



Introduction
Sepsis-associated acute kidney injury (SAKI) is a life-threatening disease characterized by renal dysfunction through sepsis with high morbidity and mortality. Recent studies have elaborated that pathophysiological responses during SAKI mediate kidney impairment [1], leading to inflammation, renal blood hypoperfusion, and tubular epithelial cell death. Therefore, early detection and treatment access is beneficial to the prognosis of SAKI patients in the clinic. However, there are no effective and reliable biomarkers to date to predict the risk stratification and prognosis of SAKI. Previous studies have described a vital role of tumor necrosis factor alpha (TNF-╬▒) in the inflammatory process of SAKI, with insufficient sensitivity and specificity [2]. Therefore, it is essential to have an early, sensitive, and accurate biomarker to predict the severity and prognosis of SAKI, which could alleviate renal injury and poor outcomes.
Interleukin (IL)-17A, as one of the IL-17 family members, is mainly secreted by CD4+ T cells and can be secreted by nature killer T cells, neutrophils, CD8+ T cells, and ╬│╬┤ T cells [3]. Initially, IL-17A indicates a proinflammatory role in protecting against microbial infections during several inflammatory diseases. Meanwhile, IL-17A interacts with inflammatory cytokines, like IL-22, IL-1╬▓, and TNF-╬▒, resulting in a worse result [4]. Once infected, IL-17A can mediate neutrophil recruitment, host defense, and inflammation, leading to overt tissue damage [5]. Some studies have revealed that IL-17A produced in the peritoneal cavity by the ╬│╬┤ T cells at the early phase of sepsis is rapidly detected in the circulation [6]. IL-17A is released within 6 hours after the mild renal ischemia-reperfusion injury (IRI) [7]. Besides, activation of toll-like receptor (TLR) 2 facilitates the generation of IL-17A, leading to cisplatin-induced acute kidney injury (AKI) by recruiting innate effector cells. Therapeutic IL-17A antibodies have been shown to protect mice from cisplatin-induced AKI [8]. However, little is known about the contributions of IL-17A to SAKI progression in humans.
Considering the high morbidity and mortality of SAKI, it is essential to study the poorly known roles of IL-17A in risk stratification and prognosis in humans. Therefore, this research aims to evaluate the prognostic values of IL-17A in SAKI patients from the emergency department.
Methods
A total of 146 patients between 18 to 80 years old and hospitalized with sepsis in the emergency department from Nov 2020 to Nov 2021 were enrolled in the study. All patients admitted to the hospital completed promptly the Acute Physiology and Chronic Health Evaluation II (APACHE II) within 24 hours. Eighty-four sepsis patients without acute kidney injury who were hospitalized were included in the control group. The exclusion criteria for the study were anyone under 18 or over 80 years, chronic kidney disease, connective tissue disease, cancer, and congenital and acquired immunodeficiency. Patients were also excluded if any inflammatory cytokines were missed. The origin of infection included pneumonia, urinary infection, intraabdominal infection, soft tissue infection, and others.
The diagnostic criterion of sepsis is formulated using the Sepsis-3 definition [9]. SAKI diagnosis is usually based on AKI in the presence of sepsis, characterized by the Kidney Disease: Improving Global Outcomes (KDIGO) criteria [10]. Based on the serum creatinine or urine output, patients were divided into those diagnosed with acute kidney injury (SAKI group) and those who did not suffer from acute kidney injury (non-SAKI group). The AKI patients were divided into three groups based on the KDIGO guidelines: stages 1, 2, and 3. Furthermore, we divided SAKI patients into survival and non-survival group based on the 28-day mortality.
All the clinical parameters were evaluated on admission. Before initiating antibiotic treatment, the peripheral blood, urine, and other bodily fluid samples were collected. IL-2, IL-4, IL-6, IL-17A, TNF-╬▒, and interferon gamma (IFN-╬│) levels were assessed by FACSCalibur flow cytometer (BD Biosciences) based on the manufacturerŌĆÖs instructions. C-reactive protein (CRP) and procalcitonin (PCT) were tested by Pylon 3D Automated Immunoassay System (ET Healthcare). In addition, the creatinine and white blood cell count (WBC) were evaluated by the clinical laboratory at Tianjin Medical University General Hospital.
The IBM SPSS version 19.0 (IBM Corp.) was used for statistical analyses. Numerical data with normal distribution were presented as mean ┬▒ standard deviation. The t test was used to compare two groups, and one-way analysis of variance was used to compare three or more groups. Quantitative data with non-normally distributed variables were represented as median with interquartile range. The Mann-Whitney U test was used for comparisons between two groups and the Kruskal-Wallis test was used for comparisons among three or more groups. A logistic regression analysis model was performed to assess the risk factors involved in the mortality of SAKI. The receiver operating characteristic (ROC) curves were implemented to analyze the area under the curve (AUC) of clinical indicators, thus assessing the prognostic values of clinical indicators in SAKI. Cox regression was utilized to evaluate the prognostic analysis. Net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were used to compare the predictive accuracy of inflammatory cytokines. A p-value of <0.05 was considered statistically significant.
The study protocol was approved by the Medical Ethics Committee of Tianjin Medical University General Hospital (No. IR2021-YX-188-01) and was conducted in accordance with the Helsinki Declaration of 1964 (revised 2008). All the patients gave informed consent to enter the study.
Results
Characteristics of study participants
The demographic and clinical characteristics of the study are presented in Table 1. There was no statistical significance between the non-SAKI and SAKI groups concerning age, sex, APACHE II, WBC, and IFN-╬│ among all the patients. However, the levels of creatinine, IL-2, IL-4, IL-6, IL-17A, TNF-╬▒, CRP, and PCT were significantly higher in the SAKI group than those in the non-SAKI group (p < 0.05). In addition, the mean length of hospitalization was significantly longer in the SAKI group (hospitalized for 15.5 ┬▒ 7.5 days) than in the non-SAKI group (hospitalized for 12.1 ┬▒ 6.3 days) (p = 0.02).
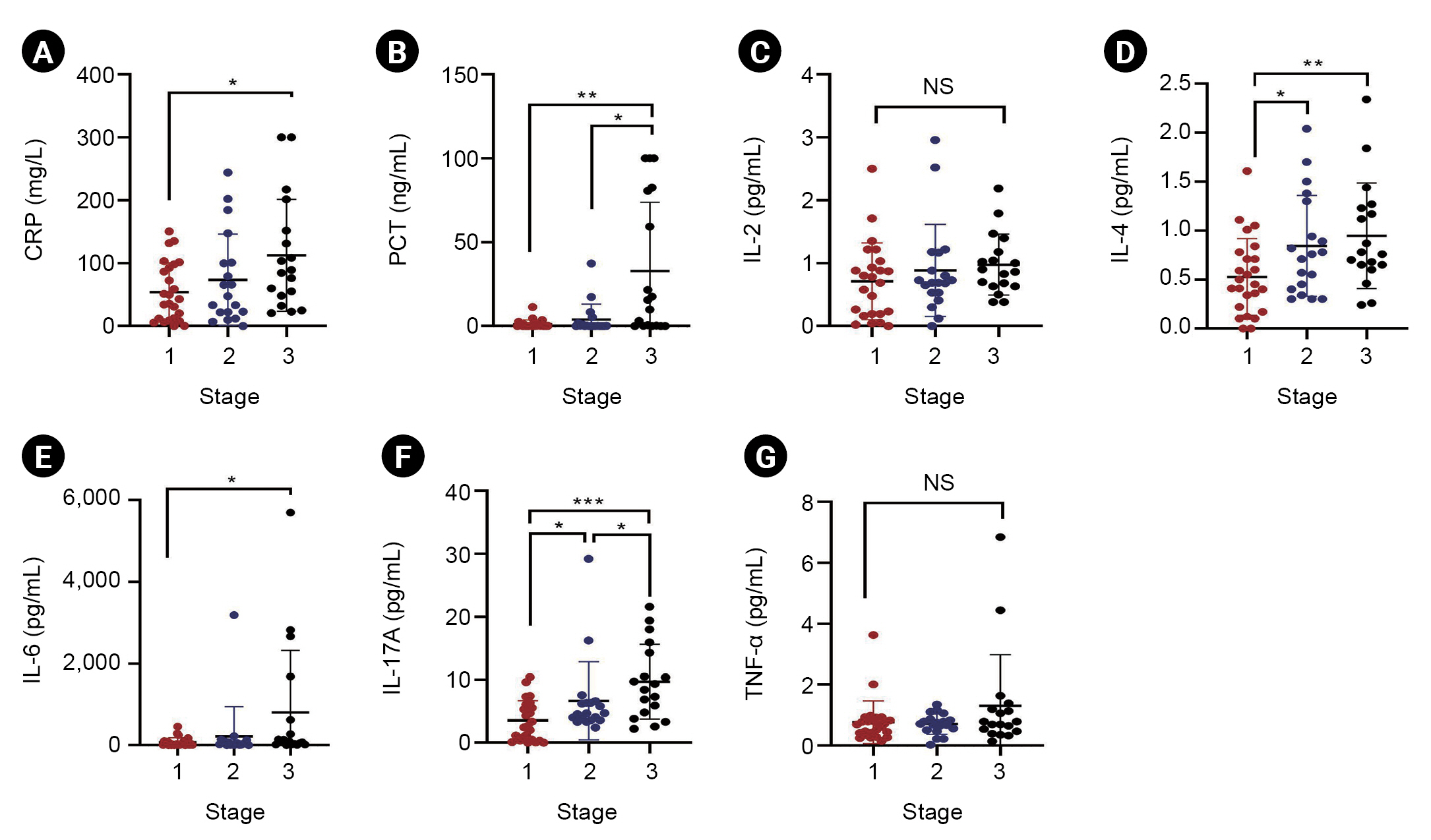
Comparison of inflammatory cytokines in sepsis-associated acute kidney injury patients based on the severity
Based on the severity, SAKI patients were divided into three groups: stage 1 (n = 25), stage 2 (n = 19), and stage 3 (n = 18). There was a significant difference in PCT, IL-4, IL-6, and IL-17A levels based on the severity of SAKI (Fig. 1). IL-4 and IL-17A levels in the stage-2 group were significantly higher than in the stage-1 group (p = 0.049 and 0.04, respectively). Compared to the stage-2 group, PCT and IL-17A levels were significantly higher in the stage-3 group (p = 0.01 and 0.048, respectively). The results indicated that IL-17A was more promising than other clinical indicators in predicting the severity of SAKI.
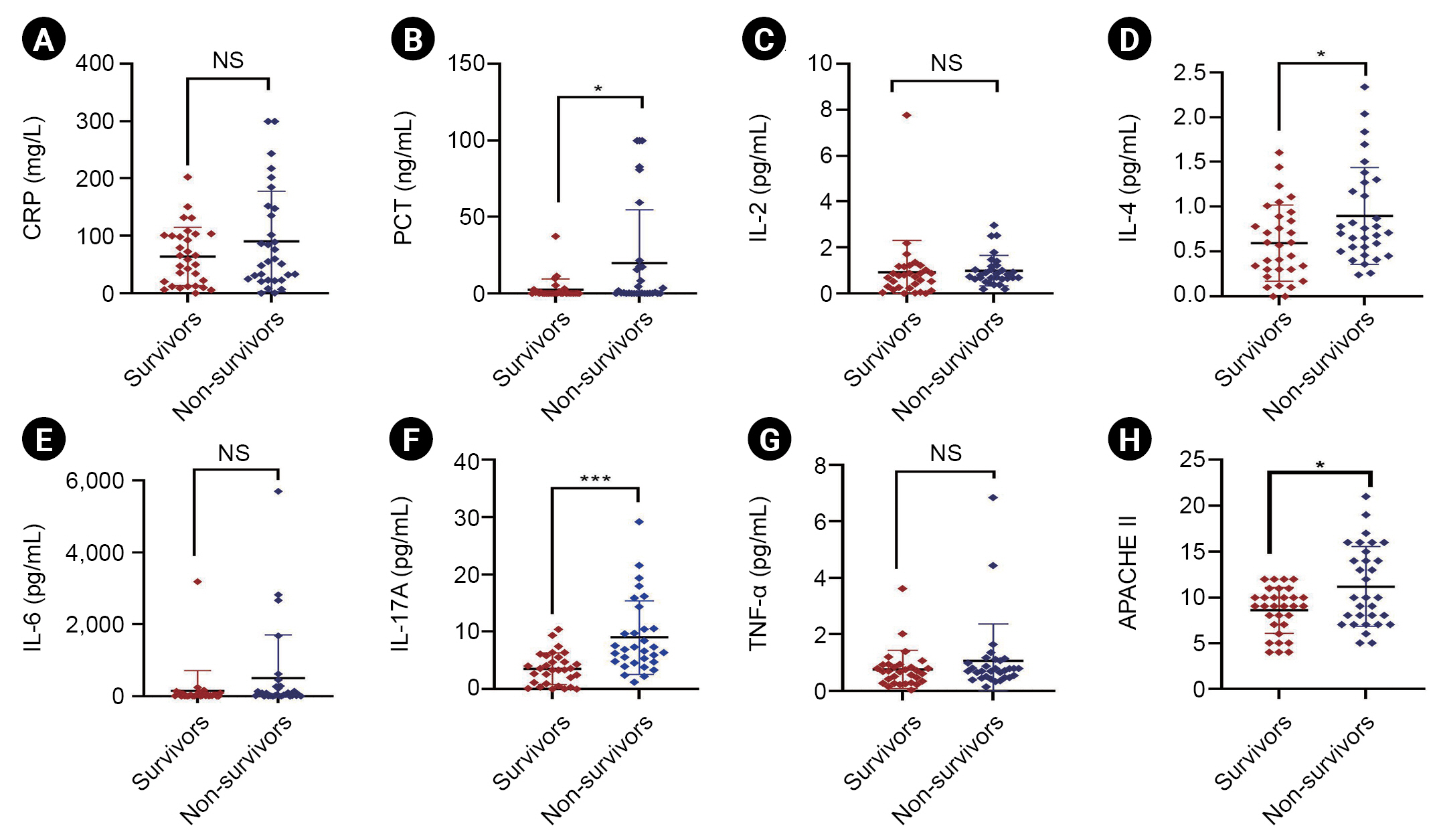
Association between the inflammatory cytokines and prognosis in sepsis-associated acute kidney injury
We assessed the predictive value of inflammatory cytokines on prognosis during the 28-day mortality of SAKI and non-SAKI patients. The mortality of the non-SAKI group and SAKI group reached 25% and 50%, respectively. Non-survivors showed significantly increased APACHE II, PCT, IL-4, and IL-17A levels than survivors in the SAKI group (p < 0.05). However, there was no statistical significance in CRP, IL-2, IL-6, and TNF-╬▒ levels between the non-survival and survival groups in SAKI patients (p > 0.05) (Fig. 2). Additionally, the mean length of hospitalization also did not reveal any significant difference between the two groups (p > 0.05). Besides, the prognostic value of inflammatory cytokines in non-SAKI patients was shown in Supplementary Table 1 (available online).
Logistic regression analysis of mortality in sepsis-associated acute kidney injury
As shown in Table 2, logistic regression analysis was used to assess mortality risk factors in SAKI. According to the results of prognosis, the levels of IL-17A, IL-4, and PCT were analyzed as the independent variables in logistic regression analysis. It was demonstrated that IL-17A was an independent factor that could predict the 28-day mortality of SAKI (odds ratio, 1.423; 95% confidence interval, 1.102ŌĆō1.839; p = 0.007). However, the levels of IL-4 and PCT were not the independent risk factors of SAKI (p > 0.05). Based on the result of logistic regression analysis, a prediction model was proposed as follows: ŌĆō2.408 + 0.353 ├Ś (IL-17A) + 0.114 ├Ś (IL-4) + 0.055 ├Ś (PCT).
Receiver operating characteristic analysis of the inflammatory cytokines in sepsis-associated acute kidney injury
We demonstrated that IL-17A had higher and superior sensitivity and specificity than other inflammatory cytokines in predicting the prognosis of SAKI. The AUC-ROC curve for sepsis prognosis in IL-17A was 0.811 (Table 3). The sensitivity was 77.4%, and the specificity was 71.0%, at a 4.7 pg/mL cutoff value. Therefore, the ROC curve revealed that of all the inflammatory cytokines assessed, IL-17A had the most potential in the prognosis of SAKI (Fig. 3A). The survival curves were established based on the cutoff value of 4.7 pg/mL of IL-17A (Fig. 3B). There was a significant difference in survival rates of SAKI as stratified based on the IL-17A on the day of admission. Patients with higher IL-17A levels showed worse outcomes than low levels.
Net reclassification improvement and integrated discrimination improvement of the inflammatory cytokines in sepsis-associated acute kidney injury
Compared with an IL-4 model, the IL-17A model resulted in an NRI of 0.26 (p < 0.05) and an IDI of 0.20 (p < 0.01), indicating a positive improvement. Compared with the PCT model, the IL-17A model had an IDI of 0.17, indicating the IL-17A model could increase the predictive accuracy by 0.17 (p < 0.05). However, NRI showed no significant difference between IL-17A and PCT models (p = 0.19).
Discussion
In recent years, many studies have revealed that a dysfunctional inflammatory response could result in organ dysfunction, wherein inflammatory indicators, primarily cytokines, play a crucial role in developing kidney injury during sepsis [11]. Various biomarkers have been utilized to diagnose and predict the mortality of SAKI. However, most conventional biomarkers are released and detected at a later phase of SAKI with low sensitivity and specificity. Previous meta-analyses suggested that urinary IL-18 had also been studied to predict AKI in severe sepsis patients with a low AUC [12]. Serum neutrophil gelatinase-associated lipocalin (NGAL) failed to discriminate AKI from non-AKI in sepsis patients [13]. PCT was not associated with mortality in critically ill patients with low sensitivity and specificity [14]. Therefore, an early and reliable biomarker could be essential to assess the severity and prognosis of SAKI clinically. In our studies, we demonstrated that IL-17A is more capable of predicting the severity and mortality at the early stage of SAKI.
The role of IL-17A had been previously studied in infectious and renal diseases [15,16]. However, the potential role of IL-17A in SAKI was rarely reported, especially the clinical ability to predict the severity and prognosis. The increasing level of IL-17A is detected in plasma and tissues of animal models during sepsis associated with organ damage [17,18]. There is evidence that TLR9 activated the myeloid dendritic cells to produce IL-23, which induced ╬│╬┤ T cells to synthesize IL-17A in septic mice and contributed to septic AKI development [19]. IL-17A is elevated in animal models of acute tubular injury and cisplatin-induced AKI [20]. The signal pathways of IL-17A and IFN-╬│ activated by upstream IL-23 and IL-12 promoted inflammatory response in mice with renal IRI [21]. Moreover, IL-17 knockout mice can defend against SAKI by decreasing the proinflammatory cytokine levels and reducing neutrophil infiltration followed by apoptosis of tubular epithelial cells [22].
Our study indicated that IL-17A could assess the severity of SAKI. PCT, IL-4, IL-6, and IL-17A levels were significantly different based on the severity of SAKI (p < 0.05). Compared with the other cytokines evaluated, IL-17A efficiently predicted the severity in SAKI patients. Liu et al. [23] reported that increasing IL-17A was associated with significantly worse disease severity and unfavorable prognosis in sepsis patients, concurrent with our results. The high levels of IL-17A in septic shock activated the proinflammatory cytokines (IL-1╬▓, TNF-╬▒, and IL-6) and chemokines [24]. Besides, IL-17A levels correlated with disease severity in patients having lupus nephritis, in which cytokines like TNF-╬▒, could attract inflammatory cells into the kidney [25]. A previous study showed that IL-17A served as an optimal biomarker to determine the severity and prognosis of sepsis-induced acute respiratory distress syndrome (ARDS) [26]. Furthermore, tubular damage and interstitial infiltration were alleviated in the IL-17A knocked-out mice [20,27]. In contrast, Thorenz et al. [7] demonstrated that IL-17A deficiency or treatment of IL-17A antibody could not attenuate renal fibrosis after severe IRI in mice.
Our study also indicated that IL-17A had the highest sensitivity and specificity to predict the prognosis of SAKI compared to IL-4 and PCT. Most of the initial IL-17A in the kidney was secreted by neutrophils, directly damaging kidney and tubular cells [19]. Moreover, IL-17A induced neutrophil infiltration and tubular cell apoptosis [22]. IL-17A acted as a driver of developing AKI in septic shock patients and was found to be deposited heavily in the glomeruli by renal biopsies of patients, who died of dengue fever [27,28]. Mikacenic et al. [3] had also shown that increased circulating levels of IL-17A were potential indicators of organ dysfunction in ARDS. Similar to the report by Ahmed et al. [18], we found that non-survivors had significantly elevated levels of IL-17A compared with survivors among SAKI patients, demonstrating that high levels of IL-17A were associated with mortality and poor outcomes in SAKI patients. However, we only studied the patients who suffered from SAKI and not poly-trauma. In animal experiments, Naito et al. [19] confirmed that the knockout of IL-17A improved outcomes post-cecal ligation and puncture (CLP) and attenuated the septic AKI. Moreover, the role of IL-17A in sepsis mortality might depend on the microbe that initiated the infection. IL-17A elevated the recruitment of neutrophils, which were unable to phagocytose the bacteria [29]. On the contrary, some animal experiments had revealed that IL-17 played a protective role in less severe CLP models. Compared to IL-17ŌĆō/ŌĆō mice, wild-type mice had significantly higher survival after CLP [30,31]. Therefore, more well-conducted trials are required to assess the role of IL-17A in SAKI.
There are several limitations to our study. First, it is a retrospective study and involves a small size of patients from a single center. Secondly, IL-17A was measured at baseline only within 24 hours after admission and dynamic monitoring was not presented, which might make the results imperfect. Thirdly, some other biomarkers, such as NGAL and IL-18, were not included in the study, which might have a potential effect on the results.
In conclusion, elevated IL-17A might indicate poor mortality in SAKI patients. Further studies are needed to elucidate better the usefulness of IL-17A in the therapy of SAKI.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









