Renal infarction caused by spontaneous renal artery dissection after playing golf
Article information

A 59-year-old man presented to our clinic with severe left flank pain after vigorous golfing. The patient exhibited tenderness at the left costovertebral angle. He had a history of hypertension and diabetes, both of which were well-controlled with medication. No recent trauma or endovascular procedures were reported. Laboratory tests showed elevated C-reactive protein (5.3 mg/dL) levels, but complete blood cell counts, creatinine levels, and urinalysis were unremarkable. A serum cholesterol test showed total cholesterol levels of 129 mg/dL, low-density lipoprotein cholesterol levels of 58 mg/dL, and triglyceride levels of 141 mg/dL. Computed tomography (CT) revealed a left renal infarction and the presence of dual left renal arteries with narrowing and irregularity in the left upper renal artery with an intraluminal hematoma, suggesting renal artery dissection. A 1.5-cm aneurysmal dilatation was also noted (Fig. 1A). CT angiography excluded other underlying arteriopathies, such as atherosclerosis, fibromuscular dysplasia, or connective tissue disorders (Fig. 2). Electrocardiogram and 24-hour Holter monitoring revealed normal sinus rhythm without arrhythmias. Echocardiography revealed the absence of intracardiac masses or thrombi. Laboratory tests revealed no abnormalities in coagulation. We suspected that spontaneous renal artery dissection (SRAD) caused the acute infarction in the left kidney. To prevent thrombosis at the site of endothelial damage and propagation of the dissection, anticoagulation was initiated with enoxaparin (1 mg/kg every 12 hours) and switched to oral warfarin. Oral warfarin therapy was continued for 6 months, aiming for an international normalized ratio range of 2 to 3. A follow-up CT scan revealed segmental atrophy of the left kidney, recovery of luminal flow in the dissected left upper renal artery, disappearance of the intraluminal thrombus, and regression of the aneurysm (Fig. 1B). Oral warfarin was discontinued and switched to low-dose aspirin as no thromboembolic risk factors were identified. No recurrence was noted during the 3-month follow-up period. Written informed consent was obtained from the patient for the publication of this report including all clinical images.
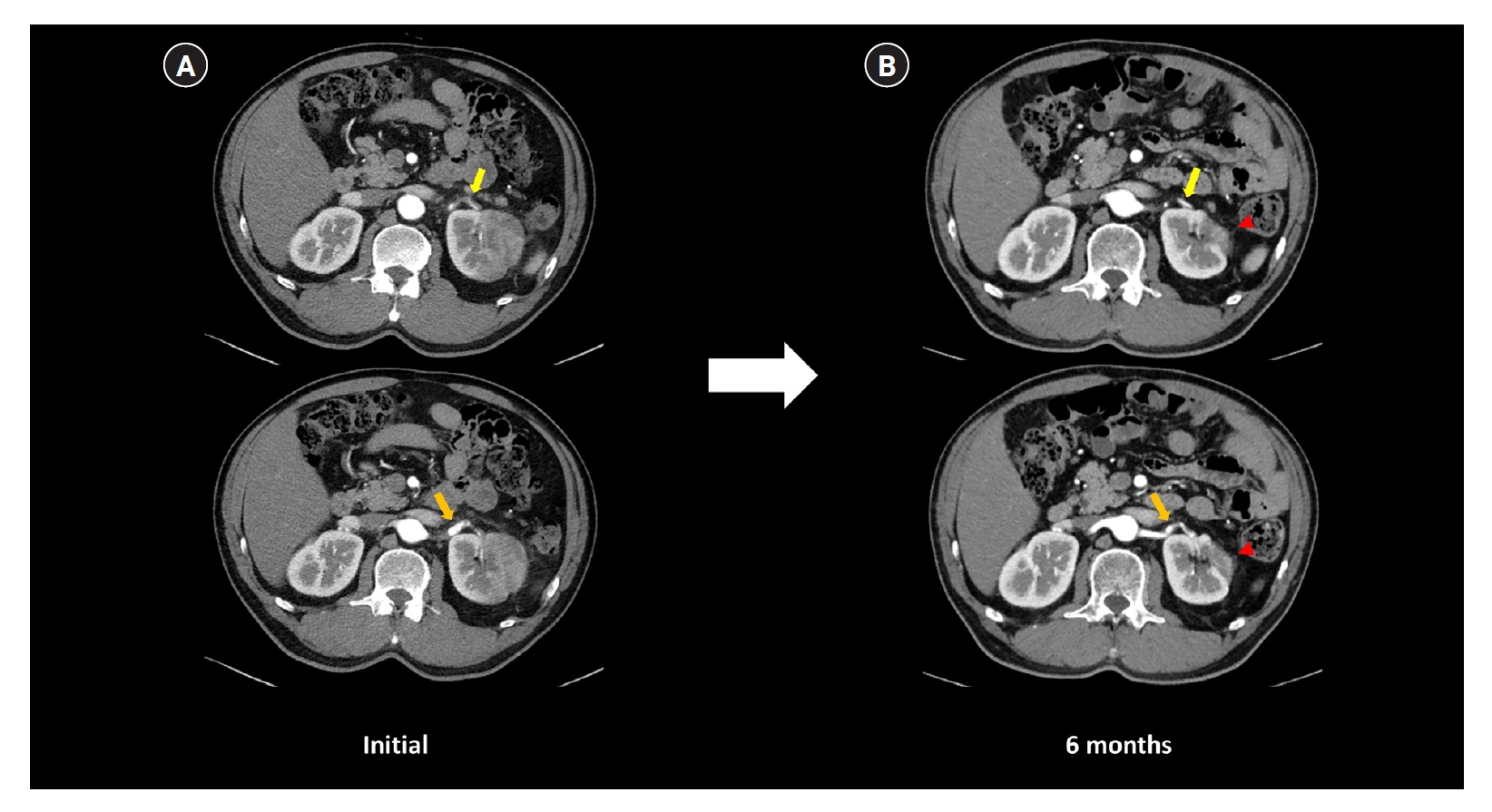
CT images at initial presentation and 6-month follow-up with warfarin therapy.
(A) Initial kidney CT scan shows luminal narrowing and irregularity of the left upper renal artery with intraluminal hematoma, suggesting renal artery dissection (yellow arrow, upper image) and a 1.5 cm aneurysmal dilatation proximal to the dissection site (orange arrow, lower image). (B) Follow-up CT scan after 6-months of warfarin therapy shows segmental atrophy of the infarcted site of the left kidney (red arrowheads), along with the recovery of luminal flow (yellow arrow, upper image), disappearance of the intraluminal thrombus (yellow arrow, upper image), and regression of the aneurysm (orange arrow, lower image) in the left upper renal artery. CT, computed tomography
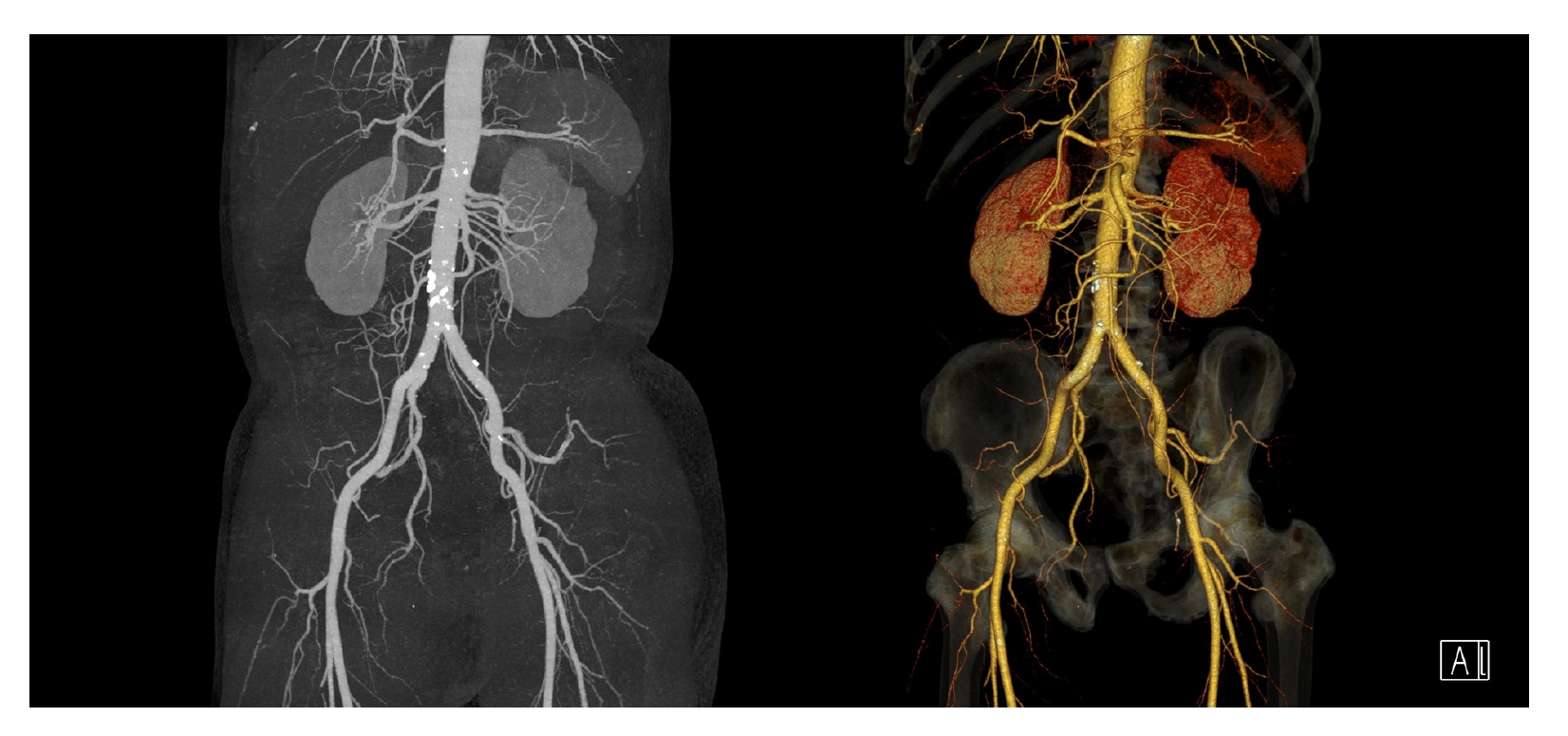
CT angiography image.
CT angiography shows no evidence of arteriopathies such as atherosclerosis, fibromuscular dysplasia, or connective tissue disorders in the aorta and its branches, including renal arteries. CT, computed tomography
SRAD is a rare condition with few case reports on its occurrence after exercise. Renal infarction secondary to SRAD is even more uncommon. SRAD may occur during golfing owing to intimal tearing, which can be caused by direct stretching or acceleration and deceleration forces. SRAD should be considered in patients presenting with acute flank pain after strenuous exercise. Based on previous reports, we did not consider surgical or endovascular treatment as the patient’s blood pressure was effectively controlled and renal function remained stable under conservative treatment with anticoagulation. He achieved a good clinical outcome with medical treatment alone.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Data sharing statement
The data presented in this study are available on reasonable request to the corresponding author.
Authors’ contributions
Conceptualization: All authors
Data curation: SHJ, JHO, AYC, IOS, KYL, HL
Formal analysis: SHJ, HL
Visualization: SHJ, DMK, HL
Supervision: HL
Writing–original draft: SHJ
Writing–review & editing: HL
All authors have read and approved the final manuscript.