



Introduction
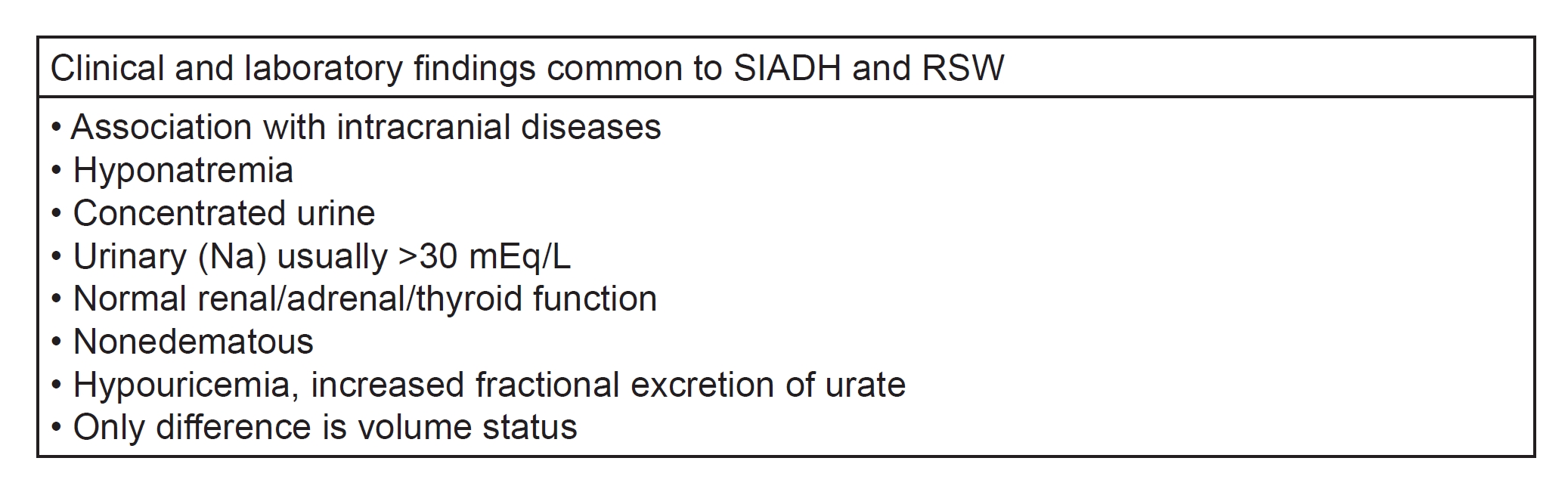
The reported high prevalence of renal salt wasting (RSW) without clinical evidence of cerebral disease has created an urgency to change the nomenclature of this syndrome from cerebral salt wasting (CSW) to RSW [1,2]. This change in nomenclature goes beyond its scientific accuracy because the absence of clinical evidence of cerebral disease would perpetuate the inappropriate water restriction of these volume-depleted patients with RSW, who were erroneously misdiagnosed as being water-logged by the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) [2]. Inappropriate water restriction of volume-depleted patients with RSW was common because CSW or more appropriately RSW, was considered to be nonexistent or very rare by internists despite its perception as being common among neurosurgeons, neurologists, and critical care physicians. The high prevalence of RSW without clinical evidence of cerebral disease supports our proposal to change CSW to RSW, which will be used throughout this manuscript [2]. However, differentiating SIADH from RSW has been elusive in part because of the perceived rarity of CSW and failure to address the identical clinical parameters that are shared by SIADH and RSW. Both syndromes present with hyponatremia; hypouricemia with high fractional excretion (FE) of uric acid; normal renal, adrenal, and thyroid function; concentrated urine where urine osmolality (Uosm) is higher than plasma osmolality; and urine sodium concentration (UNa) usually >30 mmol/L (Fig. 1).
The reported high prevalence of RSW raises valid questions of publications where the diagnosis of SIADH is on the basis of these identical clinical parameters without attempting to resolve the difficult task of differentiating SIADH from RSW. We will discuss the historical evolution of the controversy over the existence and prevalence of RSW; the ineffectiveness of the volume approach to identify the different causes of hyponatremia and hyponatremia-related diseases; the development of a new pathophysiologic approach that improved the identification of the different causes of hyponatremia; how the natriuretic factor, haptoglobin-related protein without signal peptide (HPRWSP), was identified; the development of HPRWSP as a biomarker for first encounter diagnosis of RSW to improve clinical outcomes; introduce a new syndrome of RSW in Alzheimer disease (AD); present two very instructive cases, discuss some of the clinical applications of HPRWSP and finally clarify some of the controversy over the existence and prevalence of RSW.
Historical evolution of cerebral salt wasting from being nonexistent, rare to common: failure of volume approach
CSW had an inauspicious beginning as previously discussed because the three hyponatremic patients in the first report of salt wasting with cerebral diseases failed to prove salt wasting in 1950 [3,4]. When the seminal study on SIADH was first published in 1957, the ability to diagnose SIADH without the ability to determine plasma antidiuretic hormone levels by equating their findings to studies of SIADH induced in normal subjects by daily injections of arginine vasopressin rightfully captured the respect and admiration of the medical community [5,6]. They demonstrated that a hyponatremic patient with concentrated urine and high UNa was consistent with SIADH and not RSW by critically determining increased extracellular volume by the sulfate space [5]. SIADH has since been regarded as a major cause of hyponatremia in nonedematous hyponatremic patients. This dominance of SIADH persisted, in part, because the evaluation of hyponatremic patients utilized an approach that had little or no credibility by categorizing hyponatremic patients according to the state of their extracellular volume. This volume approach persisted despite our awareness that we cannot accurately determine the volume status of patients by usual clinical criteria [7,8]. Moreover, SIADH was erroneously designated as a form of euvolemic hyponatremia, despite studies demonstrating them to be consistently hypervolemic [5,9ŌĆō11].
Pathophysiologic approach to evaluate hyponatremia and hyponatremia-related patients
It is clear that the volume approach and prevailing controversies need to be reassessed by methods that will rapidly differentiate SIADH from RSW and vastly improve clinical outcomes. We developed and tested a new pathophysiologic approach over a 30-year period that has the potential to improve our understanding and treatment of hyponatremic and hyponatremia-related diseases, defined as normonatremic patients with RSW who will develop hyponatremia if they increased water intake.
Fractional excretion rates of urate to identify causes of hyponatremia
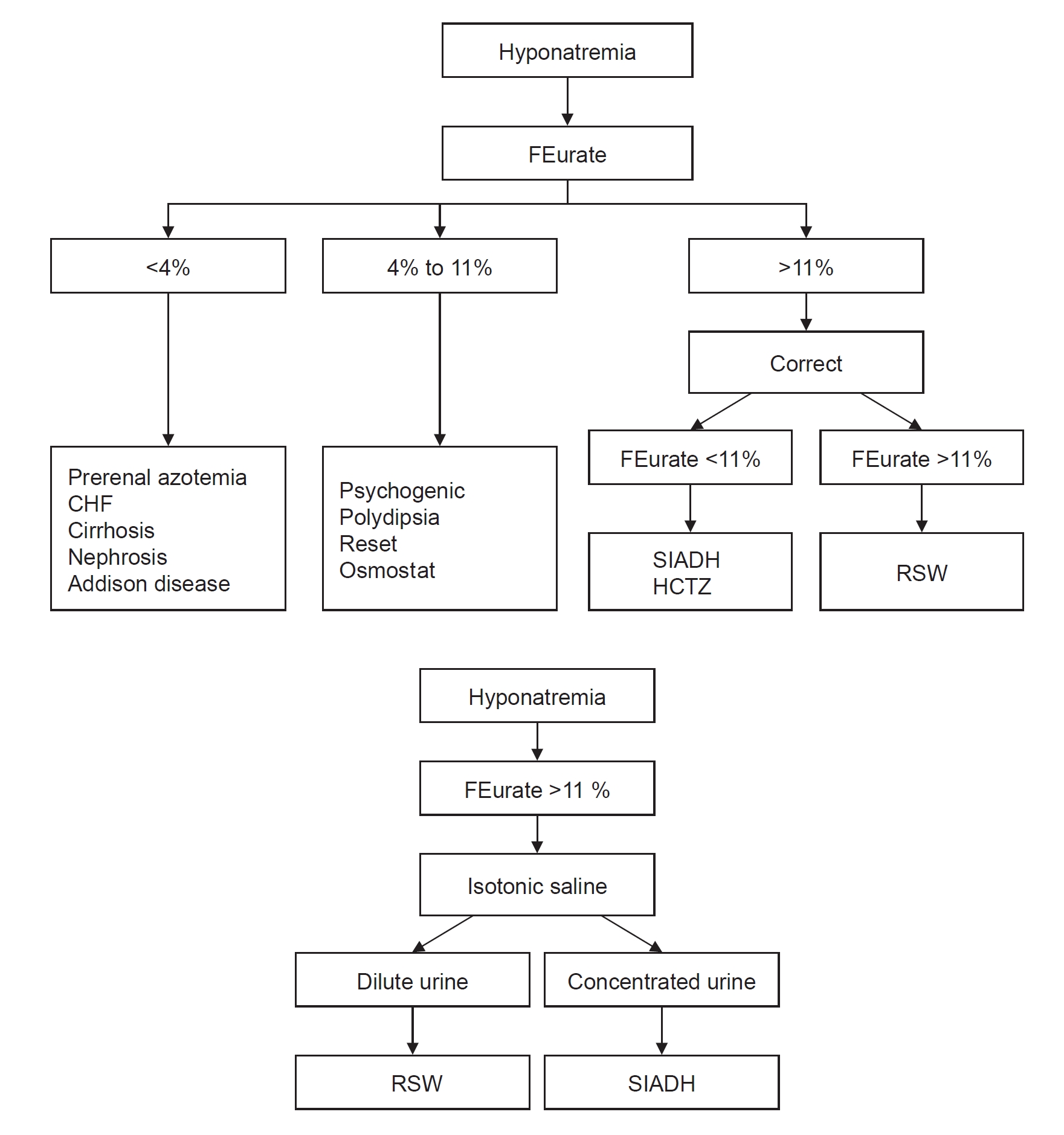
Urate is freely filtered at the glomerulus and is transported exclusively in the proximal tubule by reabsorbing and secretory transporters where there is a net reabsorption of 89% to 96% of the filtered load or 4% to 11% excretion of the filtered load that is referred to as FE of urate (FEurate) [1,12]. There is an expanding literature on the contribution of determining FEurate to identify the different causes of hyponatremia and hyponatremia-related diseases. FEurate has been especially useful in identifying patients with a reset osmostat (RO), Addison disease, SIADH, and RSW [13,14]. FEurate can also differentiate SIADH from RSW by its unique relationship to serum sodium. The increased FEurate that is >11% will decrease to a normal range of 4% to 11% in SIADH as compared to being persistently increased in RSW after correction of the hyponatremia (Fig. 2) [1,9,15ŌĆō20]. Determinations of FEurate have effectively identified many causes of hyponatremia but need to be further investigated, especially psychotropic drugs that induce hyponatremia by an upregulation of the V2 receptor to ADH, which may thus induce an SIADH-like effect on FEurate as noted with hydrochlorothiazide [21,22].
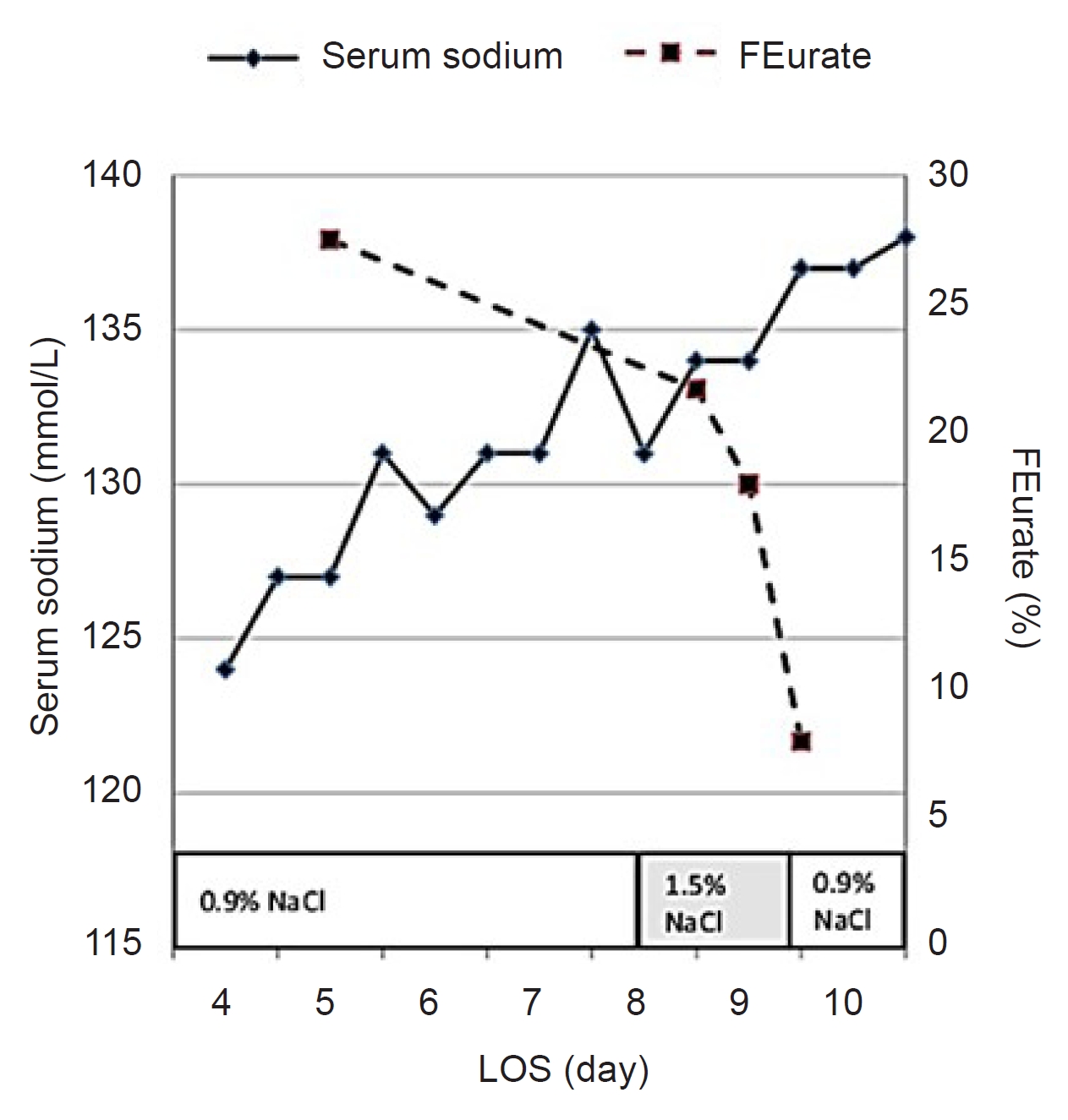
The effect of saline on FEurate has become an issue in the recent debate over the existence of RSW, which contested our proposal that saline has a meager effect on FEurate [23]. They cite an increase in FEurate to 18.7% after receiving an extremely large amount of hypertonic saline that increased FENa sodium to an incredibly high 14.5% which may be almost impossible to attain in any clinical setting [24]. They failed to cite a more appropriate study where isotonic saline increased FENa sodium from 1.04% to 4.43% and FEurate from 7.98% to only 9.76% [25]. The highest FENa sodium we achieved while volume repleting a salt wasting patient with isotonic saline was 2.86% when FEurate was 49% [20]. Further insight into the effect of isotonic saline infusions on FEurate can be appreciated by a study in which we failed to correct the hyponatremia in a patient suspected of having RSW after infusing large volumes of isotonic saline with a baseline FEurate of 28%. We corrected the hyponatremia by infusing 1.5% hypertonic saline and demonstrated a progressive reduction in FEurate to 7% (Fig. 3) [13]. It, thus, appears that isotonic saline infusions only modestly increase FEurate to levels that do not come close to levels seen in RSW or SIADH. As will be discussed later, volume depletion can significantly reduce FEurate induced by extracellular volume depletion or a uricosuric agent.
Effect of isotonic saline on urine osmolality and serum sodium in syndrome of inappropriate secretion of antidiuretic hormone and renal salt wasting
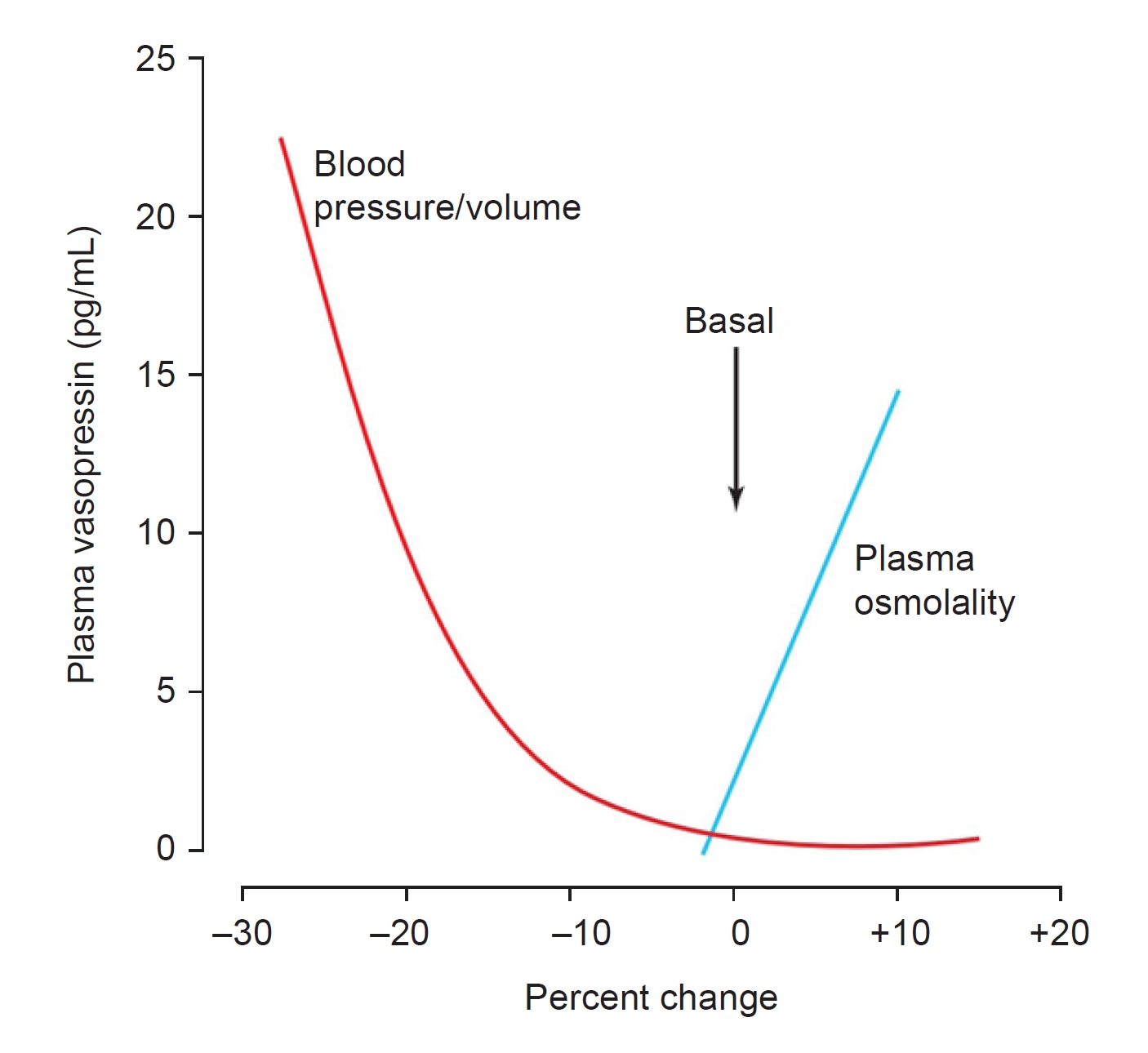
The effect of isotonic saline infusions on Uosm and serum sodium concentration has well-established physiologic explanations that can differentiate SIADH from RSW. The response is based on the unresponsiveness or inappropriateness of ADH response to osmolar or volume stimuli in SIADH as compared to an appropriate response to both stimuli in RSW. The ADH response in RSW follows the principle that the volume stimulus for ADH secretion is more potent than the osmolar stimulus (Fig. 4) [26]. ADH levels will thus remain increased as long as the patient is volume-depleted, but when the volume stimulus is removed by infusing isotonic saline, the coexistent hypo-osmolality will inhibit ADH secretion, excrete dilute urines and correct the hyponatremia [1,9,20]. We decided to infuse isotonic saline to determine its effects on Uosm and serum sodium concentrations. Because of the difficulty in differentiating SIADH from RSW, we determined blood volume studies by radioisotope dilution methods using 51 chromium-labeled red blood cells and radioiodinated serum albumin and plasma renin and aldosterone to levels to ascertain that we were indeed studying cases of SIADH and RSW.
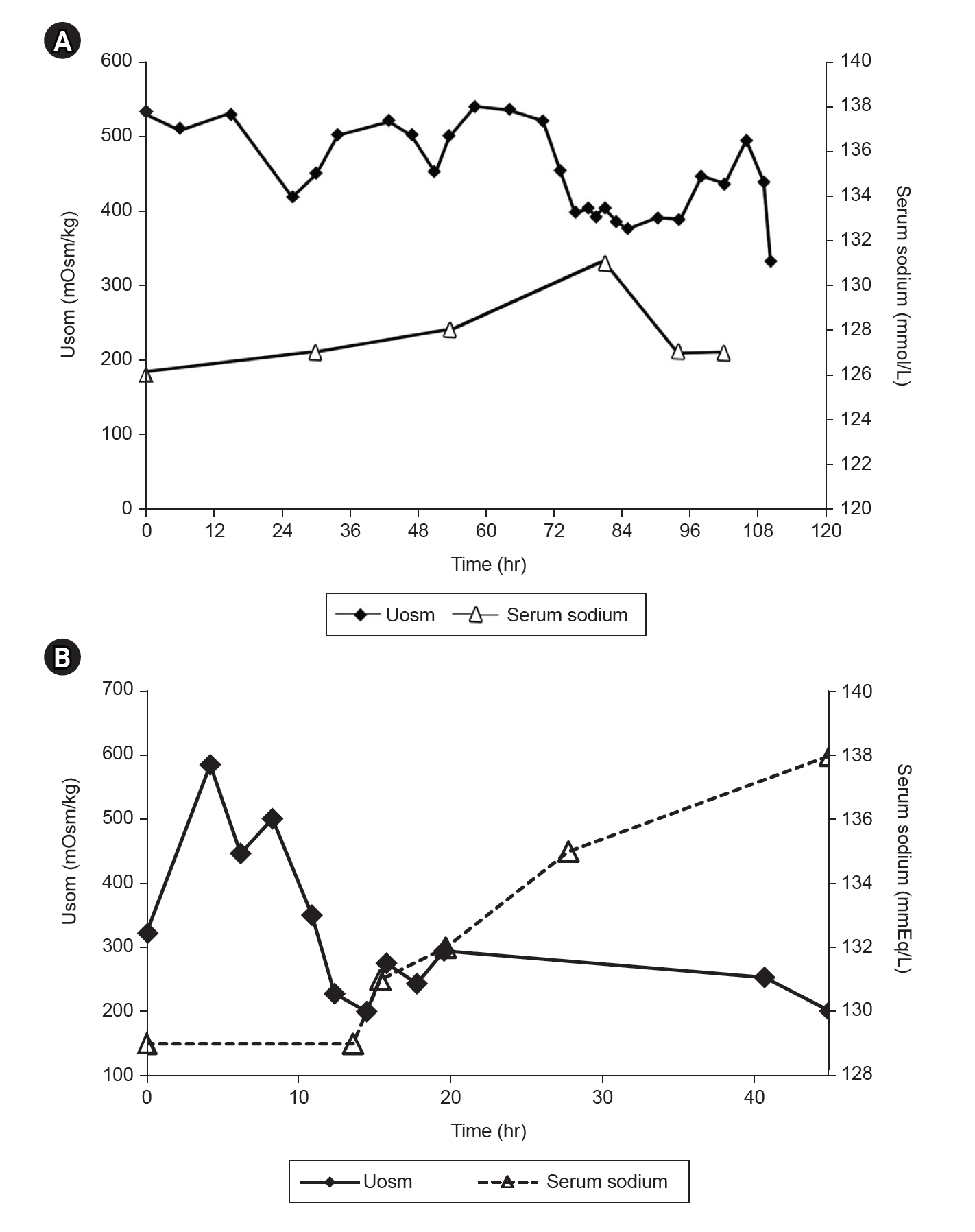
Two unequivocal cases of SIADH had increased blood volume and decreased plasma renin and aldosterone levels and one with RSW had decreased blood volume and increased plasma renin and aldosterone levels [19,20]. As noted in Fig. 5A, Isotonic saline failed to dilute the urine or correct the hyponatremia in the two patients with increased blood volume and reduced plasma renin and aldosterone levels as seen in SIADH [9]. In the patient with RSW, isotonic saline diluted the urine to 151 mOsm/kg 13 hours after initiation of isotonic saline infusions when plasma ADH was undetectable (Fig. 5B) [20]. We present this patient who provided valuable insights into RSW by virtue of the certainty with which the diagnosis of RSW was made and the credibility of the physiologic outcomes and unusual findings that were noted [20].
This is a 76-year-old female who was admitted with a hip fracture without clinical evidence of cerebral disease. A diagnosis of SIADH was made and she was water-restricted to 750 mL/day for 10 days without correction of her hyponatremia. She was referred to nephrology for further evaluation. At the time she was seen by nephrology, she had a serum sodium of 129 mmol/L, uric acid of 3.4 mg/dL, creatinine of 0.8 mg/dL, plasma renin of 8.63 ng/mL/hr, aldosterone of 16.5 ng/dL, atrial natriuretic peptide (ANP) of only 35 pg/dL, normal thyroid and adrenal function, Uosm of 321 mOsm/kg, UNa of only 6 mmol/L and FEurate of 29.6%. Her baseline blood volume as determined by 51 chromium-labeled red blood cells and radioiodinated serum album revealed a 7% reduction in blood volume. She was then infused with isotonic saline at a rate of 125 mL/hr and every urine was collected separately for the following 48 hours. As noted in Fig. 5B, Uosm increased from a baseline of 321 to 690 mOsm/kg and gradually decreased to a nadir of 151 mOsm/kg with a gradual increase in serum sodium to 138 mOsm/L 48 hours after initiation of isotonic saline infusion. Sixteen hours after initiating isotonic saline infusion, she awoke feeling much better and was very hungry. Because of the certainty of the diagnosis of RSW, there are many messages that characterize RSW and the physiology associated with the results obtained.
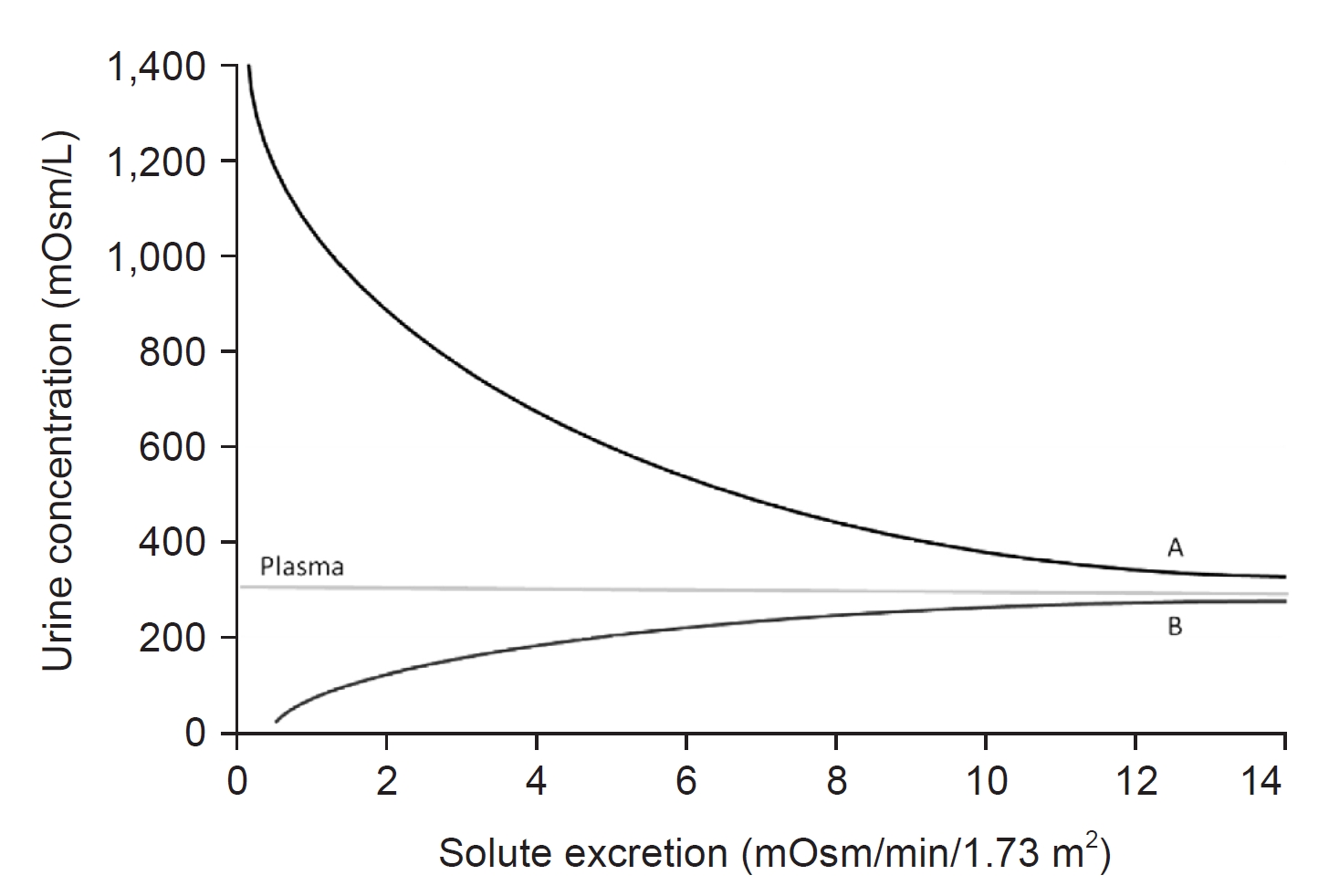
1. Isotonic saline removed the more potent volume stimulus to permit the hypo-osmolality to inhibit ADH secretion to a point where ADH was undetectable when the urine was diluted at 151 mOsm/kg. Because a dilute urine signified the removal of pure water from the body, serum sodium normalized to 138 mmol/L 48 hours after initiation of isotonic saline infusion. These data have been challenged in the recent debate on RSW claiming that the Uosm of 151 mOsm/kg did not attain a maximum dilution of 50 mOsm/kg, suggesting that ADH was still present in the plasma and not undetectable as reported [23]. This is correct in a normal subject, but this is precisely what you would expect in a patient with RSW. The Uosm of 151 mOsm/kg in the absence of ADH is consistent with the dictum that patients with RSW have a free water clearing defect. This is best explained by the infusion of hypotonic saline to normal subjects after they had attained the minimum Uosm of 50 mOsm/kg by ingesting water (Fig. 6). The hypo-osmolality of the hypotonic saline maintained ADH at a suppressed level throughout the study as the infusion of hypotonic saline increased extracellular volume and increased urinary sodium or solute excretion. As solute excretion increased with the continued infusion of hypotonic saline, Uosm progressively increased to levels approaching plasma osmolality in the absence of ADH (Fig. 6). Since the excretion of free water represents solute-free water, the progressive increase in solute excretion or osmolar clearance will progressively increase Uosm to approach plasma osmolality (Fig. 6) [27].
2. As noted in the two unequivocal cases of SIADH, isotonic saline infusion does not dilute urine or correct the hyponatremia in SIADH.
3. The UNa at baseline of only 6 mmol/L is considered to be inconsistent with RSW or SIADH but its presence in this case of RSW can be explained by the low salt intake by loss of appetite while being water restricted for an erroneous diagnosis of SIADH for 10 days. The reader is encouraged to read about the concept of escape in different clinical situations [28]. There are two phases in RSW. The first is the initiation phase where sodium excretion exceeds sodium intake to create a volume-depleted state. The patient then transitions to the equilibrated state where sodium input equals sodium output by undergoing hormonal, hemodynamic, and neural adjustments [28]. Resolution of the initiation phase must occur at some point because a daily output of sodium exceeding salt intake will otherwise lead to the total removal of all exchangeable sodium from the body. We have called this transition from the initiation to the equilibrated state as RSW escape because all exchangeable sodium would be eliminated from the body if there is no escape from the initiation phase. Mineralocorticoid escape has been a perfect counterpart of the escape phenomenon [29]. The patient must have been in the equilibrated stage when first seen by nephrology [28].
4. The low sodium intake must have reduced medullary sodium content to diminish the ability to concentrate the urine despite high levels of ADH with a baseline Uosm of 321 mOsm/kg. Infusion of isotonic saline rapidly increased sodium delivery to the distal tubules because of a major defect in proximal tubule sodium transport as will be discussed later. This rapid delivery of sodium to the distal tubule increased medullary sodium content or strengthened the medullary concentrating ability to increase Uosm to 690 mOsm/kg (Fig. 5B).
5. The baseline FEurate of 29.6% while in a volume-depleted state increased progressively to 64% after initiation of isotonic saline, suggesting that the volume depletion had decreased the effect of the uricosuric factor in plasma to reduce FEurate. Isotonic saline increased the effectiveness of the uricosuric factor to increase FEurate further in RSW as compared to a meager effect of infusing isotonic saline on FEurate in a normal euvolemic patient as noted earlier [25].
6. The ANP of a low normal 35 pg/mL is an unlikely cause of RSW as proposed in a number of publications. As will be discussed later, the physiology of the identified protein, HPRWSP, has vastly different physiologic effects that essentially rule out ANP as a possible cause of RSW [1,30,31].
7. Potassium excretion has been proposed to increase significantly during the period of volume repletion by infusion of isotonic saline. This would be expected because potassium secretion in the distal nephron is influenced by the delivery of sodium, water, and anions. Contrary to this proposal, potassium excretion actually decreased from what was observed at baseline [20]. This difference in potassium excretion might be explained by the higher baseline renin and aldosterone levels that decreased while being volume-repleted, suggesting that aldosterone plays a major role in the handling of potassium by the kidneys.
8. The absence of cerebral disease in this patient is one of many RSW patients without clinical evidence of cerebral disease. Based on these and subsequent supporting data, we advocate changing cerebral to RSW, a very important change in nomenclature [2].
There are ample data to conclude that isotonic saline does not induce excretion of dilute urines or correct the hyponatremia in SIADH. In contrast, isotonic saline infusion in RSW eliminated the more potent volume stimulus and permitted the coexisting hypo-osmolality to inhibit ADH secretion, induce the excretion of dilute urines and correct the hyponatremia in RSW [26]. These data in SIADH are consistent with comments made by Bartter and Schwartz [32], ŌĆ£a striking and consistent finding in patients with SIADH is the persistence of hyponatremia even when large quantities of sodium are administeredŌĆØ or by Janicic and Verbalis [33] who state that ŌĆ£volume expansion does not correct the hyponatremiaŌĆØ in SIADH. Verbalis [34] also presented a case of SIADH who was misdiagnosed as having CSW when the hyponatremia did not respond to isotonic saline but corrected the hyponatremia by water restriction. In addressing the controversy over the existence and prevalence of RSW, there are two editorials that comment on the rarity of RSW by citing studies of questionable credibility on the hyponatremia associated with subarachnoid hemorrhage (SAH) [34,35]. Both editorials cite retrospective and prospective studies by a single group. The credibility of the retrospective study was severely damaged by proposing that 4.8% had a combination of SIADH and RSW in the same patient without defining how they arrived at such an unlikely diagnosis [36]. In the prospective study of 49 hyponatremic patients with SAH, the diagnosis of SIADH met the criteria included in Fig. 1 without attempting to differentiate it from RSW. All 49 patients corrected their hyponatremia in a median of 3 days while on isotonic saline infusions without ever being water restricted, receiving hypertonic saline or the ADH V2 receptor inhibitor. These 49 patients had RSW and not SIADH as suggested by these authors and both editorials [34,35,37]. As a final comment, none of the criticisms about the existence and prevalence of RSW questioned the validity of our pathophysiologic approach or provided data to prove them to be wrong [23,34,35,38].
Because patients with SAH were often misdiagnosed as having SIADH, there was an increase in ischemia and brain infarction with increased morbidity and mortality when water was restricted [39]. The infusion of isotonic saline has, thus, become the standard of care for patients with SAH. As a result of this paradigm shift, we can expect to see less hyponatremia in these patients because patients must have sufficient water intake to induce hyponatremia unless they are undergoing desalination where UNa far exceeds the intake sodium concentration [40]. Water intake must substantially exceed the insensible water losses of approximately 500 mL that occur daily. This was exemplified by the early studies on the effects of daily pitressin injections on normal humans and dogs where hyponatremia was only possible when they increased water intake [6,41].
Pathophysiologic approach uncovers the high prevalence of renal salt wasting without cerebral disease
Determinations of FEurate and response to isotonic saline infusions in 62 hyponatremic patients in the general medical wards of the hospital unexpectedly found RSW to be much more common than previously perceived [1].
1. Seventeen (27%) had SIADH. Isotonic saline infusion did not dilute or correct the hyponatremia in 11 patients. High baseline FEurate normalized to <11% in five patients after correction of their hyponatremia.
2. Nineteen (31%) had a RO. All 19 patients had a normal FEurate of 4% to 11% with eight excreting a spontaneously excreted dilute urine.
3. Twenty-four (38%) had RSW. Isotonic saline infusions induced the excretion of dilute urine in 19 patients with two having undetectable plasma ADH levels when the urine was diluted. Ten patients who excreted dilute urines received 5% dextrose in water infusions to prevent serum sodium from increasing greater than 6 mmol/L in 24 hours to diminish the likelihood of inducing osmotic demyelination [42]. Eleven had a persistently increased FEurate after correction of their hyponatremia. Twenty-one of the 24 patients with RSW had no clinical evidence of cerebral disease to support our proposal to change cerebral to RSW [2]. It is our hope that this change in nomenclature will come to fruition in the future to improve clinical outcomes. The perceived rarity of RSW and absence of cerebral disease would have led to water-restricting these patients for an erroneous diagnosis of SIADH. The increase in morbidity and mortality associated with hyponatremia may thus be in part iatrogenic [43].
4. One due to Addison disease
5. One due to hydrochlorothiazide
Instructive case
A 71-year-old male with advanced large B-cell lymphoma presented with a 9.1 kg weight gain over a 6-week period, had bilateral leg edema and postural hypotension and reflex tachycardia; lying blood pressure and pulse were 95/65 mmHg and 109 beats/min that decreased to 76/56 mmHg and 138 beats/min, respectively, on standing [13]. His baseline serum sodium was 115 mmol/L; creatinine, 0.9 mg/dL; blood urea nitrogen, 22 mg/dL; uric acid, 6.8 mg/dL, FEurate, 22.7%, Uosm, 308 mOsm/kg; and UNa only 10 mmol/L. There were no clinical signs or symptoms of cerebral disease. Because of the high FEurate and postural hypotension and reflex tachycardia, he was considered to have RSW with complete obstruction of the inferior vena cava by the lymphoma, which was later confirmed by a computed tomography scan. He was thus started on infusions of isotonic saline, which induced excretion of dilute urine 14 hours after initiation of isotonic infusion with a Uosm of 140 mmol/L and undetectable plasma ADH. Because his serum sodium had increased by 5 mmol/L over 5 hours, he was started on 5% dextrose and water to limit the increase in serum sodium to less than 6 mmol/L/24 hr to reduce the possibility of inducing osmotic demyelination [42].
The presence of ascites, pleural effusion, decreased cardiac output, and UNa of only 10 mmol/L were construed to be consistent with prerenal azotemia due to heart failure. This prompted the decision by others to stop the isotonic saline infusion and start an intravenous infusion of furosemide, despite warnings that this would be harmful in a patient with RSW. What followed was an abrupt increase in urine output that led to severe hemodynamic instability that required infusion of large volumes of isotonic saline. The keys to the diagnosis of RSW were the postural hypotension with reflex tachycardia and the very important FEurate of 22.7% which dramatically contrasted it to heart failure where the FEurate would be expected to be <4% (Fig. 2). This case illustrates the value of utilizing the algorithm that was key to arriving at the accurate diagnosis and treatment of this very instructive case (Fig. 2).
The clinical absence of cerebral disease added another compelling case of RSW to support changing cerebral to RSW and the UNa of only 10 mmol/L can be seen in a patient with RSW as discussed above.
Rat clearance studies demonstrating natriuretic activity in plasma of patients with neurosurgical and Alzheimer diseases
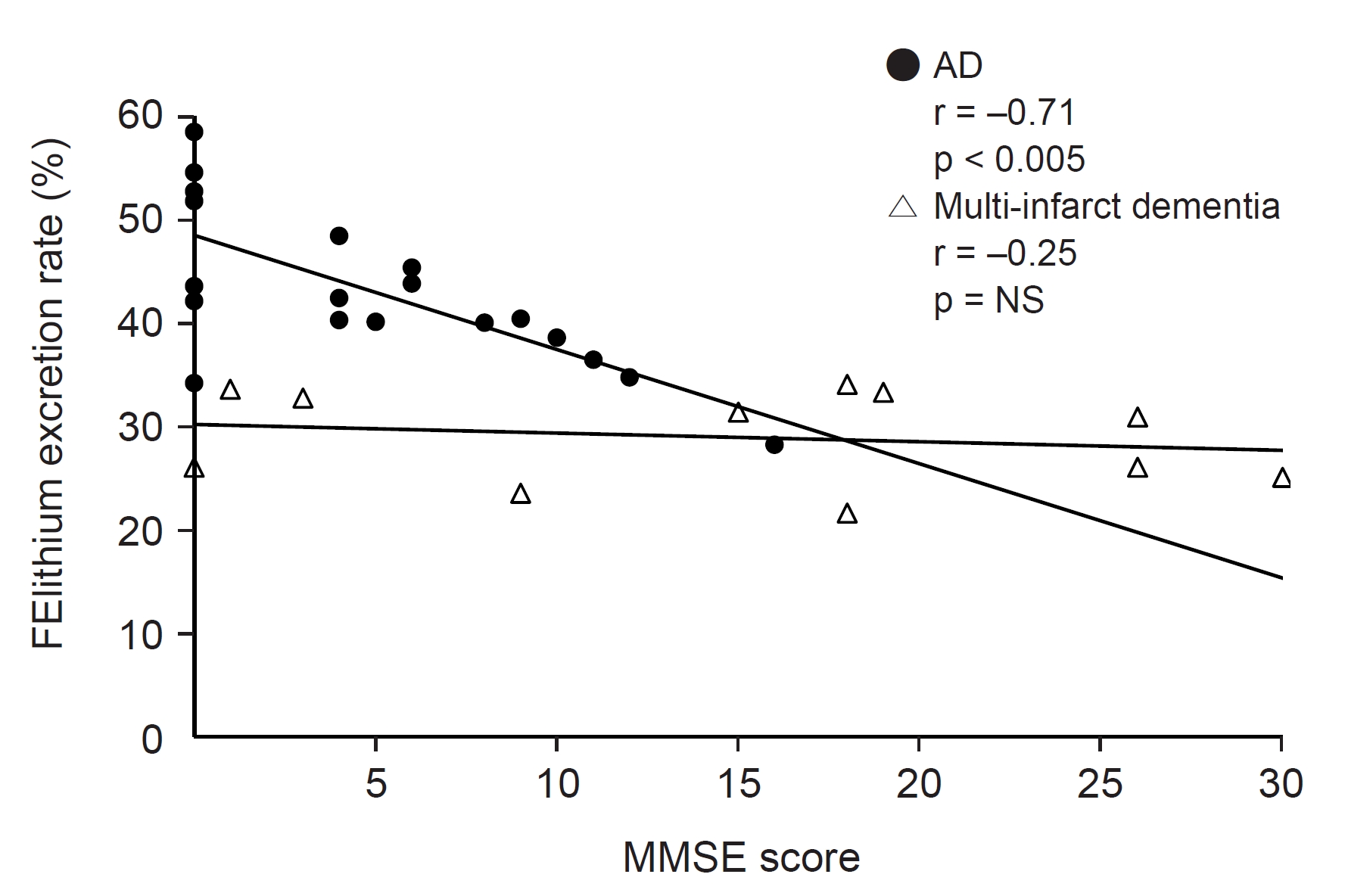
As part of our quest to identify physiologic mechanisms that contribute to clinical diseases, we developed strategies to identify a natriuretic protein that might cause RSW. We decided that an animal model would be most informative because it allowed many competing variables to be expressed as compared to an in vitro model where a limited number of variables can be expressed and controlled. We performed rat clearance studies by infusing plasma from prospective patients with RSW. The most likely candidates were neurosurgical patients where blood volume studies demonstrated RSW to be very common and in AD where the reported hypouricemia might be consistent with a high FEurate and RSW [44ŌĆō46]. Because uric acid is transported exclusively in the proximal tubule, a natriuretic factor must have a dominant effect on solute transport in the proximal tubule [12]. We elected to study lithium transport, which has been used as a marker of proximal tubular sodium transport by being transported on a one-to-one basis with sodium in the proximal tubule with little or no transport in the distal tubule [47]. On the other hand, sodium is vigorously transported in the distal tubule. In two separate rat clearance studies, we infused the plasma of 21 patients with various types of neurosurgical diseases and 18 patients with advanced AD, which we surmised might improve our chances of demonstrating the presence of a natriuretic factor [44,45]. The infusion of plasma in both studies revealed identical features. There were no changes in blood pressures or glomerular filtration rates and FENa sodium increased from the control of 0.3% and 0.33% to 0.59% and 0.63% in the neurosurgical and AD groups, respectively. FElithium increased from the control of 22.3% and 27.2% to 36.6% and 41.7% in the neurosurgical and AD groups, respectively [44,45]. Interestingly FElithium in the patients with fairly advanced AD progressively increased from an elevated level at a mini-mental status examination (MMSE) score of 12 to zero (Fig. 7). Attempts to identify the protein were abandoned because of limitations in protein analysis in 1993.
Identification of natriuretic protein in sera of patients with neurosurgical and Alzheimer diseases
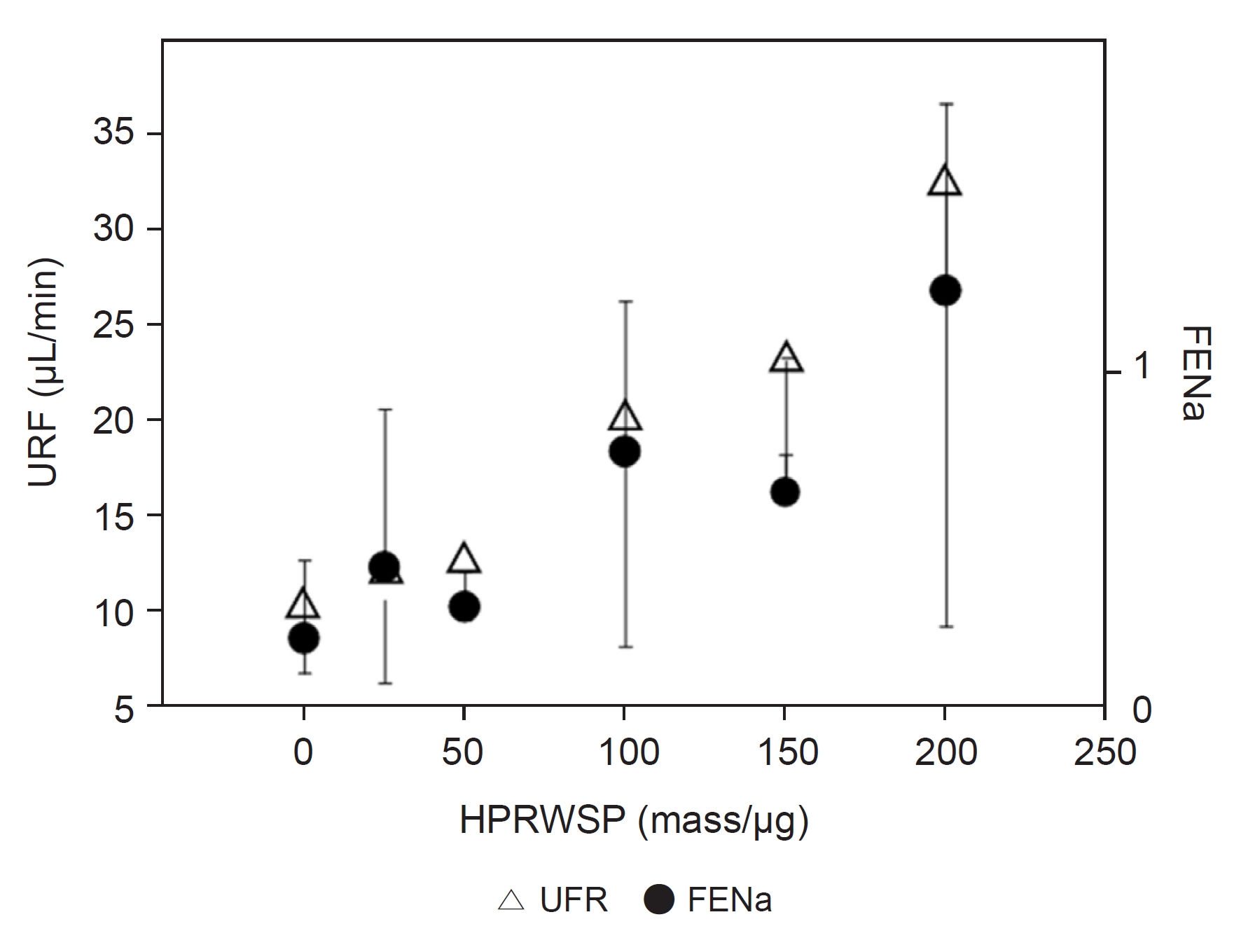
Identification of the natriuretic factor(s) in the plasma of patients with neurosurgical and ADs became possible when the analysis of proteins had developed to a point where every protein could be identified with precision in small sample sizes. We modified the protocol of the previous rat renal clearance studies by injecting 0.5 mL of serum in 1.5 minutes instead of intraperitoneal injections of 0.5 mL serum followed 90 minutes later by a constant infusion of 2 mL administered over a 3-hour period [1,44,45]. We found natriuretic activity in the sera of normonatremic patient with evidence of RSW due to SAH and another with AD. We subjected the sera with natriuretic activity and control to mass spectrometry and SWATH (sequential window acquisition of all theoretical mass spectra) analysis and subjected the results to RCProtein (fold-change of protein) to estimate semiquantitatively the relative change of a specific protein in the active sera as compared to a control serum [1]. Seventeen proteins in the sera with natriuretic activity were increased at least two-fold over the control sample with the highest levels noted for haptoglobins and haptoglobin-related protein (HPR). Recombinant samples of HPR with signal peptide, haptoglobin Hp 1-1, Hp 2-2, kininogen, thrombospondin, PROZ, alpha 1 microglobulin/bikunin, and retinol-binding protein had no natriuretic activity. A review of our analytical data revealed that HPR found in the active sera did not possess the signal peptide. Infusion of HPRWSP resulted in a robust dose-response increase in FENa sodium and urine flow rate (Fig. 8) [1]. The protocol using only 0.5 mL of serum showed an increase in FENa sodium, FElithium, and urine flow rates with no effect on FEglucose, FEphosphate, or FEurate, but the data are based on a single pass of the active serum to the kidneys. The protein can increase some or all of these solutes if there is a constant infusion of HPRWSP.
Clinical application of haptoglobin-related protein without signal peptide as biomarker and inhibitor to haptoglobin-related protein without signal peptide in hyponatremic and nonhyponatremic renal salt wasting patients
The high prevalence of RSW in hyponatremic patients in the general wards of the hospital justifies future efforts to develop methods to rapidly identify patients with RSW to select the proper mode of therapy to improve clinical outcomes. This can be accomplished by developing HPRWSP as a reliable biomarker of RSW, which is presently underway. The major causes of hyponatremia are dominated by SIADH, RO, RSW, and possibly medications and congestive heart failure. It would be anticipated that HPRWSP will be increased only in the RSW patients. The problem is to set criteria for determining HPRWSP in an expanding list of nonhyponatremic patients with RSW. The combination of the increasing use of isotonic saline in neurosurgical units, especially SAH, the common occurrence of RSW by blood volume studies in these patients, and the demonstration of natriuretic activity in the plasma of patients with various neurosurgical diseases justify determining HPRWSP blood levels to identify RSW in every neurosurgical patient and possibly in critical care intensive care units. Because HPRWSP with signal peptide had no natriuretic activity, it will be important to develop methods to determine levels of HPRWSP as a biomarker of suspected patients with RSW.
A new syndrome of renal salt wasting in Alzheimer disease
As noted above, FENa and FElithium increased significantly when the plasma of AD patients was injected into rats [45]. The significant but modestly higher FEurate of 9.7% in the AD patients as compared to 6.6% in control patients was much lower than the 18.7% noted in the 24 hyponatremic RSW patients recruited from the general medical wards of the hospital [1,45]. The comparatively lower FEurate of 9.7% in the AD patients suggests that these AD patients were more volume-depleted than the RSW patients in the general wards of the hospital as noted above.
Because there was a dose-response of FENa/FElithium to increasing doses of plasma with natriuretic activity and HPRWSP, blood levels of HPRWSP must have been progressively increasing as MMSE scores decreased from 12 to 0 in AD patients [1,45]. It appears that most or all patients with AD become progressively volume-depleted as they become more demented. Future studies intend to correlate plasma levels of HPRWSP with the onset and magnitude of RSW at different stages of dementia.
Up- and downregulation of haptoglobin-related protein without signal peptide and need to develop an inhibitor of haptoglobin-related protein without signal peptide
It appears that HPRWSP is normally produced at low levels, which appears to be upregulated under certain comorbid conditions. The duration of upregulation appears to have been of short duration in the 24 RSW patients in the general medical wards of the hospital. Most of their RSW appeared to subside as their comorbid conditions were successfully treated [1]. Only one patient continued to have RSW for 2 months after being discharged from the hospital. Treatment of all of these patients was simple as they responded favorably to isotonic saline infusions. In those that had significant volume depletion over an extended period of time, isotonic saline infusions significantly reduced quality of life by inducing polyuria and nocturia every 2 hours. In AD, however, there appears to be a permanent HPRWSP upregulation that will expose all organs of the body, especially of brain, to this protein. There is thus a need to develop an inhibitor to HPRWSP to simplify the management of all RSW patients, especially in AD where all organs appear to be permanently exposed to the putative effects of a relatively unknown protein. This would warrant investigations on the biologic effects of HPRWSP, especially on the brain. It would also be interesting to inhibit HPRWSP in all RSW AD patients to not only eliminate the need for isotonic saline infusions but also to determine its effect on the brain and possibly other organs of the body.
Conclusions
We hope we have successfully reviewed the state of confusion that exists in the area of hyponatremia and hyponatremia-related conditions. We focused on the evolution and substantive body of work on a new approach which demonstrated a high prevalence of RSW based on sound pathophysiologic principles, that have not been challenged.
We also hope we successfully justified changing cerebral to RSW and explaining the difficulty and therapeutic importance of differentiating SIADH from RSW. We encourage the reader to carefully review the valuable teaching points of the two cases presented and descriptions of a new syndrome of RSW in AD. We also describe the studies leading to identifying HPRWSP as the natriuretic peptide that causes RSW in hyponatremic and nonhyponatremic conditions and how it and its inhibitor can have optimistic diagnostic and therapeutic outcomes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









