


Introduction
Major depressive disorder is the most common psychiatric disorder among patients with end-stage kidney disease (ESKD) [1–3]. Upon initiating dialysis, patients with incident ESKD suffer from stress and various dialysis-related somatic symptoms. Furthermore, regular dialysis restricts social and occupational activities [4–6]. Concurrent presence of physical symptoms and mental stress may cause depression in patients with ESKD [4,7,8].
Depression in patients on maintenance dialysis is associated with adverse outcomes, such as mortality and hospitalization [3,9–11]. In a study from the United States, the rates of hospitalization due to depression were significantly higher in elderly patients with ESKD than those in non-ESKD elderly patients with chronic medical conditions, such as ischemic heart disease, cerebrovascular disease, and peptic ulcer disease [12]. While the mean age of patients initiating dialysis is steadily increasing [13,14], the prevalence and impact of depression on survival rates of older patients with ESKD remain unclear.
Depression and frailty were identified to have reciprocal interactions in the elderly population [15]. Depression is associated with an increased prevalence and incidence of frailty, and frailty at dialysis initiation is associated with higher mortality in patients initiating dialysis [16].
The Beck Depression Inventory-II (BDI-II) score was first introduced by Beck et al. [17] in 1996 and has been widely used as a screening instrument for depression. It is a 21-item self-questionnaire consisting of three depressive symptom domains. Affective domain is composed of emotional symptoms such as sadness, anxiety, and irritability. Cognitive domain consists of cognitive symptoms such as indecisiveness, sense of failure and guilt. Physical symptoms, such as fatigue, loss of energy, weight loss, and sleep disturbance are included in somatic domain.
This study aimed to investigate the factors predisposing to depressive disorders and the association between depression severity and long-term mortality in older patients with ESKD using nationwide prospective ESKD cohort data. Furthermore, we compared the impact of the three depressive symptom domains on patient survival.
Methods
Study population
This study enrolled patients from the Clinical Research Center for End-Stage Renal Disease (CRC for ESRD) in Korea. The CRC for ESRD included a multicenter prospective cohort of patients undergoing dialysis at nationwide 31 participating hospitals in South Korea (NCT00931970). Between July 2009 and May 2018, 487 patients aged >65 years and newly diagnosed with ESKD on maintenance dialysis for >3 months were included in the analysis (Supplementary Fig. 1, available online). The details of the cohort are described in a previous report [18].
Ethics approval and consent to participate
The Institutional Review Boards (IRBs) of all participating centers approved the study protocol before patient enrollment. The names of the IRBs are as follows: The Catholic University of Korea, Bucheon St. Mary’s Hospital; The Catholic University of Korea, Incheon St. Mary’s Hospital; The Catholic University of Korea, Seoul St. Mary’s Hospital; The Catholic University of Korea, St. Mary’s Hospital; The Catholic University of Korea, St. Vincent’s Hospital; The Catholic University of Korea, Uijeongbu St. Mary’s Hospital; Cheju Halla General Hospital; Chonbuk National University Hospital; Chonnam National University Hospital; Chung-Ang University Medical Center; Chungbuk National University Hospital; Chungnam National University Hospital; Dong-A University Medical Center; Ehwa Womans University Medical Center; Daegu Fatima Hospital; Gachon University Gil Medical Center; Inje University Pusan Paik Hospital; Kyungpook National University Hospital; Kwandong University College of Medicine, Myongji Hospital; National Health Insurance Service Ilsan Hospital; National Medical Center; Pusan National University Hospital; Samsung Medical Center; Seoul Metropolitan Government, Seoul National University, Boramae Medical Center; Seoul National University Hospital; Seoul National University Bundang Hospital; Yeungnam University Medical Center; Yonsei University Severance Hospital; Yonsei University Gangnam Severance Hospital; Ulsan University Hospital; and Wonju Christian Hospital (in alphabetical order). Written informed consent was obtained from all patients prior to inclusion. This study was performed in accordance with the 2013 Declaration of Helsinki.
Data collection
The requisite data were extracted from the web-based CRC for ESRD database. Baseline patient information was collected at enrollment, including demographics, history of primary renal disease, dialysis modality, comorbidities, and laboratory values. The modified Charlson comorbidity index (mCCI) was calculated for each patient at the time of dialysis [19,20].
Assessment of depression
Depression was evaluated using the BDI-II questionnaire at the time of enrollment. The BDI-II is a 21-item questionnaire that assesses the severity of depressive symptoms [17]. Each symptom is rated between 0 and 3, with a greater score indicating increased severity. The BDI-II score was divided into tertiles: minimal (0–10), mild-to-moderate (11–19), and severe depression (≥20). Additionally, BDI-II scores were separated into three symptom domains: affective, cognitive, and somatic depressive symptoms [21].
Outcomes
The main study outcome was all-cause mortality after initiation of dialysis during the study period. Mortality data of the cohort patients were obtained from Statistics Korea until December 2019. Patients were censored at the time of loss of follow-up or kidney transplantation.
Statistical analysis
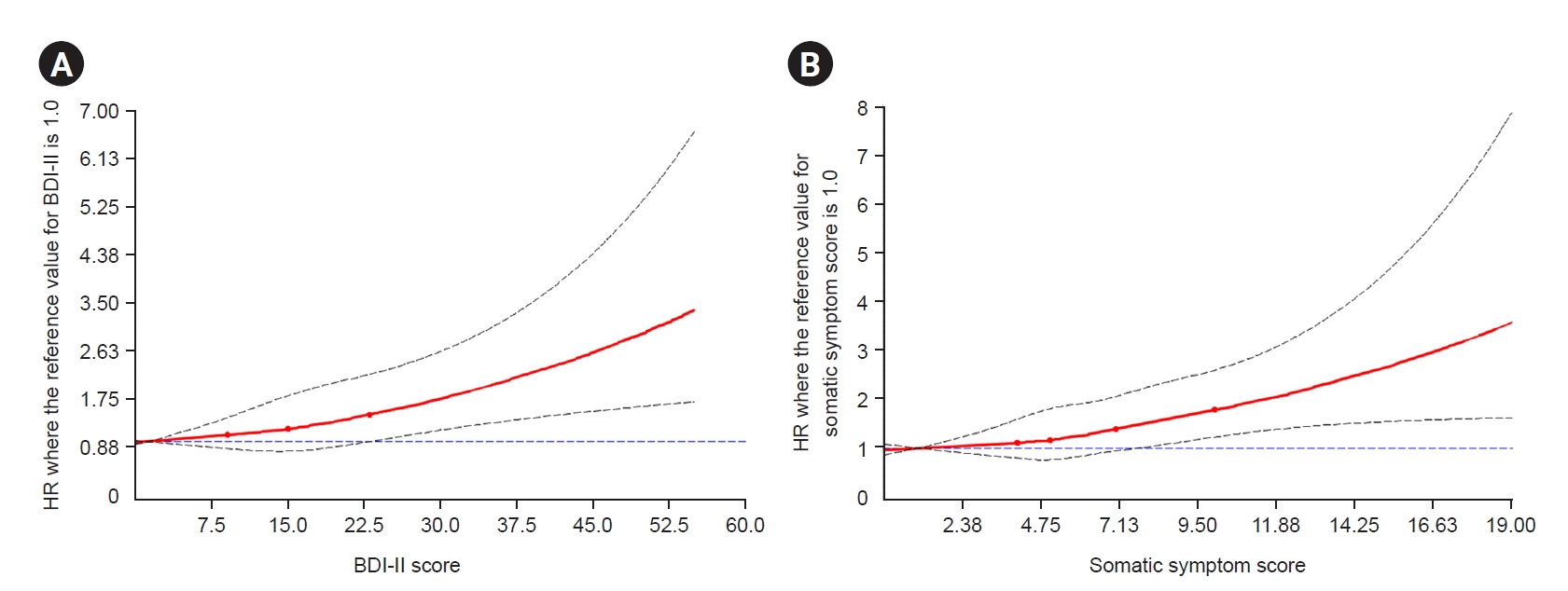
Continuous and categorical variables are presented as mean ± standard deviation and numbers (percentage), respectively. Analysis of variance was used to compare continuous variables, and Pearson chi-square or Fisher exact test was used for categorical variable comparisons. The Kaplan-Meier curve with the log-rank test was used to compare the differences in mortality among the three depression groups. A Cox proportional hazards regression model was used to calculate the adjusted hazard ratios (HRs) for all-cause mortality in the tertiles. Association between the BDI-II score and mortality was evaluated using multivariate Cox regression analysis, for which clinically important baseline characteristics, including age, sex, mCCI, and serum albumin, phosphate, and uric acid levels, were selected as adjustment values; the univariate analysis determined the values that were significantly different at baseline, which were subsequently included in the multivariate analysis along with age and sex. Factors associated with the BDI-II score were evaluated using logistic regression analysis. The associations among the three depressive symptom domains and mortality were analyzed using multivariate Cox proportional hazard regression models. The Kaplan-Meier method was used to analyze the differences in mortality among tertiles of depressive symptom domains. The cut-off values for the tertiles of depressive symptom scores were as follows: affective: <1, 1–5, ≥5; cognitive: <3, 3–7, ≥7; and somatic symptom: <5, 5–8, ≥8. To analyze the BDI-II or somatic symptom score as a quantitative variable, the relationship between each score and mortality was evaluated using a Cox proportional hazard model with restricted cubic spline functions to capture potential nonlinear effects. Statistical analyses were performed using the IBM SPSS version 22.0 (IBM Corp.) and R version 3.6.2 (The R Foundation for Statistical Computing). Statistical significance was set at p < 0.05.
Results
Baseline characteristics
Of 487 older patients with newly diagnosed ESKD on dialysis, 305 (62.6%) were male and the mean age was 74.2 ± 6.7 years. The mean BDI-II score was 16.5 ± 10.9, and patients were followed up for a median of 69.3 months. The proportion of patients with hemodialysis was higher than that of patients with peritoneal dialysis (76.8% vs. 23.0%, respectively). Until December 2019, 245 patients died and 96 (56.5%) of deceased patients had severe depression. Table 1 summarizes the baseline demographic characteristics and laboratory values of the depression groups stratified by the BDI-II scores. The severe depression group had a higher mCCI, more comorbidities, such as cerebrovascular diseases, chronic lung disease, and malignancy, and lower serum albumin, phosphate, and uric acid levels than the other depression groups.
Predictors of severe depression
Univariate analysis showed a positive association between BDI-II and mCCI and negative associations between BDI-II and serum albumin, phosphate, and uric acid levels (Table 2). In the multivariate linear regression model, BDI-II score displayed a positive association with mCCI and a negative association with serum albumin level (p = 0.009 and p = 0.04, respectively).
Association between Beck Depression Inventory-II score and mortality
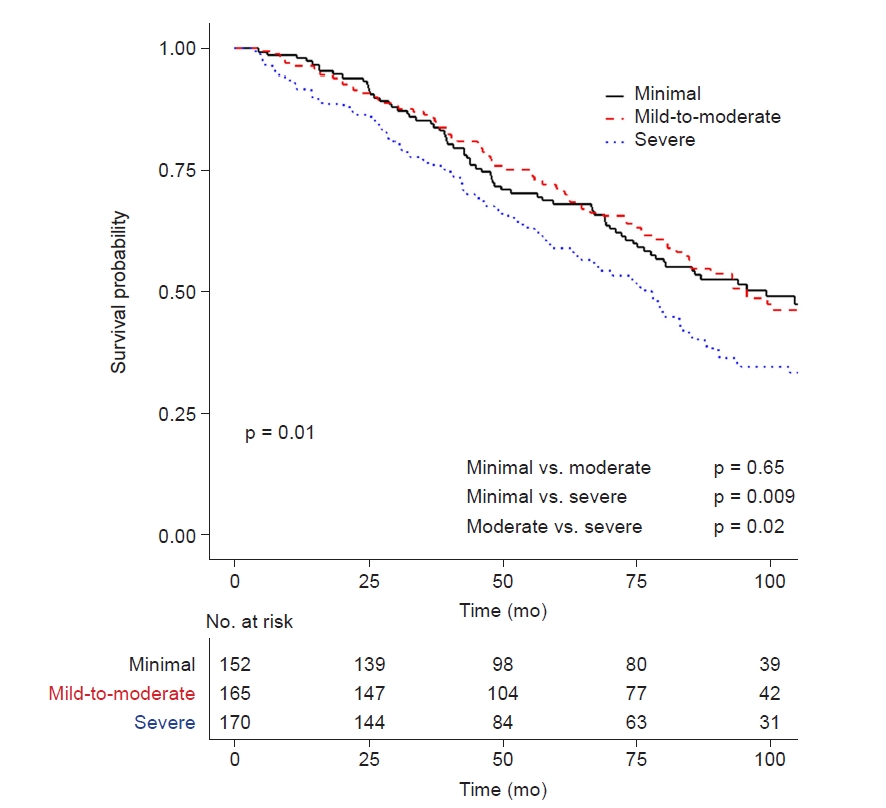
Higher BDI-II and somatic symptom scores were both associated with increased mortality in older patients with ESKD (Fig. 1). In the Kaplan-Meier survival curve, the severe depression group showed significantly lower survival than the minimal and mild-to-moderate depression groups (log-rank p = 0.01) (Fig. 2). In the Cox proportional hazards model, severe depression was an independent risk factor for mortality in older patients with ESKD (model 4: HR, 1.39; 95% confidence interval [CI], 1.01–1.91; p = 0.04) (Table 3). However, mortality risk was comparable between mild-to-moderate and minimal depression.
Analysis of depressive symptom domains
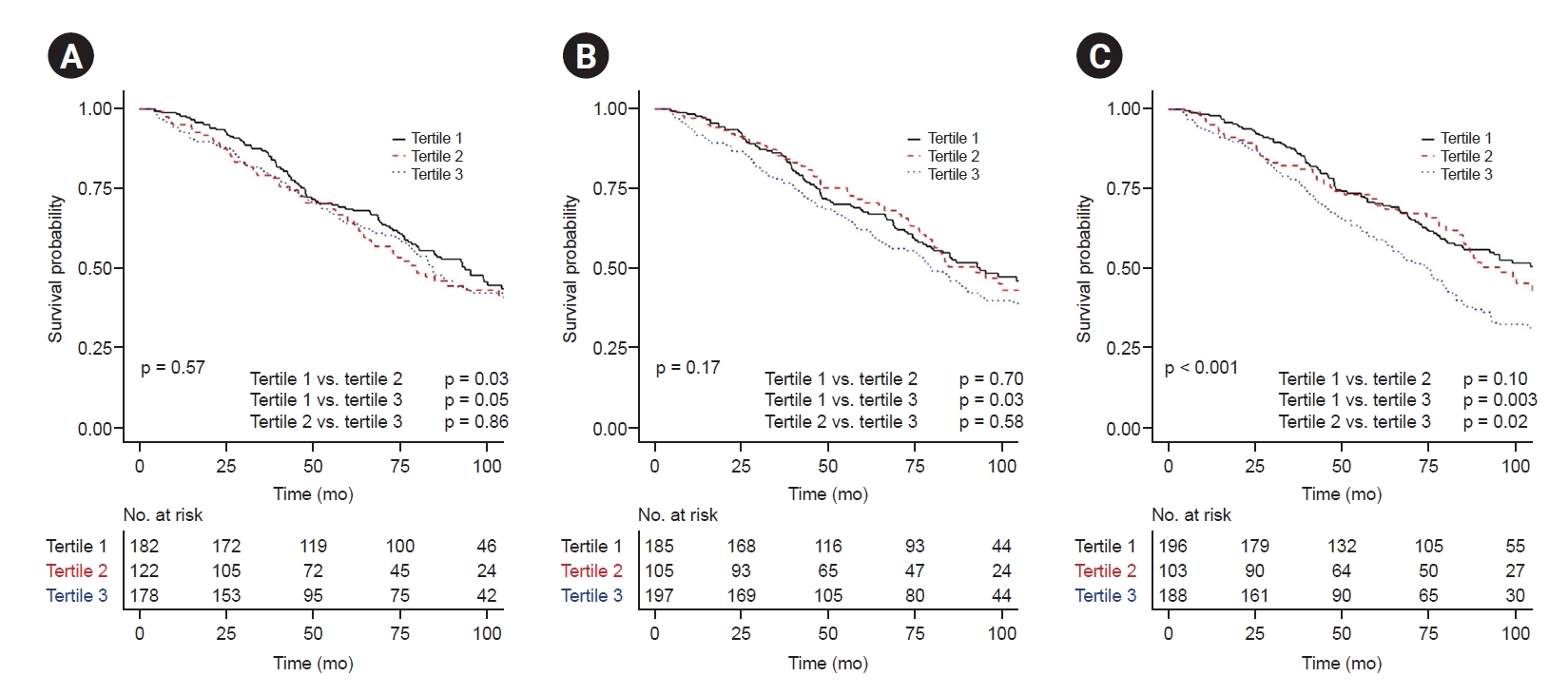
When comparing depressive symptoms among the tertiles, the differences in the three depressive symptom scores were similar to that of the BDI-II scores, with the highest scores in the severe depression group (Supplementary Table 1, available online). To analyze the factors related to survival among depressive symptom domains, each depressive symptom score (affective, cognitive, and somatic symptom scores) was divided into tertile groups. The Kaplan-Meier survival curves revealed that only somatic symptom scores were associated with mortality among the tertiles (log-rank p < 0.001) (Fig. 3). The third tertile group of the somatic symptom domain showed poor survival compared to the first tertile and second tertile groups (p = 0.003 and p = 0.02, respectively) (Fig. 3C). Among the three depressive-symptom scores, only a high somatic symptom score was an independent risk factor for mortality (model 4: HR, 2.45; 95% CI, 1.25–4.79; p = 0.009) (Table 4). In the multivariate linear regression analysis, somatic symptoms negatively correlated with age and albumin level and positively with the male sex among older patients with ESKD (all p < 0.05) (Table 5).
Discussion
This Korean nationwide prospective cohort study revealed that severe depression increased the mortality risk in older patients with ESKD, whereas minimal and mild-to-moderate depression showed similar survival outcomes. The negative effect of severe depression on survival remained significant after adjusting for confounding factors. Among the three depressive symptom domains, only somatic symptoms were associated with mortality in the study cohort. In addition, older patients with a higher comorbidity index or lower albumin level had an increased risk of severe depression.
Over the decades, many studies have demonstrated an association between depression and mortality in patients with ESKD [2,3,9,11,22]. The cut-off values of BDI-II score for discriminating depression may change depending on the patient group and a definite cut-off value that could be applied consistently has not yet been determined. A study of hemodialysis patients aged 65 years and older showed that a BDI score of ≥10 had a diagnostic value of depression with a sensitivity of 68% and specificity of 77% [23]. In this background, a cut-off of 10 for the minimal depression group was acceptable as a value to discriminate depression. In addition, we referred to another study that reported the association between the severity of depression and patient survival. The study investigating hemodialysis patients with a mean age of 64 years showed that only moderate depression (BDI-II score, ≥20) was significantly associated with all-cause mortality [24]. Therefore, dividing patients into BDI-II tertile groups (minimal, 0–10; mild-to-moderate, 11–19; severe, ≥20) was considered appropriate to investigate outcomes of interest based on previous studies from a similar population.
With the progressive establishment of aging societies, evaluating the relationship between depression and mortality among older patients is important [25]. Among the screening tools for depression, the BDI-II is the most widely used for the chronic kidney disease population [1,23,26]. Depression increases the mortality risk in patients with ESKD [2,3,9–11,22]; however, the behavioral and biological mechanisms that fully explain the link between the two remain unclear [27]. Our results showed that the risk of severe depression increased in older patients with higher mCCI values. The presence of multiple comorbidities increases the burden of illness, such as selfcare demands and functional impairment, causing depression and poor therapeutic adherence [28–31]. The close association between depression, frailty, and mortality has been demonstrated in several studies [15,32]. In addition, hypoalbuminemia is linked to severe depression; therefore, depression may reflect a poor nutritional status. These depression-related factors may result in poor outcomes for older patients with ESKD.
Several studies have demonstrated a relationship between the BDI score and mortality in patients with ESKD, but not among older patients. Kimmel et al. [9] reported that higher time-varying BDI scores were associated with increased mortality in 295 patients with a mean age of 54.6 years on hemodialysis. However, a cumulative survival analysis showed a similar increase in mortality in the mild and moderate-to-severe depression groups compared with the minimal depression group, with no differences in the mortality risk between the mild and moderate-severe depression group [9]. A European multinational cohort study, using a sensitivity analysis, revealed that self-reported severe depression was significantly associated with all-cause mortality during the 11-month follow-up period among 3,086 patients with a mean age of 63.6 years undergoing hemodialysis [24]. Unlike previous studies, our study included a cohort of older patients with ESKD with a mean age of 74.2 years and showed that severe depression negatively impacted mortality compared with minimal or mild-to-moderate depression. To the best of our knowledge, this is the first study to investigate the association between depression and mortality among older patients with ESKD.
Few studies have investigated depression among Korean patients with ESKD. Recently, a nationwide cohort study analyzed psychiatric problems in patients with ESKD based on the code of International Classification of Disease, 10th revision; the hemodialysis and peritoneal dialysis groups had a greater depression risk than the kidney transplantation group [33]. In addition, patients with ESKD aged >60 years reportedly have a higher depression risk than those aged 18–39 years [33]. Contrary to our results, Jeon et al. [34] found no association between depression, as measured by the BDI, and all-cause mortality among 166 patients on hemodialysis. However, the mean age of patients was 57.9 years, which was younger than that in our study, and the 31.2-month follow-up period was much shorter than that in our study; therefore, their reports of the effects of depression among older patients with ESKD were limited [34].
Interestingly, our results demonstrated that each depressive symptom domain had a different relationship with mortality. Among the three domains, patients with higher scores for somatic, but not affective or cognitive, depression had higher mortality. This is consistent with a previous prospective study conducted in the Netherlands, which reported that only BDI-II score-derived somatic depressive symptoms affected mortality in 687 patients on dialysis [35]. Most patients on dialysis with depression have somatic symptoms; somatic and psychiatric symptoms are reportedly associated in patients on dialysis [36]. In our study, somatic symptoms negatively correlated with age among older patients. In other words, younger subsets of older patients with better physical capacity are more likely to experience physical and sexual dysfunctions compared with the older subsets. In a cross-sectional study, somatic symptoms were associated with low physical activity levels, measured using pedometry, in patients with ESKD [37]. Although our study did not measure the physical activity levels of patients, a higher somatic symptom score among younger subsets of older patients may reflect their discouragement due to discrepancies between their physical activity levels and expectations. These causal relationships should be further investigated.
This study had some limitations. First, this was an observational study; therefore, potential prognostic factors could not be considered, such as history of psychiatric disorder and antidepressants. Additionally, the causal relationship and pathophysiological mechanisms between depression and mortality could not be explained. Second, the depressive symptoms were similar to those observed in uremia. However, we did not investigate dialysis adequacy and prescription, which may have affected the symptoms. Third, since this study focused on the association between baseline depression and mortality in older patients with ESKD, no evidence regarding the effect of depression treatment and changes in the degree of depression on patient outcomes was generated.
In conclusion, we found that severe depression increases mortality in older patients with ESKD. Older patients with somatic depressive symptoms are a particularly vulnerable population and may require meticulous management of comorbidities and nutritional status to improve their outcomes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









