Status and trends in epidemiologic characteristics of diabetic end-stage renal disease: an analysis of the 2021 Korean Renal Data System
Article information

Abstract
This article provides an update of the trends and characteristics of diabetic kidney disease stage 5D (CKD 5D) patients according to the Korean Renal Data System (KORDS), a nationwide registry database operated by the Korean Society of Nephrology. The KORDS Committee analyzed epidemiologic characteristics of diabetic CKD 5D patients using data from 2001 to 2021 in KORDS. In 2021, the dialysis adequacy of hemodialysis (HD) was lower in diabetic CKD 5D patients than non-diabetic CKD 5D patients, while that of peritoneal dialysis (PD) was similar. Diabetic CKD 5D patients had a higher proportion of cardiac and vascular diseases and were more frequently admitted to hospitals than non-diabetic CKD 5D patients, and the leading cause of death was cardiac disease. From 2001 to 2020, diabetic CKD 5D patients had a higher mortality rate than non-diabetic CKD 5D patients, but in 2021 this trend was reversed. Diabetic PD patients had the highest mortality rate over 20 years. The mortality rate of diabetic HD patients was higher than that of non-diabetic HD patients until 2019 but became lower starting in 2020. There was a decreasing trend in mortality rate in diabetic CKD 5D patients, but cardiac and vascular diseases were still prevalent with frequent admissions to hospitals. More specialized care is needed to improve the clinical outcomes of diabetic CKD 5D patients.
Introduction
Diabetic end-stage renal disease (ESRD) is a serious complication of diabetes mellitus (DM) that affects the quality of life and survival of patients. Diabetic nephropathy is the leading cause of ESRD, accounting for about 50% of all cases in developed countries [1]. The prevalence of DM in South Korea’s overall population continues to rise, with the prevalence rate among adults aged 19 years and older estimated to be 13.9% in 2020 [2]. The Korean Renal Data System (KORDS) is a comprehensive, nationwide registry established by the Korean Society of Nephrology (KSN) in 1985 that systematically collects and maintains data on ESRD patients receiving renal replacement therapy (RRT), chronic kidney disease stage 5D (CKD 5D), in South Korea. KORDS provides valuable information on the epidemiology, management, and outcomes of these patients. KORDS is a valuable resource that provides crucial epidemiological data, insights into treatment patterns and outcomes, informs healthcare policy and planning, promotes quality improvement in renal care, and fosters research collaborations both nationally and internationally. In this study, the Registration Committee of the KSN conducted a comparative analysis of the characteristics of diabetic CKD 5D patients and nondiabetic CKD 5D patients using data from the KORDS registry. The objective of this study was to gain a comprehensive understanding of the current status of patients with diabetic CKD 5D in South Korea to provide insights for frontline healthcare providers and inform healthcare policy-making related to DM and ESRD.
Methods
This study utilized KORDS, a nationwide registry updated on an annual basis [3,4]. To examine trends over time, we conducted a retrospective analysis of 20 years of data (2001 to 2021) for CKD 5D patients enrolled in KORDS. In addition, we utilized the most recent data available from 2021 to provide a current snapshot of the status of CKD 5D patients in Korea. More comprehensive data on KORDS can be found on the KSN website (http://www.ksn.or.kr). The study population comprised CKD 5D patients 19 years of age or older. The following exclusion criteria were applied: 1) Missing data or errors, including cases without dialysis start date or death date or those with death dates preceding the dialysis start date for deceased patients, or cases with enrollment dates preceding the dialysis start date for survivors; 2) Patients with a dialysis start date in 2001 or earlier; and 3) Individuals who had undergone kidney transplantation. The analysis encompassed changes in annual proportions and mortality across all patient groups. Meanwhile, a specific examination of the current status was specifically conducted for the subset of patients who initiated dialysis in the year 2021. Continuous variables are expressed as mean ± standard deviation or median (interquartile range, IQR), while categorical variables are presented as absolute values and percentages. Categorical variables were compared between groups using the chi-square test. Differences between groups for continuous variables were assessed using either a two-tailed Student t test or the Mann-Whitney U test as appropriate. Trends in mortality rates are presented for patients treated each year according to the number of patient-years at risk. Absolute mortality rates were presented per 1,000 person-years of follow-up and adjusted for age and sex. All statistical analyses of survival data were analyzed using R version 4.2.1 (R Foundation for Statistical Computing).
Results
Trends in the prevalence and mortality rates of diabetic CKD 5D patients
Trends in the prevalence of diabetic CKD 5D patients
Over the past two decades, DM has remained the leading cause of ESRD in South Korea. The proportion of diabetic CKD 5D has remained between 46.4% and 51.0% of all CKD 5D patients in the KORDS registry (Fig. 1A).
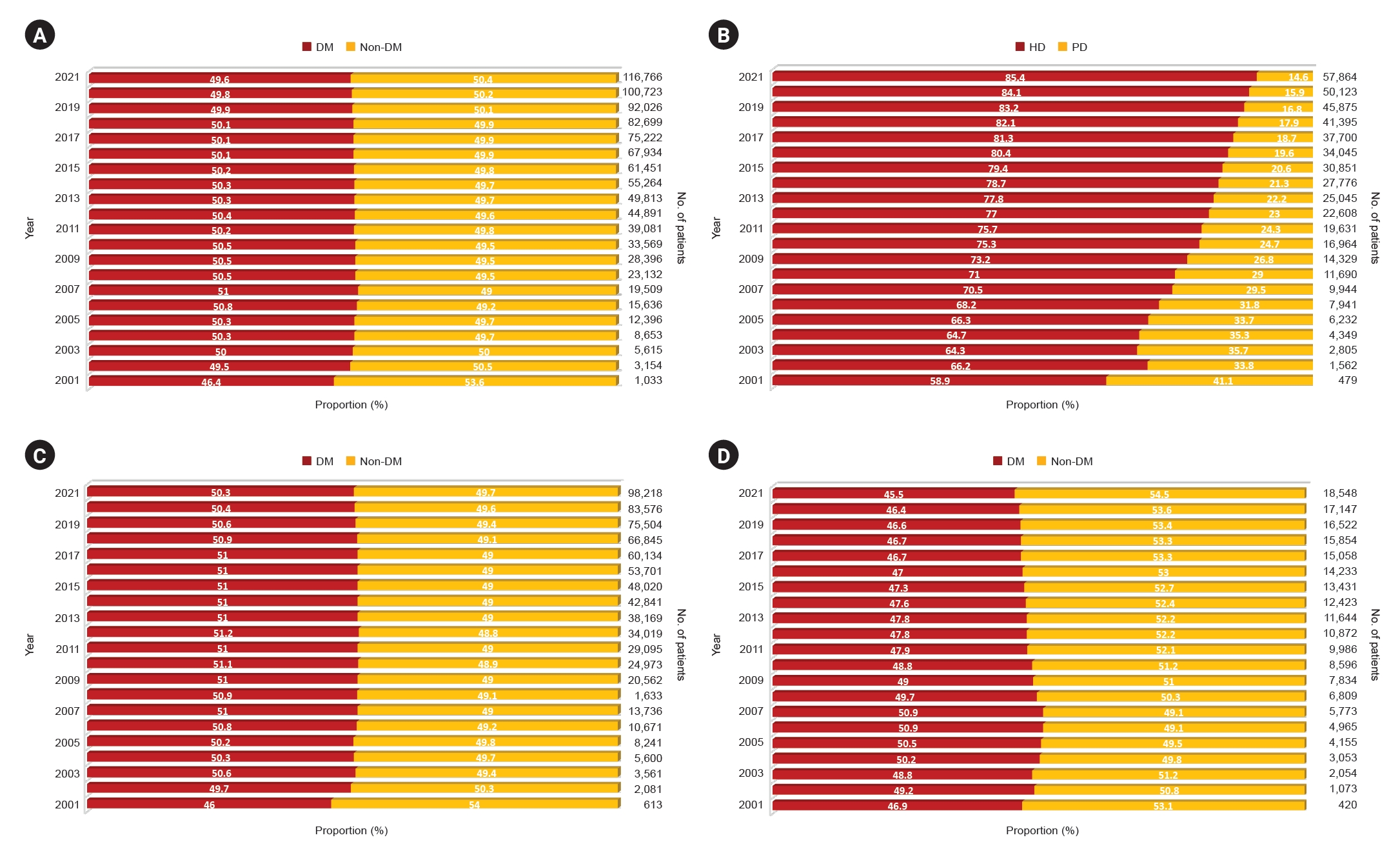
Changes in the proportion of patients with diabetic CKD 5D.
(A) Change in the ratio of patients with diabetic CKD 5D to those with nondiabetic CKD 5D. (B) Change in the proportion of patients with diabetic CKD 5HD vs. CKD 5PD. (C) Change in the ratio of patients with diabetic CKD 5HD to those with nondiabetic CKD 5HD. (D) Change in the ratio of patients with diabetic CKD 5PD to those with nondiabetic CKD 5PD.
CKD 5D, chronic kidney disease stage 5D; CKD 5HD, CKD 5D patients undergoing hemodialysis; CKD 5PD, CKD 5D patients undergoing peritoneal dialysis; DM, diabetes mellitus.
The proportion of CKD 5D patients undergoing hemodialysis (CKD 5HD) has increased, while that of CKD 5D patients undergoing peritoneal dialysis (CKD 5PD) has decreased over 20 years (Fig. 1B). In 2001, over 40% of the total diabetic CKD 5D patient population were on PD. However, there has been a sustained decline in the proportion of patients undergoing PD, resulting in a decrease to less than 15% of diabetic CKD 5PD in 2021 (Fig. 1B). Diabetic CKD 5D patients accounted for about 50% of CKD 5HD patients over 20 years (Fig. 1C). The proportion of diabetic CKD 5D among CKD 5PD patients was over 50% in the mid-2000s, but has slowly declined to around 45% in 2021, whereas the proportion of diabetic CKD 5HD has remained relatively constant (Fig. 1D).
Trends in mortality rates of diabetic CKD 5D patients
Until the year 2020, patients with diabetic CKD 5D had a higher mortality rate than those with nondiabetic CKD 5D. However, in 2021, the mortality rate for nondiabetic CKD 5D patients increased slightly to 41.2 per 1,000 person-years, while the mortality rate for diabetic CKD 5D patients was 40.3 per 1,000 person-years, indicating a narrowing gap between the two groups (Fig. 2A).
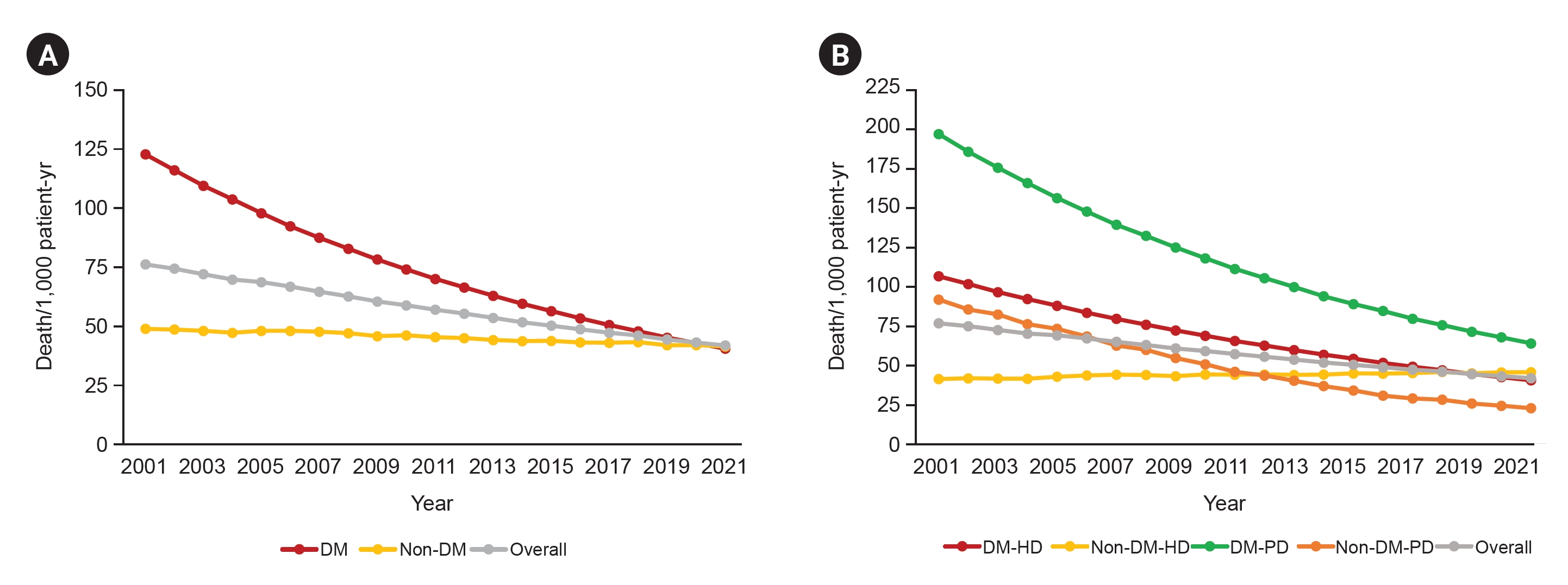
All-cause mortality in patients with diabetic CKD 5D.
(A) Change in mortality rate among patients with diabetic CKD 5D after adjusting for age and sex. (B) Mortality rate changes adjusted for age and sex according to dialysis modality in patients with diabetic CKD 5D.
CKD 5D, chronic kidney disease stage 5D; DM, diabetes mellitus; HD, hemodialysis; PD, peritoneal dialysis.
Since 2001, diabetic CKD 5PD patients have consistently had the highest mortality rate, and since 2013, nondiabetic CKD 5PD patients have had the lowest mortality rate. In the context of CKD 5HD, a consistent decline in the disparity of mortality rates was observed, with a significant turning point occurring in 2019 when the mortality rate for diabetic CKD 5HD patients (44.3/1,000 person-years) fell below that of their nondiabetic counterparts (44.7/1,000 person-years). This discrepancy continued to widen, and by 2021, the diabetic CKD 5HD patients exhibited a mortality rate of 40.3 per 1,000 person-years, while the nondiabetic CKD 5HD patients demonstrated a mortality rate of 45.4 per 1,000 person-years (Fig. 2B).
Age and sex distribution of diabetic CKD 5D patients
Among all CKD 5D patients in the KORDS registry in 2021, diabetic CKD 5D patients aged 60–69 years were the most prevalent (13.3%), followed by those aged 70–79 years (12.9%) and those aged 80 years or more (10.9%), as shown in Fig. 3A. The age distribution was also analyzed in diabetic CKD 5HD and diabetic CKD 5PD patients according to the RRT modality. The age distribution of both diabetic CKD 5HD patients and diabetic CKD 5PD patients showed a similar pattern; aged 60–69 years were most prevalent, followed by those aged 70–79 years and those aged 80 years or more (Supplementary Fig. 1, available online).

Age and sex distribution of diabetic CKD 5D in 2021.
(A) Age distribution of diabetic CKD 5D patients in 2021. (B) Number of patients with diabetic CKD 5D according to age and sex in 2021.
CKD 5D, chronic kidney disease stage 5D.
Upon examination of the age and sex distribution in diabetic CKD 5D patients, the sex distribution was significantly different in age subgroups (p < 0.001). There were more females than males under the age of 30 years with diabetic CKD 5D. However, starting from the 30s, the number of males surpasses that of females, and this difference became particularly significant in the 50s to 70s age group (Fig. 3B).
Status of diabetic CKD 5D patients starting renal replacement therapy in 2021
We analyzed the status of diabetic CKD 5D patients, focusing on incident dialysis patients in 2021.
Characteristics of incident diabetic CKD 5HD patients
Based on the data registered in the 2021 KORDS, the most common type of HD access for both diabetic and nondiabetic CKD 5HD patients was autologous arteriovenous fistula (AVF), followed by central venous catheterization (CVC) and arteriovenous graft (AVG). In nondiabetic CKD 5HD patients, the use of CVC was more prevalent, while in diabetic CKD 5HD patients, a higher proportion of patients utilized AVF and AVG (p < 0.001) (Fig. 4A).
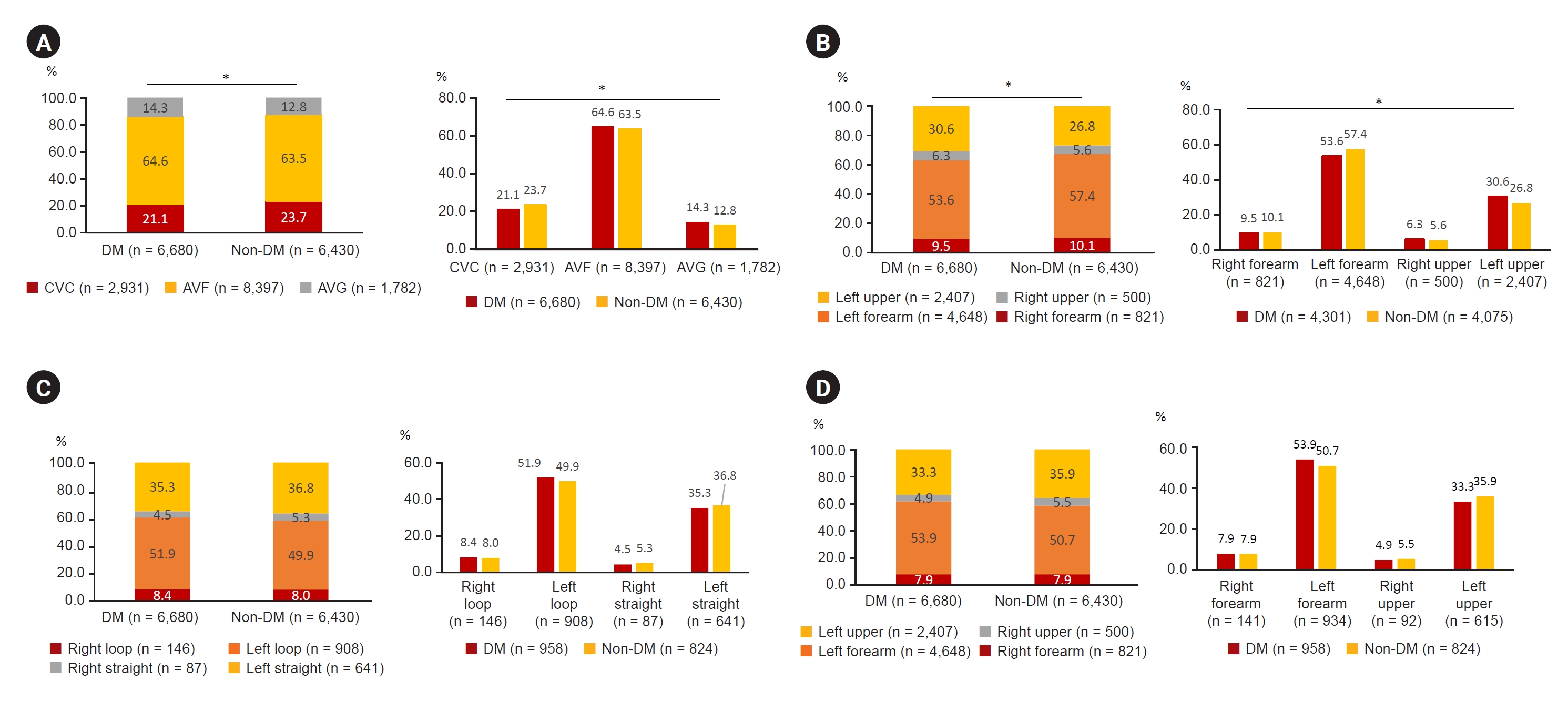
Characteristics of HD access of diabetic CKD 5HD patients.
(A) Types of HD access for diabetic CKD 5HD patients in 2021. (B) Distributions of AVF among diabetic CKD 5HD patients in 2021. (C) Types of AVG among diabetic CKD 5HD patients in 2021. (D) Distributions of AVG among diabetic CKD 5HD patients in 2021.
AVF, arteriovenous fistula; AVG, arteriovenous graft; CKD 5, chronic kidney disease stage 5; CKD 5HD, CKD 5D patients undergoing HD; CVC, central venous catheter; DM, diabetes mellitus; HD, hemodialysis.
*p < 0.05.
AVFs were in the left forearm, left upper arm, right forearm, and right upper arm with decreasing frequency. The rate of AVF placement in the upper arm was significantly higher in diabetic CKD 5HD patients than in nondiabetic CKD 5HD patients (p < 0.001) (Fig. 4B). The most common types of AVGs were, in order of prevalence, left loop, left straight, right loop, and right straight. The prevalence of types of AVG in diabetic and nondiabetic CKD 5HD patients was similar (p = 0.72), as depicted in Fig. 4C. The distribution of AVGs followed the order of left forearm, left upper arm, right forearm, and right upper arm, with similar distribution ratios observed for both diabetic and nondiabetic CKD 5HD patients (p = 0.58) (Fig. 4D).
Supplementary Fig. 2 (available online) provides additional analyses of HD access categorized by DM and sex. The type of HD access was different between diabetic and nondiabetic CKD 5HD male patients (p = 0.041) and female patients (p = 0.002) (Supplementary Fig. 2A, available online). The distribution of AVFs was different between diabetic and nondiabetic CKD 5HD male patients (p = 0.001) and female patients (p = 0.003) (Supplementary Fig. 2B, available online). The type of AVGs showed similar ratios for diabetic and nondiabetic CKD 5HD male (p = 0.13) and female patients (p = 0.50) (Supplementary Fig. 2C, available online). The distribution of AVGs also showed similar ratios for diabetic and nondiabetic CKD 5HD male (p = 0.28) and female patients (p = 0.34) (Supplementary Fig. 2D, available online).
Supplementary Fig. 3 (available online) provides additional analyses of HD access categorized by DM and age subgroups. The type of HD access was statistically different between diabetic and nondiabetic HD patients aged 30–39 years (p = 0.02) and aged ≥80 years (p = 0.009) (Supplementary Fig. 3A, available online). The distribution of AVFs was statistically different between diabetic and nondiabetic HD patients aged 60–69 years (p < 0.001) (Supplementary Fig. 3B, available online). The type and distribution of AVGs showed similar ratios for diabetic and nondiabetic CKD 5HD patients in all age subgroups (Supplementary Fig. 3C, D; available online).
When comparing groups, the diabetic CKD 5HD group exhibited higher systolic blood pressure (median [IQR]: 150.0 [130.0–160.0] vs. 140.0 [130.0–150.0]) and lower diastolic blood pressure (80.0 [70.0–80.0] vs. 80.0 [70.0–83.5]) than the nondiabetic CKD 5HD group (both, p < 0.001). While there were no significant differences in hemoglobin (p = 0.10) or serum phosphorus (p = 0.39) levels between groups, the nondiabetic CKD 5HD group had higher levels of serum albumin (median [IQR]: 3.89 [3.50–4.10] vs. 3.80 [3.50–4.10]), calcium (8.60 [8.10–9.10] vs. 8.50 [8.00–8.90]), and intact parathyroid hormone (PTH) (164.0 [83.3–280.0] vs. 153.7 [82.0–249.9]) than the diabetic CKD 5HD group (all p < 0.001) (Fig. 5A).
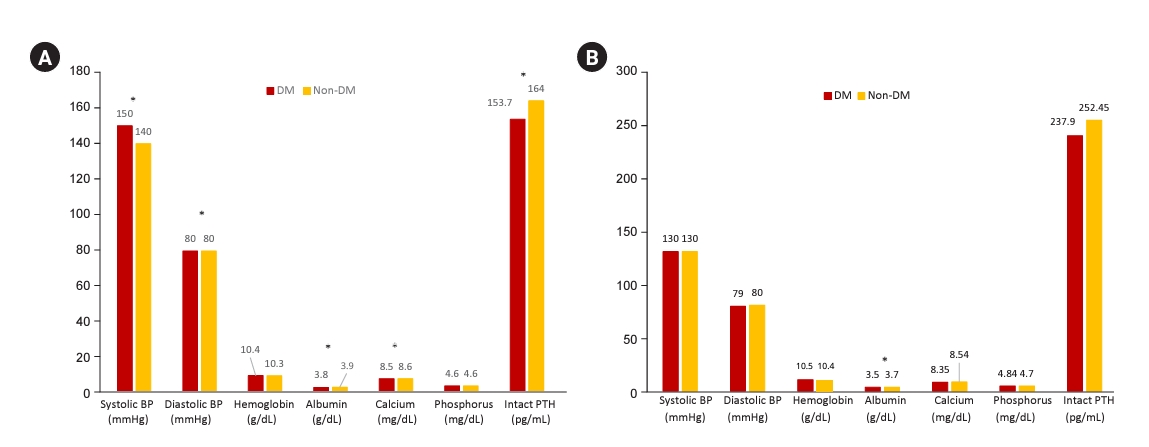
BP and laboratory values in diabetic CKD 5HD and CKD 5PD patients.
(A) Systolic BP, diastolic BP and laboratory parameters in diabetic CKD 5HD patients in 2021. (B) Systolic and diastolic BP and laboratory parameters in diabetic CKD 5PD patients in 2021.
BP, blood pressure; CKD 5D, chronic kidney disease stage 5D; CKD 5HD, CKD 5D patients undergoing hemodialysis; CKD 5PD, CKD 5D patients undergoing peritoneal dialysis; DM, diabetes mellitus; PTH, parathyroid hormone.
*p < 0.05.
Characteristics of incident diabetic CKD 5PD
Based on the data registered in the KORDS in 2021, continuous ambulatory peritoneal dialysis (CAPD) was more frequently used than automated peritoneal dialysis (APD) by both diabetic and nondiabetic CKD 5PD patients. Patients undergoing CAPD were more likely to be nondiabetic, whereas those undergoing APD were more likely to be diabetic (p = 0.03) (Fig. 6A).

Characteristics of diabetic CKD 5PD patients.
(A) PD modality types in diabetic CKD 5PD patients in 2021. (B) Types of PD catheters used in diabetic CKD 5PD patients in 2021. (C) Methods of PD catheter insertion in diabetic CKD 5PD patients in 2021. (D) The exit site infection rate and average incidence of peritonitis per patient and in diabetic CKD 5PD patients in 2021.
APD, automated peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis; CKD 5PD, chronic kidney disease stage 5D patients undergoing peritoneal dialysis; DM, diabetes mellitus; PD, peritoneal dialysis.
*p < 0.05.
Swan neck catheters and a swan neck with a coiled tip were the most common catheters used by diabetic and nondiabetic CKD 5PD patients. More nondiabetic CKD 5PD patients than diabetic CKD 5PD patients had a swan neck catheter (p = 0.03) (Fig. 6B).
In terms of PD catheterization technique, surgical catheterization was the most frequently utilized approach, followed by trocar insertion. When comparing groups, the proportion of surgical insertions was higher in the diabetic CKD 5PD group, whereas the proportion of patients catheterized using a trocar was higher in the nondiabetic CKD 5PD group (p < 0.001) (Fig. 6C).
The rate of exit infections was slightly higher in nondiabetic CKD 5PD patients than diabetic CKD 5PD patients, with an overall rate of 1.6% in diabetic patients and 3.0% in nondiabetic patients (p = 0.007). However, no significant difference was observed in PD-related peritonitis between the two groups (p = 0.142) (Fig. 6D).
Median systolic and diastolic blood pressure, hemoglobin, calcium, phosphorus, and intact PTH levels in the blood did not differ significantly between diabetic and nondiabetic CKD 5PD patients, but serum albumin levels were slightly lower in diabetic CKD 5PD patients than nondiabetic CKD 5PD patients (median [IQR]: 3.50 [3.32–3.90] vs. 3.70 [3.40–4.00], p = 0.049) (Fig. 5B).
Dialysis adequacy in diabetic CKD 5HD and CKD 5PD patients
The distribution of single pooled Kt/V within each group revealed a median of 1.39 (IQR, 1.22–1.58) for diabetic CKD 5HD patients and a median of 1.45 (IQR, 1.25–1.66) for nondiabetic CKD 5HD patients, indicating a statistically significant difference (p < 0.001) (Fig. 7A). In CKD 5PD patients, the median weekly Kt/V, encompassing both urine and dialysate, was 2.15 (IQR, 1.70–2.72) for diabetic CKD 5PD patients and 2.16 (IQR, 1.79–2.69) for nondiabetic CKD 5PD patients, which showed no significant difference (p = 0.86) (Fig. 7B).
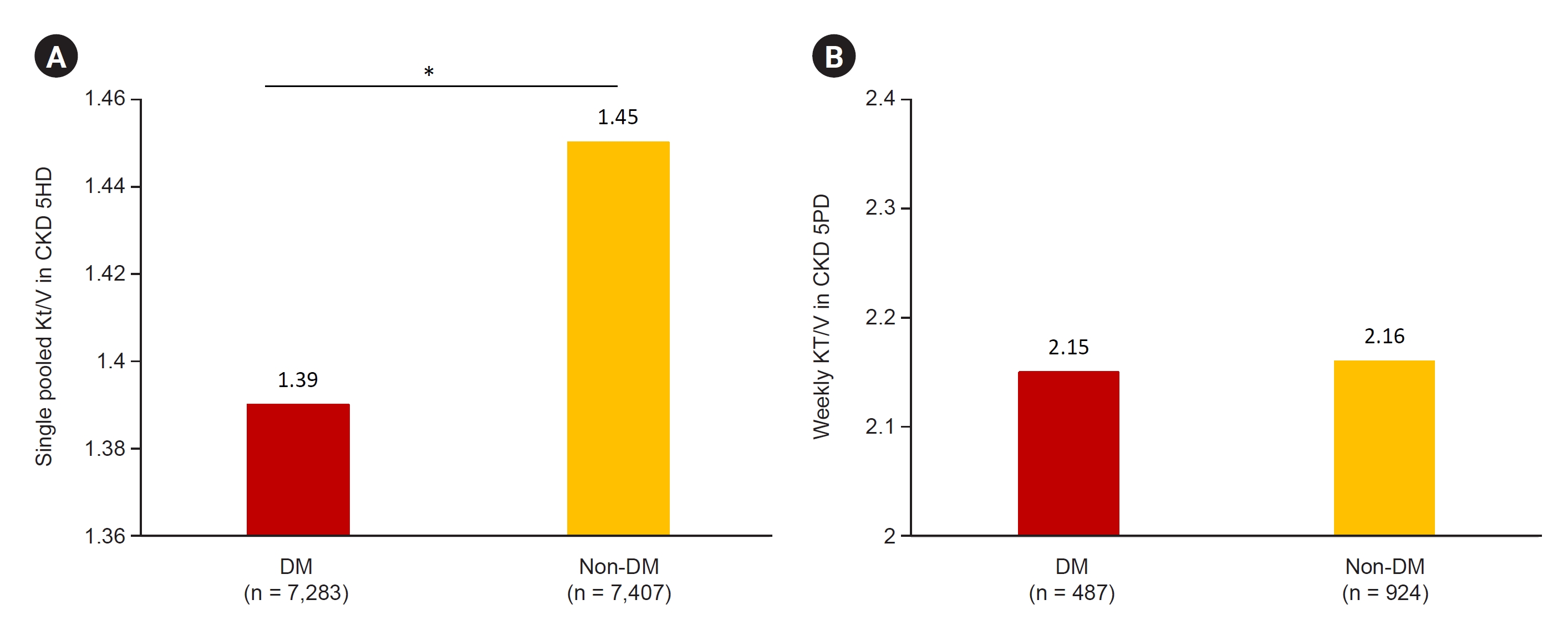
Dialysis adequacy in diabetic CKD 5HD and CKD 5PD patients.
(A) Dialysis adequacy in diabetic CKD 5HD patients in 2021. (B) Dialysis adequacy in diabetic CKD 5PD patients in 2021. *p < 0.05.
CKD 5HD, chronic kidney disease stage 5D patients undergoing hemodialysis; CKD 5PD, chronic kidney disease stage 5D patients undergoing peritoneal dialysis; DM, diabetes mellitus.
*p < 0.05.
Cause of deaths, comorbidities, and hospitalization of diabetic CKD 5D patients
Cause of death of diabetic CKD 5D patients
In 2021, the leading cause of death among all diabetic CKD 5D patients registered in the KORDS was cardiac disease. However, cardiac disease and others that caused death had similar frequencies among nondiabetic CKD 5D patients. The proportion of deaths due to cardiac disease was not different between diabetic and nondiabetic CKD 5D patients (p = 0.23). However, the proportion of deaths due to vascular disease was higher in diabetic CKD 5D patients compared to nondiabetic CKD 5D patients (p = 0.01) (Fig. 8A).
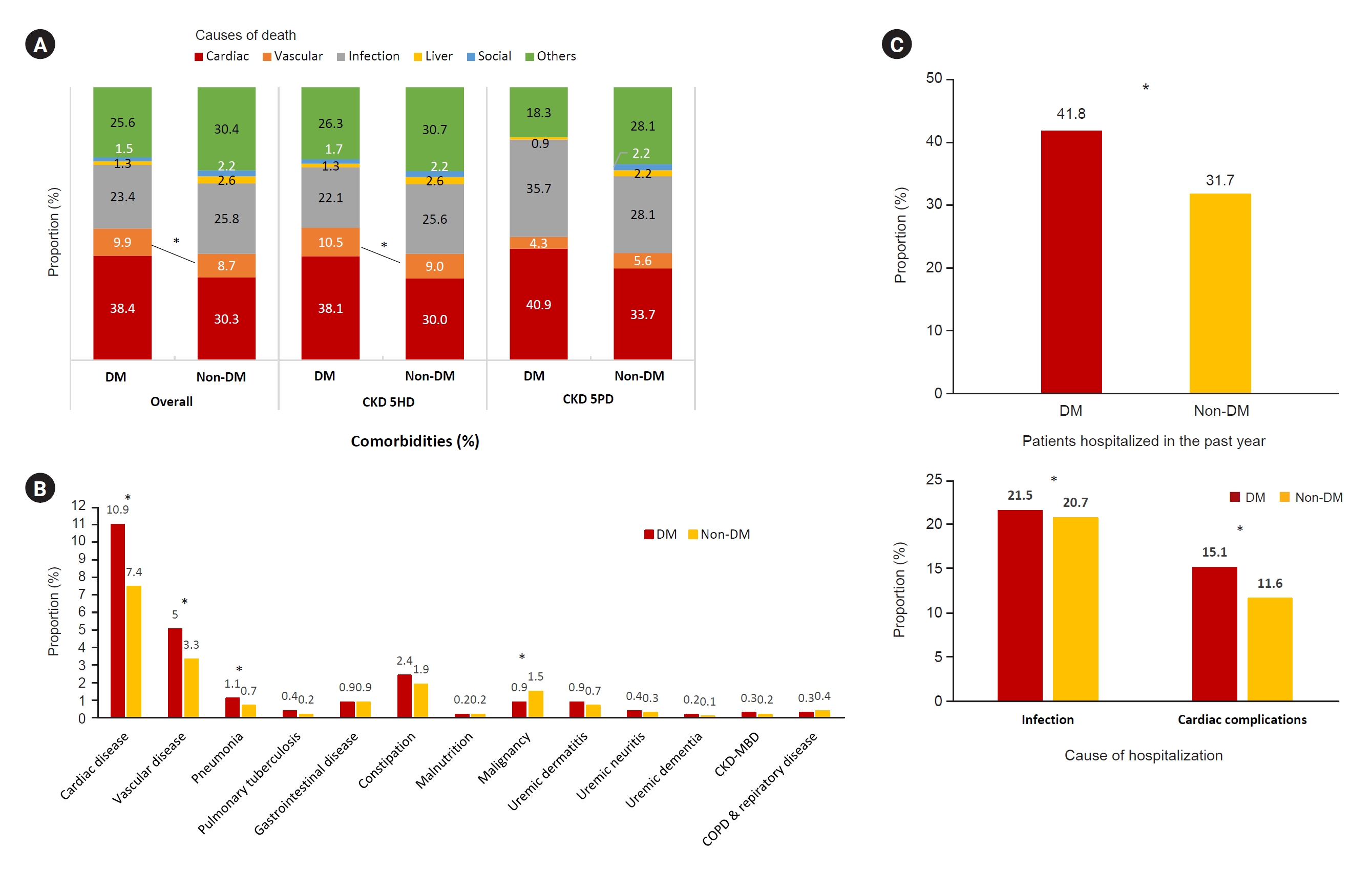
Causes of death, comorbidities, and hospitalization in patients with diabetic CKD 5D.
(A) Causes of death in diabetic CKD 5D patients in 2021. (B) Comorbidities and complications in diabetic CKD 5D patients in 2021. (C) Hospitalization rates and causes of hospitalization in the past year for diabetic CKD 5D patients in 2021.
CKD 5D, chronic kidney disease stage 5D; CKD 5HD, CKD 5D patients undergoing hemodialysis; CKD 5PD, CKD 5D patients undergoing peritoneal dialysis; CKD-MBD, chronic kidney disease-mineral bone disorder; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HD, hemodialysis; PD, peritoneal dialysis.
*p < 0.05.
The proportions of cause of deaths were also analyzed by RRT modality (Fig. 8A). Among CKD 5HD patients, the proportion of deaths attributed to cardiac disease was not statistically different between diabetic and nondiabetic patients (p = 0.23). However, diabetic CKD 5HD patients had a higher mortality rate due to vascular disease than nondiabetic CKD 5HD patients (p = 0.006). Among CKD 5PD patients, the proportion of deaths attributed to cardiac disease, vascular disease, and infection was not statistically different between diabetic and nondiabetic patients (p = 0.92, p = 0.72, and p = 0.36, respectively). No significant differences were observed between diabetic and nondiabetic patients in CKD 5HD or CKD 5PD groups for other causes of deaths.
Comorbidities and hospitalization in diabetic CKD 5D patients
Cardiac disease was the most prevalent comorbidity in both diabetic and nondiabetic CKD 5D patients, followed by vascular disease. The prevalence of cardiac and vascular disease was higher in diabetic CKD 5D patients than nondiabetic CKD 5D patients (both p < 0.001) (Fig. 8B). The prevalence of pneumonia was higher (p = 0.02), while that of malignancy was lower (p < 0.001) in diabetic CKD 5D patients than nondiabetic CKD 5D patients.
Furthermore, the rate of hospitalization within the past year for diabetic CKD 5D patients was higher at 41.8% compared to 31.7% for nondiabetic CKD 5D patients (p < 0.001). The proportions of infection and cardiac disease as the cause of hospitalization were both higher for diabetic CKD 5D patients compared to nondiabetic CKD 5D patients (both p < 0.001) (Fig. 8C).
Discussion
Based on our analysis of the KORDS data from 2001 to 2021, we present several key findings regarding diabetic CKD 5D in Korea.
First, diabetic CKD 5D remains the most common cause of CKD 5D in Korea, accounting for approximately 50% of cases over the past 20 years. This finding is consistent with the global trend, where DM has been identified as the leading cause of ESRD.
Second, the proportion of diabetic CKD 5PD patients has decreased over the past 20 years from approximately 41.1% in 2001 to less than 14.6% in 2021. This trend is likely due to various factors including changes in clinical practice, provider or patient preferences, and accessibility to different dialysis modalities. Studies have discussed factors influencing the choice of PD in diabetic CKD 5D patients, such as potential impact on glycemic control, risk of peritonitis, and comorbidities that could complicate treatment [5–11]. Considering the high cardiovascular mortality and potential dialysis-induced cardiac injury associated with HD [12], PD remains a viable alternative. Our analysis indicates that nondiabetic CKD 5PD patients exhibited lower mortality rates than those who received HD, with the former subgroup displaying the lowest mortality rate among all analyzed groups. Consequently, optimal patient selection and effective management of PD may result in superior outcomes for diabetic CKD 5D patients relative to HD, emphasizing the importance of shared decision-making [13] between healthcare providers and patients when selecting the most appropriate RRT modality [14–17]. Nonetheless, further efforts are imperative to improve the survival outcomes of diabetic CKD 5PD, as this subgroup continues to exhibit the highest mortality rate among the four groups.
Third, diabetic CKD 5D patients were found to have a higher prevalence of comorbid cardiac and vascular diseases and a higher rate of hospitalization than nondiabetic ESRD patients. The greater prevalence of comorbidities and prior cardiovascular events in diabetic patients prior to initiating dialysis may account for this increased risk [18]. This underscores the importance of comprehensive management of diabetic CKD 5D patients, including control of cardiovascular risk factors and timely intervention for complications.
Fourth, dialysis adequacy differed between diabetic and nondiabetic CKD 5D patients. Specifically, diabetic CKD 5HD patients had lower dialysis adequacy than nondiabetic CKD 5HD patients, whereas there was no significant difference in dialysis adequacy between diabetic and nondiabetic CKD 5PD patients. Multiple factors may be involved in the difference, including comorbidities, access problems, or residual renal function, but the reason is unclear because of limited data. Clinical practice guidelines recommend maintaining a Kt/V level above 1.4 due to the association between lower values and increased morbidity in CKD 5HD patients [19,20]. In this study, the median Kt/V of diabetic CKD 5HD patients was 1.39. This finding suggests that a significant proportion of patients may have Kt/V levels below the recommended threshold, given that this value represents only the median value for the study population. Therefore, active management of these patients is necessary to improve survival rates and address gaps in outcomes.
Lastly, it is promising to observe that the mortality for patients with diabetic CKD 5D, adjusted for age and sex, has decreased continuously over the last two decades, ultimately achieving parity in 2021 with nondiabetic CKD 5D patients. Nevertheless, when analyzed by RRT modality, it is evident that diabetic CKD 5PD patients still have the highest mortality rate, while nondiabetic CKD 5PD patients have the lowest mortality rate. Based on these observations, it appears that the primary underlying cause of death among patients with diabetic CKD 5D is DM itself rather than the PD modality itself. This suggests that there is a significant unmet need in addressing the impact of DM on outcomes in this patient population.
In conclusion, analysis of the KORDS registry data provided valuable insights into the epidemiologic characteristics of diabetic CKD 5D in Korea. There was a decreasing trend in mortality rate in diabetic CKD 5D patients, but cardiac and vascular diseases remained prevalent in diabetic CKD 5D patients in addition to frequent hospital admissions. More specialized care is needed to improve the clinical outcomes of diabetic CKD 5D patients. Further research to elucidate the factors contributing to the observed trends and to develop effective strategies for the prevention and management of diabetic CKD 5D is warranted.
Supplementary Materials
Supplementary data are available at Kidney Research and Clinical Practice online (https://doi.org/10.23876/j.krcp.23.130).
Acknowledgements
The ESRD Registry Committee of the KSN thanks all the medical doctors and nurses of the dialysis centers in Korea for participating in this registry.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Funding
This research was supported by a cooperative research fund from the Korean Society of Nephrology (2022).
Data sharing statement
The data presented in this study are available upon reasonable request from the corresponding author.
Authors’ contributions
Conceptualization: YKK, HEY
Data curation, Formal analysis: SAJ
Funding acquisition, Methodology: HEY
Investigation: KMK, THB, YAH, SDH, SRC, HL, JHK, SHK, THK, HSK, CYY, KK, SHA, HEY
Writing–original draft: KMK, HEY
Writing–review & editing: THB, YAH, SDH, SRC, HL, JHK, SHK, THK, HSK, CYY, KK, SHA, YKK
All authors read and approved the final manuscript.