


Introduction
Acute kidney injury (AKI) frequently occurs in critically ill patients and is associated with significant mortality and morbidity [1]. In patients with severe AKI requiring renal replacement therapy, the rate of in-hospital mortality has been reported to be 50% to 60% over the past two decades [2,3]. For those who survive, the AKI episode confers a risk of several complications, including progression to chronic kidney disease and subsequent events such as myocardial infarction and congestive heart failure [4–8].
Either intermittent hemodialysis or continuous kidney replacement therapy (CKRT) may be provided to patients who have severe AKI. CKRT is often the initial option in critically ill patients with AKI due to its superior hemodynamic stability and continuous removal of water and uremic solutes [9]. Despite the merit of CKRT, the survival benefit has not been conclusively documented in comparison to intermittent hemodialysis [10–13]. Given the high costs, prolonged immobilization, and requirement of admission to the intensive care unit (ICU) for CKRT, intermittent hemodialysis may become a viable therapeutic alternative for both hemodynamically stable and sometimes unstable patients [13,14].
Intradialytic hypotension (IDH) is a prevalent complication of hemodialysis. The pathophysiological mechanisms underlying IDH include decreased organ perfusion, particularly in the heart and brain, leading to ischemic injury and further exacerbation of cardiovascular disease [15]. Maintenance hemodialysis with IDH has been linked to severe adverse events, including major cardiac events, stroke, loss of residual kidney function, and mortality [16–19]. However, studies investigating the association between IDH and adverse outcomes in AKI are scarce. Herein, we addressed this issue using a cohort of AKI patients receiving intermittent hemodialysis as their initial modality and further identified risk factors related to IDH occurrence.
Methods
The study protocol was approved by the Institutional Review Board (IRB) of the Seoul National University Hospital (No. H-2110-085-1262) and was conducted in accordance with the ethical standard outlined in the Declaration of Helsinki. The IRB waived the need for informed consent because of the retrospective design.
Patient and data collection
This study is a retrospective analysis involving a cohort of 1,460 patients who were diagnosed with severe AKI and received intermittent hemodialysis as their initial modality at Seoul National University Hospital between November 2004 and June 2022. The hemodialysis modality was determined based on the patient’s status, such as vital instability. The study patients did not require care from the ICU at the time of initiating hemodialysis. Criteria for exclusion included patients under the age of 18 (n = 121), those who were initially admitted to the ICU (n = 270), those who had end-stage kidney disease (ESKD) (n = 24), and those with missing data (n = 36). Accordingly, a total of 1,009 patients were included in the final analysis.
Baseline data at the first session of hemodialysis were obtained, such as age, sex, weight, initial vital signs (e.g., systolic [SBP] and diastolic blood pressures [DBP] and pulse rate), hemodialysis duration, blood flow rate, ultrafiltration volume, diagnosis of septic AKI, and comorbidities (e.g., diabetes mellitus, hypertension, coronary heart disease, liver cirrhosis, chronic kidney disease, and active malignancy). Blood findings included blood urea nitrogen, creatinine, sodium, potassium, chloride, bicarbonate, bilirubin, albumin, and C-reactive protein. During each hemodialysis session, blood pressure (BP) was regularly monitored, essentially every hour, and was measured more often in cases of hemodynamic instability. Subsequently, IDH of the first session of hemodialysis was incorporated into the analysis.
Because there is no consensus on defining IDH when patients have AKI rather than maintenance hemodialysis, we referred to the methods used in previous studies, as follows [20]: discontinuation of dialysis as a result of hemodynamic instability plus a nadir SBP less than 90 mmHg and/or a decrease in SBP of ≥30 mmHg.
Outcomes
The primary outcome was all-cause mortality following the initiation of hemodialysis, up to the point of either hospital discharge or death. Additionally, we assessed the rate of transfer to the ICU due to hemodynamic instability subsequent to the initial hemodialysis session.
Statistical analysis
Categorical and continuous variables are presented as proportions and means ± standard deviations when exhibiting a normal distribution and as medians with interquartile ranges (IQRs) when lacking a normal distribution. The Kolmogorov-Smirnov test was employed to analyze the distribution’s normality. Categorical variables were compared using the chi-square test or Fisher exact test, while continuous variables with or without normal distribution were compared using the Student t test or the Mann-Whitney U test, respectively.
Survival curves were generated using the Kaplan-Meier method and compared between groups through a log-rank test. Hazard ratios (HRs) and 95% confidence intervals of outcomes were determined using the Cox proportional hazard regression model. IDH events at multiple time points, adhering to the stated definition, were incorporated as a time-dependent variable to examine the impact of IDH on outcomes. To pinpoint risk factors for IDH, logistic regression with backward stepwise selection was utilized. All statistical analyses were conducted using IBM SPSS version 27 (IBM Corp.) and R version 4.1.1 (R Foundation for Statistical Computing). A p-value below 0.05 was deemed statistically significant.
Results
Patient characteristics
The mean patient age was 60.9 ± 16.0 years, and 61.4% of the patients were male. The proportion of patients with septic AKI was 47.8%. Median value of sessions was 4 (IQR, 2–9), and this value did not differ between the IDH and no IDH subgroups. Based on the first session, IDH occurred in 449 patients (44.5%). The IDH group was more likely to have a high initial BP and pulse rate and more comorbidities, such as liver cirrhosis and active malignancy. Other baseline characteristics are shown in Table 1.
Relationship between intradialytic hypotension and mortality
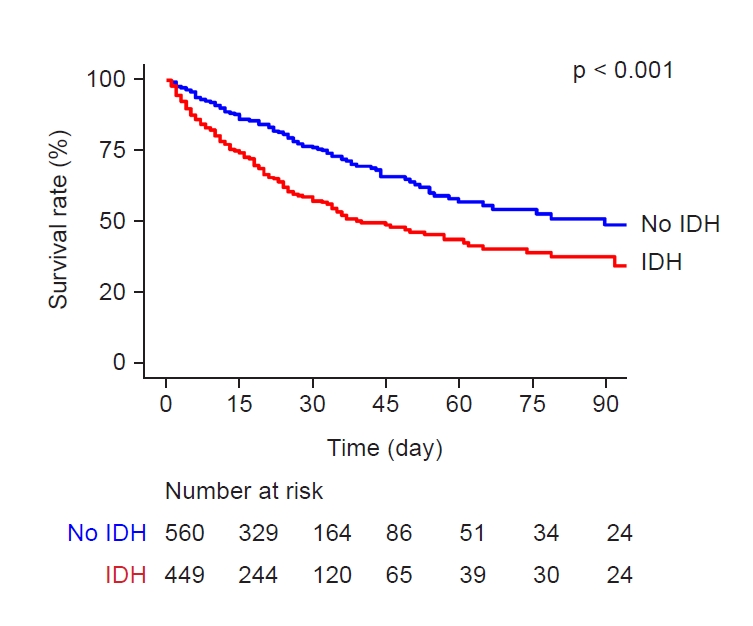
During a median follow-up period of 17 days (IQR, 9–33 days), 310 patients (30.7%) died. The incidence rate of mortality was 10.0 deaths per 1,000 person-days. Kaplan-Meier survival curves indicate the disparity in survival rates between patients who experienced IDH and those who did not (Fig. 1). Notably, the survival rate was lower in the group with IDH (p < 0.001). After adjustment for multiple variables, IDH was found to be an independent risk factor for all-cause mortality (Table 2).
Relationship between intradialytic hypotension and intensive care unit transfer
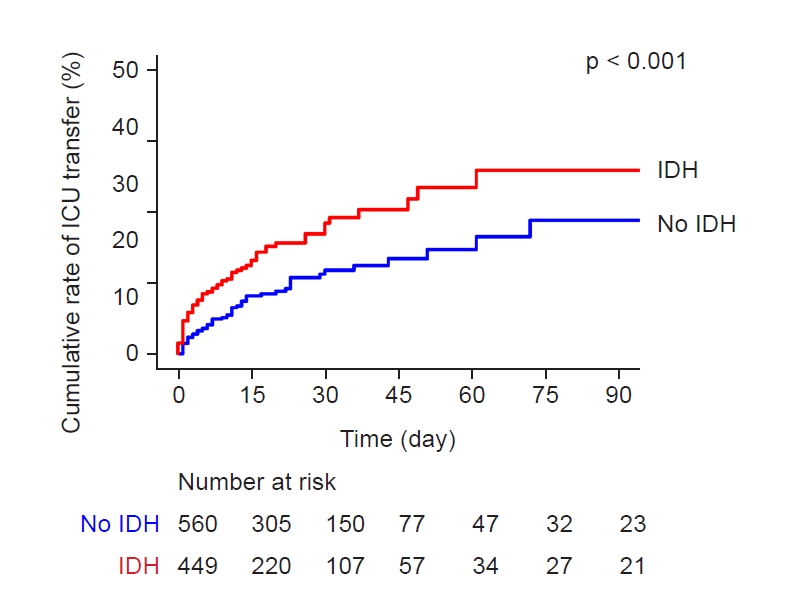
The study further examined the risk of transfer to the ICU due to hemodynamic instability after hemodialysis application. Of the patients, 144 (14.3%) were transferred to the ICU. Fig. 2 presents Kaplan-Meier curves illustrating the cumulative rates of ICU transfer in groups with and without IDH. Patients experiencing IDH were more likely to be transferred to the ICU than the counterpart group, and this finding remained consistent after adjustment for multiple variables (Table 3).
Factors related to intradialytic hypotension
Upon application of a multivariable logistic regression model with backward stepwise selection, several factors, including old age, elevated BP and pulse rate, hypoalbuminemia, and comorbidities, such as liver cirrhosis and active malignancy, were associated with the occurrence of IDH (Table 4).
Discussion
IDH occurrence is associated with adverse outcomes in patients on chronic or maintenance dialysis. However, this relationship has never been established in AKI patients requiring intermittent hemodialysis. According to our cohort analysis, IDH occurrence was associated with subsequent high risks of mortality and transfer to the ICU. Several factors were identified to be associated with IDH occurrence. These findings will help clinicians cope with AKI patients at risk of IDH to prevent worse outcomes.
IDH in patients with severe AKI requiring intermittent hemodialysis has been reported to occur in 30% to 90% of cases depending on the timing and protocol of hemodialysis as well as the definition of IDH [21,22]. We reported that approximately 45% of patients suffered IDH in the initial hemodialysis session, which ranges within the previous report and is a relatively high proportion in comparison to maintenance hemodialysis. Several mechanisms may further increase the risk of IDH in patients with AKI, such as fluid overload due to resuscitation in hemodynamic instability, insufficient support of nutrition, and use of nephrotoxic antibiotics [23]. Furthermore, IDH can occur because of an impaired response to physiological stress during hemodialysis, such as increased vascular resistance or decreased cardiac reserve due to critical illness [24,25].
A previous cohort study involving patients with AKI who underwent hemodialysis at outpatient units for 3 to 6 months after discharge showed that frequent occurrence of IDH led to a higher incidence of ESKD [26]. Another observational study involving patients on CKRT found that IDH occurring within the first hour of treatment initiation, defined by a drop in BP from the baseline, significantly elevated the mortality risk [27]. Similar but unlike the above two studies, our study compared the outcomes of patients with acute illness who had intermittent hemodialysis initiated in the ward, which might have an advantage in selecting vulnerable patients in the ward setting.
There is still no clear consensus on whether to choose intermittent hemodialysis or CKRT in critically ill patients with AKI, except in some situations such as cerebral edema [28]. We also found that the incidence of ICU transfer was closely related to IDH events after adjusting for potentially relevant known confounders. It seemed that for close monitoring of patients who developed IDH and had hemodynamical instability, the patients were transferred to the ICU, but this study could not determine whether this transition to CKRT as a dialysis modality could improve the prognosis by this observational study design.
Previous research has explored risk factors for IDH in patients undergoing maintenance hemodialysis, such as in patients who have diabetes mellitus or cardiovascular disease, including systolic and diastolic dysfunction, ischemic heart disease, and arrhythmias [29,30]. In addition to a large volume of ultrafiltration, rapid diffusive solute removal during hemodialysis precipitates IDH occurrence due to a swift decline in serum osmolality, consequently reducing extracellular fluid [31]. However, there is a gap in understanding regarding patients with AKI requiring intermittent hemodialysis. In critically ill patients, as mentioned above, compensatory mechanisms such as increasing sympathetic tone and cardiac output can be compromised, thereby contributing to IDH. Hemodialysis itself can also induce IDH through mechanisms unrelated to fluid removal, such as electrolyte imbalances such as hypokalemia or hypophosphatemia. These imbalances, which are commonly seen as complications of CKRT, can lead to diminished myocardial performance and arrhythmia [32–34]. In a multivariate analysis of this cohort, predialytic hemodynamic status and underlying liver cirrhosis, as well as hypoalbuminemia, were identified as independent risk factors for subsequent IDH. In maintenance hemodialysis, both low and high predialytic SBPs are considered as risk factors of IDH, which are dependent on the definition of IDH. Low SBP may contribute to the risk of IDH with nadir SBP of <90 mmHg, while high SBP seems to be associated with the risk of IDH with ΔSBP of >20 mmHg. According to the complex association between predialytic SBP and the risk of IDH, recent studies suggest variability in BP and DBP itself as an alternative risk factor of IDH [35,36]. Regarding the AKI condition, research on the risk factor of IDH does not exist. The present study did not show ultrafiltration volume as a risk factor, in conflict with previous studies [37]. Future work should validate these findings, particularly in the AKI condition requiring intermittent hemodialysis.
Although the study provides insightful information, it presents certain limitations. Due to its retrospective design, there may be unaccounted bias and confounders that could have influenced the results. The study did not consider the potential impact of continuous fluctuations in specific biochemical parameters, nor did it account for practice-related alterations, both of which could be correlated with the outcomes. Data on cardiac function such as echocardiography and brain natriuretic peptide, were not available, which would be fruitful to understand the causality between observations. Recovery of kidney function or the transition to acute kidney disease has recently been considered important for outcome [38], but the present study did not depict these factors. Future evaluation of the transition from such a setting to acute kidney disease or ESKD is needed. This study did not categorize nonseptic patients into their specific causes and could not determine the cause of death.
The present study shows that IDH occurring during the initial session in patients undergoing intermittent hemodialysis due to AKI independently contributed to the risk of mortality and subsequent transfer to the ICU. Certain laboratory hemodynamic factors and comorbidities were found to be associated with the occurrence of IDH. These findings lay the groundwork for future studies aimed at elucidating the clinical implications of IDH and developing strategies to prevent its occurrence during the initiation of intermittent hemodialysis in patients with AKI.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









