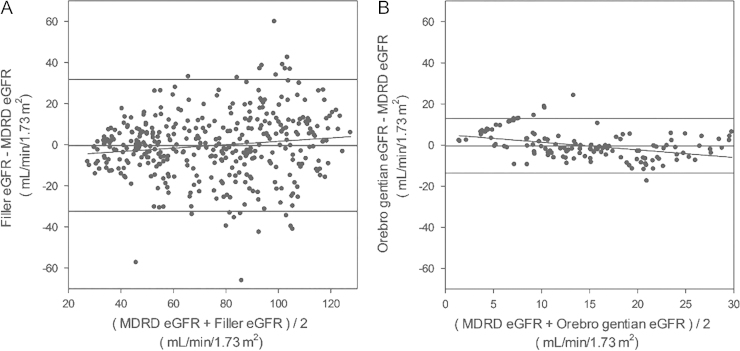
We measured the concordance between the GFRs estimated by each cystatin C-based equation and the K-aMDRD equation. FillerŌĆÖs equation yielded the most similar eGFRs in CKD Stages 1ŌĆō3 (74.77┬▒28.26┬ĀmL/minute/1.73┬Ām2 vs. 75.17┬▒28.26┬ĀmL/minute/1.73┬Ām2; P=0.622, bias=0.39┬▒16.09), whereas the Orebro-cystatin (Gentian) equation yielded the most similar eGFRs in Stages 4 and 5 (15.44┬▒9.45┬ĀmL/minute/1.73┬Ām2 vs. 15.17┬▒9.05┬ĀmL/minute/1.73┬Ām2; P=0.722, bias=0.27┬▒8.87; Table 3). Accordingly, the BlandŌĆōAltman plot showed the highest concordance with FillerŌĆÖs equation in Stages 1ŌĆō3, and the Orebro-cystatin (Gentian) equation in Stages 4 and 5 (Fig. 4).
Discussion
We evaluated the performance of serum cystatin C and the cystatin C-based eGFR equations and compared the results with that of the K-aMDRD equation according to the CKD stage. Inulin clearance and other methods using injected radioactive substances such as 52Cr-ethylenediaminetetraacetic acid, Tc-99m-DTPA are considered the true reference standards for determining GFR. Unfortunately, these tests are expensive and laborious, and therefore are not suited to clinical practice. In our cross-sectional retrospective study, we did not measure inulin clearance and performed DTPA renal scans in only 21 patients. Therefore, we were unable to compare the cystatin C-based estimates of GFRs with the true reference GFR. However, the recently proposed K-aMDRD equation is based on inulin clearance [5], and the MDRD equation has been previously validated in patients with CKD [27], [28]. In addition, although the number of patients was limited in our study, the BlandŌĆōAltman plot showed agreement between the K-aMDRD eGFR and the GFR measured by DTPA renal scans in 21 patients with CKD Stages 4 and 5. These findings suggest the validity of having used the K-aMDRD equation as a reference rather than as the true reference GFR.
We found that the cystatin C-based eGFR equations yielded values that differed greatly depending on the CKD stage. Overall, in Stages 1ŌĆō3, the eGFRs were lower than those calculated by the K-aMDRD equation, whereas the results differed by equation in Stages 4 and 5.
As previously reported, serum cystatin C concentration may underestimate renal dysfunction in advanced CKD because cystatin C did not increase along with the CKD stage, and the cystatin C-to-creatinine ratio decreased with advancing CKD stage [29]. It has been hypothesized that the discrepancy between serum creatinine and cystatin C may be due to extrarenal clearance of cystatin C [20]. In our study, the cystatin C-to-creatinine ratio was comparable with previously published values (Fig. 2), and the estimated rates from Hoek, Filler, and Le BriconŌĆÖs equations were greater than those from the K-aMDRD equation in CKD Stages 4 and 5 (Table 4), as the previously cited group suggested [20]. By contrast, we found that the Orebro-cystatin (Gentian) equation generated eGFR values comparable with those of the K-aMDRD equation in all CKD stages.
In the Orebro-cystatin (Gentian) equation, unlike the other cystatin C-based eGFR equations, both the production rate and extrarenal clearance of cystatin C are taken into account [30]. This could prevent an overestimation of eGFR in patients with CKD Stage 4 or 5.
The Orebro-cystatin (DAKO) equation also considered the extrarenal elimination of cystatin C, and this equation used the same template as the Orebro-cystatin (Gentian) equation [19]. However, the results from this equation were not comparable with the eGFR calculated using the K-aMDRD equation, because the reagents used in the determination of serum cystatin C levels were different. Tidman et al [30] reported that serum cystatin C determined by the Gentian method was approximately 40% higher than the DAKO method in the low GFR range. This may explain the differing results of the DAKO and Gentian equations. In our study, cystatin C was measured by turbidimetric methods using HBI reagents produced in Korea, which differ from the Gentian methods. Nonetheless, the Gentian equation generated eGFRs comparable with those generated by the K-aMDRD equation in patients with CKD Stages 4 and 5. Based on previously published literature, creatinine-based MDRD equations are known to underestimate the GFR in patients with a GFR>60┬ĀmL/minute/1.73┬Ām2
[31]. By contrast, we found the eGFR from the K-aMDRD equation to be higher than those from the cystatin C-based equations. This may be due to improved accuracy of the modified equation [5], or possibly due to the superior performance of cystatin C as an early marker of GFR decline [32], [33].
The eGFRs produced by the six cystatin C-based equations differed widely. We found that FillerŌĆÖs equation yielded results most similar to those of the K-aMDRD equation in CKD Stages 1ŌĆō3, whereas the Orebro-cystatin (Gentian) equation performed similarly in CKD Stages 4 and 5. However, given the lack of a true reference GFR in our study, we are unable to conclude that these equations are the most accurate.
In summary, the eGFRs calculated by the six cystatin C-based equations differed from each other and from those calculated by the K-aMDRD equation. Therefore, further study is needed to determine the most suitable equation to estimate GFR in Koreans with CKD.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









