


A 54-year-old man visited our hospital with symptoms of abdominal pain and generalized skin rash that had developed over several weeks. He had no history of diabetes mellitus, except alcoholic liver cirrhosis (LC). Laboratory investigations revealed that the serum creatinine, albumin, hemoglobin, and platelet levels were 0.95 mg/dL, 2.3 g/dL, 10.0 g/dL, and 49,000/μL, respectively. Urinalysis showed severe proteinuria. Antineutrophil cytoplasmic antibody was not detectable. Serum C3 was decreased.
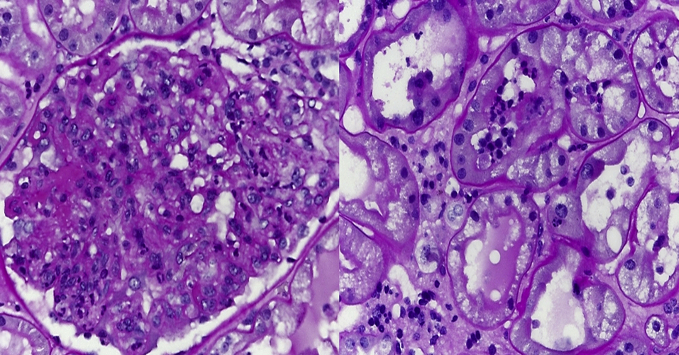
Colonoscopy revealed ulcerative lesions along the transverse colon, and abdominal computed tomography revealed severe bowel edema along the entire colon (Fig. 1). We immediately administered intravenous fluid therapy. However, uremic symptoms were newly developed. A renal biopsy was performed because of aggravation of renal function. It showed the following: capillary lumens occluded by several inflammatory cells in most glomeruli, infiltration of lymphocytes in the interstitium and tubules, and diffuse mesangial proliferation with cellular crescent (Fig. 2). Immunofluorescence microscopy stains were strongly positive for IgA and C3 in the mesangium. We initiated treatment with steroids and cyclophosphamide for the crescentic glomerulonephritis. However, we could not continue immunosuppressants because of adverse events including gastrointestinal bleeding and pneumonia. Ultimately, the patient received regular hemodialysis, and his symptoms improved completely.
The infiltration of IgA immune complexes is related to the degree of liver damage in LC, especially. Henoch–Schönlein purpura (HSP) nephritis can often be developed in adult patients with LC. Because HSP nephritis in an adult indicates a poor prognosis, treatment should be initiated immediately. As in this case, the cytotoxic management for HSP nephritis with crescent in patients with LC can result in severe adverse outcomes. Therefore, an early dialysis in patients with HSP nephritis with crescent formation and alcoholic LC can be one of the best treatment options.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









