


Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a group of disorders characterized by inflammation and destruction of small and medium-sized blood vessels, with few or no immune deposits, and the appearance of circulating ANCA with specificity toward proteinase-3 (PR3) or myeloperoxidase (MPO). The spectrum of anti-neutrophil cytoplasm antibody AAV includes three clinical phenotypes: microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA), and eosinophilic GPA (EGPA) [1]. AAV often affects the kidneys, the glomerulonephritis caused by AAV is called ANCA-associated glomerulonephritis (AAGN), and kidney involvement is an important factor with respect to patient morbidity and mortality.
Bowman capsule (BC) is a thick connective tissue barrier between the glomerular filtrate within the Bowman space and the interstitium. The BC is invested on its outer aspect by interstitial connective tissue, reticular fibers that contain type III collagen, and membrane-bound granular vesicles. Bowman capsule rupture (BCR) was first described in 1984, BCR was not only observed during crescent formation associated with vasculitis [2], and also found in pauci-immune glomerulonephritis [3]. In 2010, Berden et al. [4] proposed the histopathological classification dividing patients into four categories based on the proportion of normal, crescentic, and sclerotic glomeruli at renal biopsy (focal, crescentic, mixed, and sclerotic). A novel tool called the ANCA renal risk score (ARRS) was developed and validated by Brix et al. [5]. This prediction was based on three parameters: normal glomeruli, estimated glomerular filtration rate (eGFR), and interstitial fibrosis/tubular atrophy (IF/TA). However, BCR was not included in these scoring systems, also including rapidly progressive glomerulonephritis (RPGN) severity classification [6], Mayo Clinic chronicity score (MCCS) [7], and Banff scoring system [8]. Recent reports on adult patients established a better performance of the Berden classification and ARRS after the addition of BCR to these scoring systems, suggesting that the BCR lesion was independent from already described glomerular and renal tubule lesions [9]. MPO-AAGN is the predominant type in Asian, such as Chinese and Japanese, while PR3 positive is more common in Western countries [10ŌĆō12]. However, the effect of BCR on MPO-AAGN in children has not been explored so far, Therefore, in this study, we aimed to explore the relationship between BCR and clinical manifestations, pathological changes, and prognosis in children with MPO-AAGN.
Methods
Patient
Children (<18 years old) with biopsy-proven MPO-AAGN newly diagnosed in the Department of Pediatrics, Jinling Hospital, an Affiliated Hospital of Medical School, Nanjing University, from June 2017 to June 2022 were recruited consecutively into the study. MPO-AAGN was defined as serum MPO-ANCA positive and pauci-immune type necrotizing and/or crescentic glomerulonephritis (CrGN). Exclusion criteria were 1) PR3-ANCA positive; 2) glomerular diseases: anti-glomerular basement membrane (anti-GBM) nephritis, membranous nephropathy, Henoch-Sch├Čnlein purpura nephritis, immunoglobulin A nephropathy, and lupus nephritis (LN); 3) secondary vasculitis; 4) tumor; 5) biopsy specimens contained <10 glomeruli and follow-up duration of <6 months.
Clinical and laboratory data included demographics, clinical manifestations of AAV, serology, and urine examination. The eGFR was calculated using the modified Schwartz formula [13]. Disease activity was assessed using the pediatric vasculitis activity score (PVAS) [14]. Acute kidney injury (AKI), acute kidney disease (AKD), and chronic kidney disease (CKD) definitions were based on the KDIGO (Kidney Disease: Improving Global Outcomes) guidelines [15]. All the data were abstracted retrospectively from the electronic medical records. The study conformed to the principles outlined in the Declaration of Helsinki and was approved by the Ethical Committee of Jinling Hospital (No. 2019JLHGKJDWLS-177). Because of the retrospective design of the study, the need to obtain informed consent from eligible patients was waived by the Committee.
Renal histopathology
Two kidney pathologists came from the Department of Renal Pathology of Jinling Hospital evaluated all biopsies and assessed the integrity of BC and were blinded to all clinical data and analyses. Kidney tissues were stained with periodic acid-silver methenamine and evaluated by a kidney pathologist using light microscopy. BCR was defined as a discontinuity in the wall of BC in renal biopsy sections (Fig. 1; Supplementary Fig. 1, available online). Based on the status of BC, patients were divided into two groups: the BCR (+) group was defined as patients with glomeruli involved by Ōēź1 BCR, while those without BCR were assigned to the BCR (ŌłÆ) group.
Based on the Berden classification, ARRS, RPGN severity classification, and MCCS systems, the patients were divided into different types. Within a renal biopsy, infiltrates of neutrophils, eosinophils, plasma cells, and mononucleated cells (macrophages, lymphocytes) were quantified as a fraction of the area of total cortical inflammation [16]. Tubular dilatation, epithelial simplification, brush border shedding, tubular vacuolization, and casts were given a score between 0 and 4 as a percentage of the total cortical area of the biopsy (0, 0%ŌĆō1%; 1, >1%ŌĆō10%; 2, >10%ŌĆō25%; 3, >25%ŌĆō50%; and 4, >50%) [17].
We observed the distribution of tubulointerstitial inflammation and scored (score 1, Ōēż25%; 2, 26%ŌĆō50%; and 3, >50%). The degree of tubulitis was evaluated and scored (score 1: mild, 0ŌĆō9 inflammatory cells/tubules; 2: moderate, 10ŌĆō14 cells/tubules; and 3: severe, 15 or more cells/tubules in the most affected region) [18]. The total renal chronicity score including global/segmental glomerular sclerosis (score 0, <10%; 1, 10%ŌĆō25%; 2, 26%ŌĆō50%; and 3, >50%), interstitial fibrosis (score 0, <10%; 1, 10%ŌĆō25%; 2, 26%ŌĆō50%; and 3, >50%); tubular atrophy (score 0, <10%; 1, 10%ŌĆō25%; 2, 26%ŌĆō50%; and 3, >50%), and arteriosclerosis (score 0, intimal thickening < thickness of media and 1, intimal thickening Ōēź thickness of media) [16]. The extent of crescents was graded into five categories: grade 0, lesion < 10%; grade 1, 10% Ōēż lesion < 25%; grade 2, 25% Ōēż lesion < 50%; grade 3, 50% Ōēż lesion < 75%; and grade 4, lesion Ōēź 75% (lesion refer to cellular/fibrocellular) [19]. Based on the individual lesions, each biopsy was evaluated according to the Banff scoring system, and the Banff score lesions include interstitial inflammation (i), tubulitis (t), arteritis (v), glomerulitis (g), interstitial fibrosis (ci), tubular atrophy (ct), arteriolar hyalinosis (ah), peritubular capillaritis (ptc), total inflammation (ti), inflammation in areas of IF/TA (i-IF/TA), and tubulitis in areas of IF/TA (t-IF/TA) [8].
Treatments
The treatment of AAGN was based on the book of Chinese Nephrology [20]. All the patients were treated via oral prednisolone. Other treatments were determined according to clinical and pathological manifestations and disease severity, including methylprednisolone pulse therapy, cyclophosphamide, glucocorticoids, calcineurin inhibitors, hydroxychloroquine and rituximab, renal replacement therapy (RRT), and plasma exchange. There was no difference in treatment between the two groups.
Outcomes assessment
The primary endpoint of the study was the cumulative percentage of patients who developed end-stage kidney disease (ESKD) over time censored by death. ESKD was defined as the need for long-term RRT or renal transplantation. Renal survival time for each patient was computed from baseline evaluation at the time of biopsy to the last time of follow-up or the time point of reaching ESKD.
Statistical analyses
All analyses were performed using IBM SPSS version 24.0 (IBM Corp.). Continuous variables were described as mean and standard deviation or median (interquartile range [IQR]), and differences between groups were analyzed using a two-factor analysis of variance or a nonparametric test. Categorized variables were described as percentages and were analyzed using the chi-square test. The association of variables with ESKD was assessed with univariate and multivariate Cox proportional hazard regression models. The prognosis was evaluated using Kaplan-Meier curves, and the log-rank test was used to test the two curvesŌĆÖ differences. Spearman correlation analyses were used to analyze correlations and shown by a heatmap reflecting mean values of SpearmanŌĆÖs Žü, asterisks indicate p < 0.05. The r-value of >0.5 was defined as a moderate correlation. A p-value of <0.05 (two-sided) was considered significant.
Results
Baseline of demographic, clinical, and pathological characteristics
Based on clinical characteristics, the mean age was 15.28 ┬▒ 3.48 years, and 53 of 56 patients (94.6%) were diagnosed with MPA and the remainder with GPA. As presented in Table 1, the levels of C-reactive protein, serum creatinine (sCr), urinary N-acetyl-╬▓-D-glucosidase enzyme, and neutrophil gelatinase-associated lipocalin in the BCR (+) group were higher than those in the BCR (ŌĆō) group (p < 0.05), and the levels of hemoglobin, platelet, eGFR, and C3 in the BCR (+) group were lower than those in the BCR (ŌĆō) group (p < 0.05 and p < 0.01). The BCR (+) group demonstrated a lower frequency of focal and higher crescentic Berden classes as compared to the BCR (ŌĆō) group (p < 0.05), and the BCR (+) group had a lower percentage of ARRS low-risk and higher ARRS high-risk than the BCR (ŌĆō) group (p < 0.05). Based on RPGN severity classification, the cases of grade II in the BCR (+) group were more than the BCR (ŌĆō) group (p < 0.05). The extent and scores of crescents, tubulointerstitial inflammation, tubulitis, interstitial fibrosis, and tubular atrophy in the BCR (+) group were greater than the BCR (ŌĆō) group (p < 0.01) (Table 1).
Correlations between Bowman capsule rupture and clinical characteristics and laboratory markers
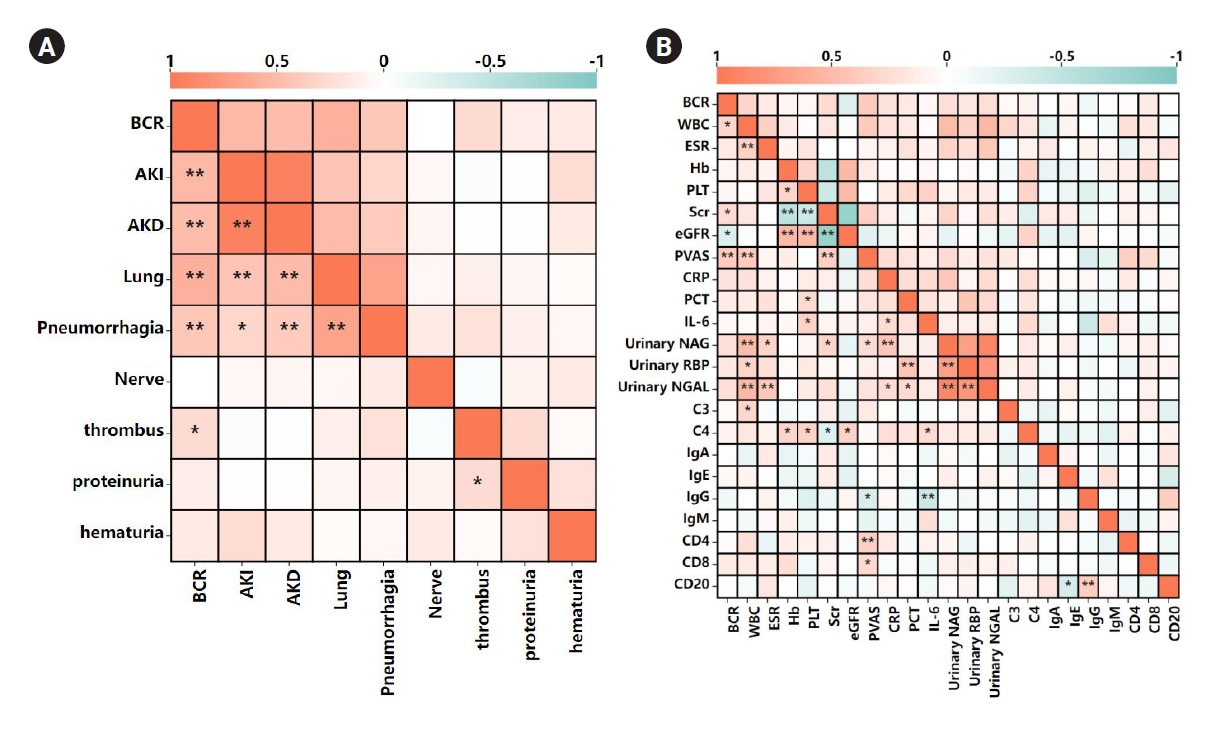
The results of relationship between BCR and clinical and laboratory features were shown in Fig. 1. BCR positively correlated with the manifestations of AKI, AKD, lung injury, pneumorrhagia, and thrombus (r = 0.52, p < 0.001; r = 0.499, p < 0.001; r = 0.60, p < 0.001; r = 0.41, p = 0.002; and r = 0.27, p = 0.045; respectively), and positively correlated with levels of white blood cells, sCr, and PVAS (r = 0.32, p = 0.02; r = 0.27, p = 0.045; and r = 0.39, p = 0.003; respectively), and negatively correlated with eGFR (r = ŌĆō0.27, p = 0.04). Above them, BCR positively moderately correlated with AKI, AKD, and lung injury.
Correlations between Bowman capsule rupture and renal pathological changes
Considering that BCR was a special pathological lesion, we analyzed the relationship between BCR and renal pathological changes. We found that BCR positively correlated with intrarenal neutrophils, mononuclear cells, plasma cells, and eosinophils infiltrates (r = 0.62, p < 0.001; r = 0.60, p < 0.001; r = 0.44, p = 0.001; and r = 0.28, p = 0.04; respectively) (Fig. 2A). BCR positively correlated with glomerular obsolescence and crescent, tubulointerstitial inflammation score, tubulitis score, tubular atrophy score, epithelial simplification, tubular dilation, tubular vacuolization, and granular casts (r = 0.34, p = 0.01; r = 0.50, p < 0.001; r = 0.56, p < 0.001; r = 0.41, p = 0.002; r = 0.31, p = 0.02; r = 0.55, p < 0.001; r = 0.41, p = 0.002; r = 0.31, p = 0.02; and r = 0.31, p = 0.02; respectively), and negatively correlated with normal glomeruli and immunoglobulin G (IgG) deposition (r = ŌĆō0.29, p = 0.03 and r = ŌĆō0.41, p = 0.002; respectively) (Fig. 2B). We also analyzed the relationship between BCR and Banff score system, and the results showed that BCR positively correlated with interstitial inflammation (i), tubulitis (t), tubular atrophy (ct), total inflammation (ti), and i-IF/TA (r = 0.50, p < 0.001; r = 0.41, p = 0.002; r = 0.31, p = 0.02; r = 0.43, p = 0.001; and r = 0.40, p = 0.003; respectively). The above results suggested that BCR positively moderately correlated with intrarenal neutrophils and mononuclear cell infiltrates, crescent, tubulointerstitial inflammation score, epithelial simplification, and interstitial inflammation (i) (Fig. 2C).
Correlations between Bowman capsule rupture and clinical and pathological scoring system
BCR positively correlated with mixed and crescentic groups in the Berden classification, ARRS medium-risk and high-risk groups, and MCCS minimal group (r = 0.27, p = 0.045; r = 0.45, p < 0.001; r = 0.27, p = 0.045; r = 0.37, p = 0.005; and r = 0.27, p = 0.046; respectively), and negatively correlated with focal group of the Berden classification and ARRS low-risk group (r = ŌĆō0.45, p < 0.001 and r = ŌĆō0.52, p < 0.001; respectively). Of which, BCR negatively moderately correlated with ARRS low-risk group (Fig. 2D).
Survival analysis and risk factor
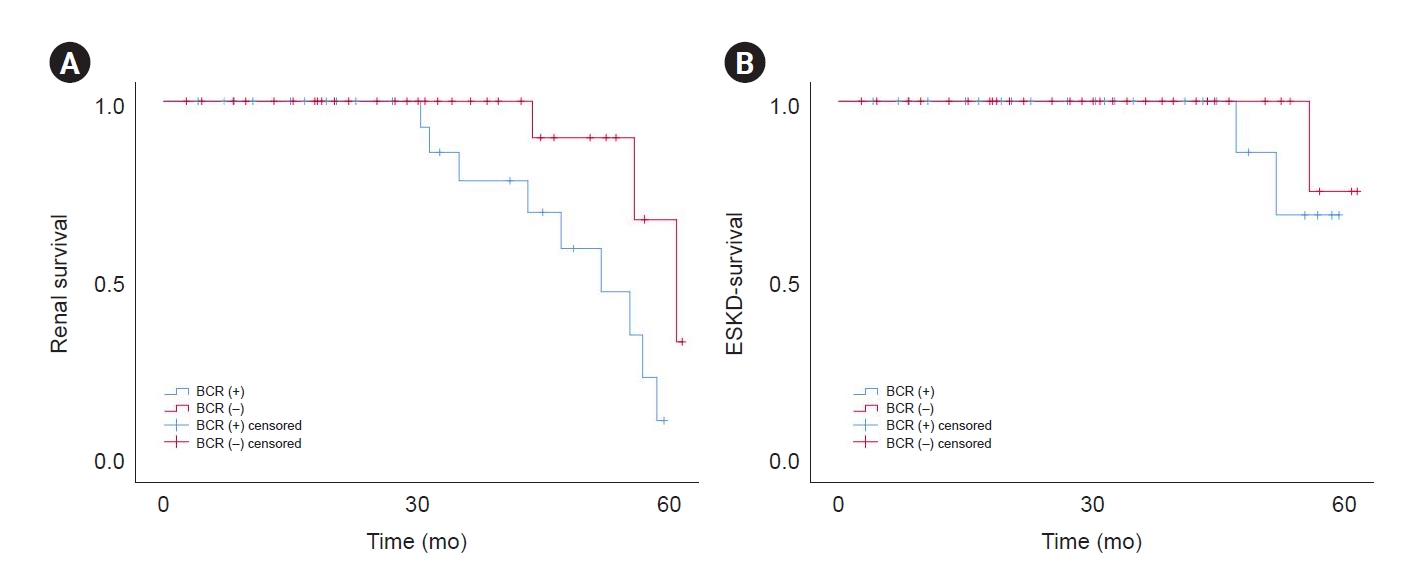
The median follow-up period was 31.98 months (IQR, 16.64ŌĆō45.51 months). During the observational period, 12 children (21.4%) progressed to ESKD, with significantly more patients in the BCR (+) group than BCR (ŌĆō) group (p < 0.05). There were three deaths (5.4%), including two cases in BCR (+) group and one case in BCR (ŌĆō) group. The causes of death were interstitial pneumonia (n = 2) and sepsis (n = 1). We analyzed renal survival according to BCR. Our results showed that the estimated renal survival at 1 and 3 years in the BCR (+) group were 100% and 77.9%, respectively, and the renal survival was 100% at both 1 and 3 years in the BCR (ŌĆō) group. The renal survival rate in the BCR (+) group was significantly poorer than the BCR (ŌĆō) group (Žć2 = 5.45, p = 0.02) (Fig. 3A); however, there was a numerical but not statistical difference in ESKD-free survival between two groups (Žć2 = 0.51, p = 0.47) (Fig. 3B). The multivariate Cox regression analysis showed that eGFR of Ōēż15 mL/min/1.73 m2 (hazard ratio [HR], 1.71; 95% confidence interval [CI], 0.87ŌĆō3.33; p = 0.02), BCR (HR, 11.28; 95% CI, 2.64ŌĆō21.17; p = 0.003), and ARRS (HR, 17.14; 95% CI, 6.88ŌĆō40.52; p = 0.009) were independent risk factors for the development of ESKD in children with MPO-AAGN (Table 2). And multivariate logistic regression analysis showed that BCR was associated with neutrophils and plasma cell infiltration, tubulointerstitial inflammation (Table 3).
Comparison of predictive value between the Berden classification, antineutrophil cytoplasmic antibody renal risk score, and Bowman capsule rupture
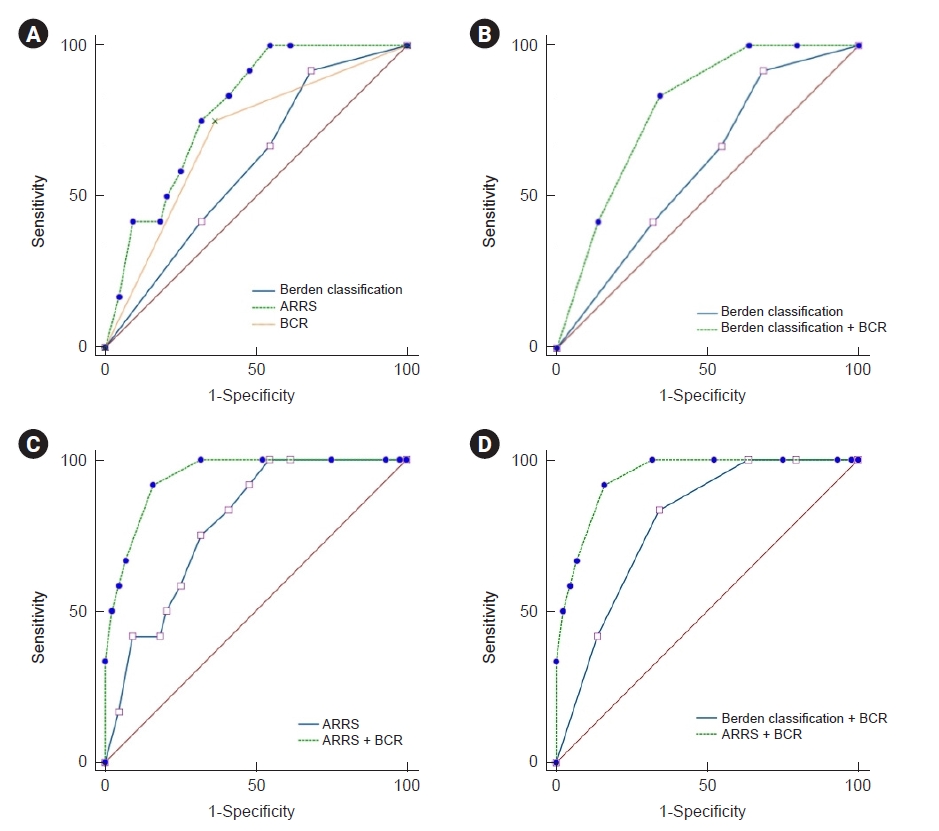
The area under the curve for ESKD prediction at the end of follow-up of the Berden classification, ARRS, and BCR were 0.60 (p = 0.28), 0.79 (p = 0.002), and 0.69 (p = 0.04), respectively. ARRS showed better predictive value for ESKD than those of the Berden classification (p = 0.004) (Fig. 4A; Supplementary Fig. 2, available online). After combining BCR with ARRS and the Berden classification, they show better predictive values. The Berden classification + BCR showed better predictive value for ESKD than those of the Berden classification (0.79 vs. 0.60, p = 0.004) (Fig. 4B), ARRS + BCR showed better predictive value for ESKD than those of the ARRS (0.94 vs. 0.79, p = 0.001) (Fig. 4C), and ARRS + BCR showed better predictive value for ESKD than those of the Berden classification + BCR (0.94 vs. 0.79, p = 0.002) (Fig. 4D).
Discussion
BCR was first reported more than 30 years ago, and only a few case reports have described its presence in diseased kidneys to date. Previous research showed that BCR was present in 21% to 65% of adult patients with AAGN [21ŌĆō25]. The percentage of BCR in our series of AAGN children was 42.9%, which was consistent with the data in previous literature.
BC was implicated in functionally isolating potential immune effectors thereby preventing injury to the glomerulus, and an intact BC prevents inflammatory cells from gaining access to the glomerular space. However, once BC was breached, inflammatory cells could access the glomerular space in CrGN with BCR enabling direct pathological interaction between both compartments [26]. When renal inflammation leads to the destruction of glomerular capillaries and the release of proinflammatory cytokines and chemokines into the BC, parietal epithelial cells proliferate and build crescents [27]. When BC was normal, vascular injury causing ruptures in the GBM that triggered plasmatic coagulation within BC, drove hyperplasia of parietal epithelial cells and the formation of crescent. Furthermore, immune cell infiltrates in AAGN were found to influence renal outcomes [28]. In addition to AAGN, BCR is also present in immune complex-mediated CrGN, anti-GBM CrGN, and LN [23ŌĆō25,29]. Therefore, we suspected that the formation of BCR may be associated with renal inflammation, immune cell infiltration, and renal prognosis in children with MPO-AAGN.
To clarify the role of BCR in AAGN, we evaluated differences in clinical and laboratory manifestations and renal histopathology changes between the BCR (+) and BCR (ŌĆō) groups. Our results indicated that the clinical features and kidney involvement were more severe in the BCR (+) group. The renal survival rate was significantly poorer in the BCR (+) group than in the BCR (ŌĆō) group.
The relationship between BCR and renal pathological changes in the kidney had rarely been reported. Recent studies have shown that BCR links glomerular damage to tubulointerstitial inflammation in a considerable subset of patients with AAGN [9,21,30]. Hakroush and Tampe [30] found that BCR was associated with tubulointerstitial inflammation containing infiltrates of neutrophils, eosinophils, and plasma cells. A study on LN showed that BCR was correlated with the levels of crescents, tubular atrophy, and interstitial fibrosis [29]. To our knowledge, the relationship between BCR and renal pathological changes lesions in children with MPO-AAGN has not been reported. In our study, as suggested by the results from the MPO-AAGN children, the BCR is positively associated with intrarenal immune cells infiltration, glomerular obsolescence and crescents, tubulointerstitial inflammation, tubulitis, tubular atrophy, and inflammatory and tubular lesions in the Banff score system, and negatively correlated with normal glomeruli and IgG deposition in the kidney. However, Hakroush and Tampe [31] demonstrated that an association between tubulointerstitial inflammation and BCR was specifically observed in PR3-AAGN and was not observed in adult with MPO-AAGN. These findings indicated that the renal pathology of AAGN in adults and children is different, and further research on the mechanism is needed. Multivariate logistic regression analysis confirmed that BCR was associated with neutrophil and plasma cell infiltration, and tubulointerstitial inflammation, which provides a theoretical reference for research on the BCR formation mechanism.
For almost two decades, constant effort has been made to stratify ESKD risk in AAGN. We demonstrated that BCR has independently been associated with poor renal outcomes in children with MPO-AAGN. Recent studies have demonstrated the good discrimination of the Berden classification and ARRS, and the relationship between ARRS and BCR as well as the effect of BCR on renal prognosis has gradually attracted the attention of clinicians. LŌĆÖImperio and Pagni [32] showed that arteritis was correlated with evidence of BCR in AAV, which suggested a complementary role for these two features in improving the predictive performance of the ARRS. Duan et al. [29] suggested that it correlates with severe clinical manifestations, pathological changes, and poor prognosis in patients with LN. Furthermore, we incorporated BCR into the two models that permitted the identification of MPO-AAGN patients who could benefit from that, with better sensitivity and specificity. Our data suggested that the Berden classification + BCR and ARRS + BCR showed better predictive values for ESKD than those of the Berden classification and ARRS, respectively. And ARRS + BCR showed better predictive value for ESKD than those of the Berden classification + BCR. These findings illustrated that indications of BCR need to be clarified, and it would be very interesting to assess its value in other cohorts with AAGN and CrGN.
Our study also had certain limitations. First, we excluded children with known PR3-AAGN, so our results are not generalizable to that subset of children. Second, due to the limited number of patients, it was difficult to determine the effect of drugs on BCR. Finally, this was a single-center retrospective observational analysis, and it was difficult to control for all factors that may affect renal survivorship.
Our study represents a further step in the description of the relationship between BCR and renal damage. This was the first study to describe the relationship between BCR and MPO-AAGN in children. We show that BCR was frequent in children with MPO-AAGN and was observed in a subset of renal biopsies in our single-center cohort. Additionally, BCR was an independent risk factor for the development of ESKD. Furthermore, a better performance of the Berden classification and ARRS were observed after the implementation of BCR to the classification systems.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print






")









