Remaining life expectancy of Korean hemodialysis patients: how much longer can they live?
Article information

Abstract
Background
Hemodialysis (HD) patients have a higher mortality rate compared to the general population. However, no study has investigated life expectancy in Korean HD patients so far. Therefore, this study aimed to calculate the remaining life expectancy among Korean maintenance HD patients and compare it to those of the general population as well as HD patients from other countries.
Methods
Baseline data were retrieved from HD quality assessment data from 2015. Among the patients over 30 years old who were alive at the beginning of 2016 (20,304 males and 14,264 females), a total of 22,078 (12,621 males and 9,457 females) were still alive at the end of 2021 while 12,490 (7,683 males and 4,807 females) were deceased during 6 years of follow-up. We used the life table method to calculate the expected remaining years of life in 2-year increments.
Results
The remaining life expectancies for 60-year-old patients were 11.64 years for males and 14.64 years for females. The average remaining life expectancies of the HD population were only about half of the general population. Diabetic patients demonstrated shorter life expectancy compared to patients with hypertension or glomerulonephritis. The remaining life expectancy of Korean HD patients was similar to that of Japanese and was almost double that of HD patients in Western countries such as Europe and the United States.
Conclusion
The HD population shows a shorter life expectancy compared to the general population. Longitudinal analysis should be warranted to analyze the effect of advanced dialysis technology on improved survival rates among the HD population.
Introduction
The number of patients with end-stage kidney disease (ESKD) increased tremendously causing increased health burden worldwide [1,2]. The number of ESKD patients who begin dialysis therapy doubled in the last 10 years in Korea [3]. The increase in diabetic patients and the elderly is one of the many causes contributing to the increase in the dialysis population [4,5].
The ESKD patients not only cause increased medical expenses but also demonstrate a high morbidity and mortality rate. Although dialysis treatment improved the survival rate of ESKD patients in past decades [6,7], hemodialysis (HD) patients have a much higher mortality rate than the age- and sex-matched general population [8]. The mortality rate from ESKD is even higher than that of regional breast cancer, colon cancer, and kidney cancer [8].
Age-specific life expectancy is a commonly used measure to estimate the impact of health status and disease burden at a population level [9]. Policymakers can use it to identify disease conditions that have the greatest impact on overall life expectancy and to prioritize specific health programs or funding [10]. Although there are a few research papers investigating risk factors and mortality trends in Korean maintenance HD patients [3,11], there has been no study calculating the remaining lifespan among maintenance HD patients in Korea. Therefore, this study was performed to calculate the remaining life expectancy among Korean maintenance HD patients and compare it to those of the general population as well as HD patients from other countries.
Methods
Study population and data collection
This is a longitudinal observational cohort study of Korean patients with maintenance HD. We used HD quality assessment data from the Health Insurance Review and Assessment Agency (HIRA) in 2015. The mortality data were collected from January 2016 to November 2021. The HD quality assessment data were collected by each HD facility through a web-based data collection system from October to December 2015. Adult HD patients who received HD treatment at least twice a week were included in the HD quality assessment data. The data were collected from outpatient HD patients, and those who were hospitalized or transferred to other facilities were excluded from data collection. Among 34,941 patients, we excluded 373 patients under 30 years old and included a total of 34,568 patients over 30 years old in the current analysis. Baseline clinical and demographic data were obtained from the HIRA database. Demographic data included age, sex, dialysis duration, body mass index, cause of ESKD, and health insurance status. The death of a patient was recognized from the date of loss of insurance eligibility from the HIRA database.
The research was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Hallym University Kangnam Sacred Heart Hospital (No. 2021-11-043). As the study subjects were de-identified, the written informed consent was waived.
Remaining life expectancy calculation
We calculated the remaining life expectancy of HD patients using the life table method [9]. In order to calculate the remaining life expectancy, we firstly obtained the number of patients by age who were alive and receiving dialysis by the end of 2015 (20,304 males and 14,264 females), which can be interpreted as the number of patients alive at the beginning of 2016. Second, we obtained the number of patients who were still alive at the end of 2021 (12,621 males and 9,457 females). Lastly, the number of patients by age who had died by the end of 2021 (7,683 males and 4,807 females) was obtained. The life expectancy at each age was calculated using a life table describing the population’s death rate, the number of survivors and deceased individuals, and the static population. Life expectancy at the age of x can be calculated from a static population of x years or older divided by the number of survivors at the age of x. Patients’ ages were stratified by 2-year increments before analysis.
We have adjusted the age, sex, and cause of ESKD for calculating life expectancy. We computed the expected remaining years of life separately for males and females because the number of males and females in each age group differed. Based on the cause of ESKD, we divided patients into three groups (diabetes mellitus, hypertension, and glomerulonephritis) and calculated the remaining life expectancy in each group. When we compared the life expectancy, we excluded the patients over 80 years old because the number in each age group was less than 30 years. We compared the life expectancy according to the cause of ESKD, i.e., diabetes mellitus to hypertension ratio (DH-R), diabetes mellitus to glomerulonephritis ratio (DG-R), or hypertension to glomerulonephritis ratio (HG-R).
Comparison of remaining life expectancy between hemodialysis patients and the general population
We compared the remaining life expectancy of HD patients in 2016 to the remaining life expectancy of the general population in Korea from the same year. For the general population, we used values from data published by Statistics Korea [12]. We extracted the expected remaining years of life per decade of age for HD patients and the general population to calculate the ratio of the remaining life expectancy of dialysis patients to the general population, i.e., the HD patient to general population ratio.
Comparison of remaining life expectancy among hemodialysis patients from different countries
We compared the life expectancy of Korean HD patients with that of patients in Japan, the United States, and Europe [6–8]. The life expectancy data for each country was collected at different times. The remaining life expectancy of Japanese patients was based on the Japan Society for Dialysis Therapy (JSDT) Renal Data Registry database in 2015 [13]. The expected remaining years of life for the United States patients was based on the United States Renal Data System (USRDS) from 2016 [14]. For European dialysis patients, the life expectancy was based on the European Renal Association (ERA) registry from 2011 to 2015 [15].
Since the JSDT registry calculated the remaining life expectancy every 1 year while the USRDS and ERA registry published the life expectancy of patients every 5 years, we used the median of the 5-year age range in the Japanese data to compare the remaining life expectancy of HD patients in other countries. We computed the ratio of the remaining life expectancy of Korean dialysis patients to the remaining life expectancy of Japanese, European, and the United States dialysis patients and referred to each as the ratio of Korean dialysis patients to Japanese dialysis patients (KJ-R), Korean dialysis patients to the United States dialysis patients (KU-R), and Korean dialysis patients to European dialysis patients (KE-R).
Results
Baseline characteristics of hemodialysis patients
A total of 34,568 HD patients from 797 facilities were included in the analysis. Mean age was 60.5 ± 12.4 years old, and 58.7% were male. The average duration of HD was 5.63 ± 5.11 years. The most common cause of ESKD was diabetes mellitus (n = 14,523, 42.0%), followed by hypertension (n = 9,359, 27.1%) and glomerulonephritis (n = 3,780, 10.9%). The proportion of the patients on Medicaid was 23.0%.
Remaining life expectancy of Korean hemodialysis patients
Among 34,568 HD patients, a total of 12,490 patients (7,683 male and 4,807 female) died during 6-year follow-up. Table 1 shows the remaining life expectancy of Korean HD patients. On average, 30-year-old HD patients are expected to live until 60.9 years old while 60-year-old HD patients are expected to live until 72.8 years old. Females tended to have a longer life expectancy compared to males at about the same age. When we compared the remaining life expectancy of HD patients according to the cause of ESKD, the patients with diabetic nephropathy showed the shortest life expectancy compared to hypertensive nephropathy or glomerulonephritis (Table 2). However, the differences in life expectancy were negligible in older age (Fig. 1).

Remaining life expectancy of Korean hemodialysis patients
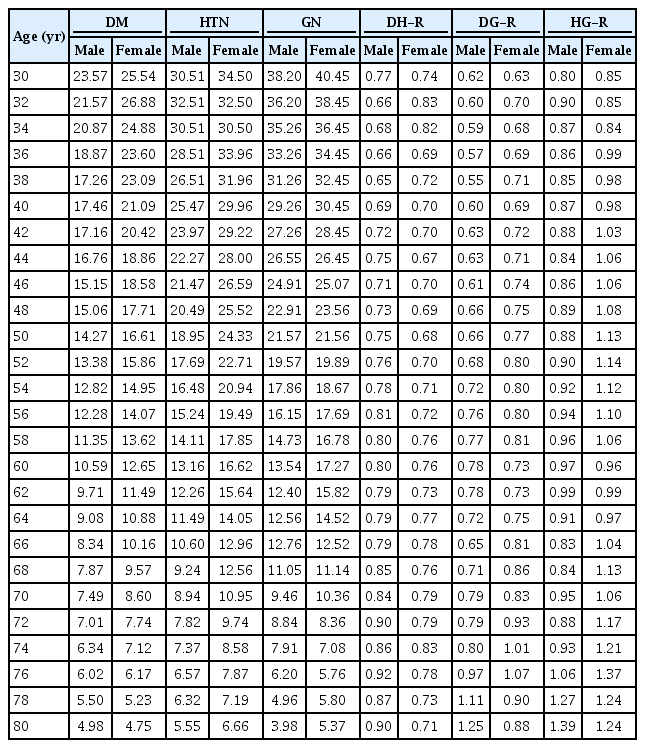
Remaining life expectancy of Korean HD patients according to the cause of ESKD

Remaining life expectancies in the maintenance hemodialysis patients according to the cause of end-stage kidney disease.
DM, diabetes mellitus; GN, glomerulonephritis; HTN, hypertension.
Comparison of remaining life expectancy between hemodialysis patients and the general population
We retrieved the remaining life time of the general population from the official website of Statistics Korea [12]. Since the life table of the general population in 2016 is demonstrated in 5-year increments, we calculated the remaining life expectancy of HD patients in 5-year increments for comparison. Korean HD patients demonstrated about 16% to 63% life expectancy compared to the general population of the same age group (Fig. 2; Supplementary Table 1, available online). The HDG-R was similar between males and females.
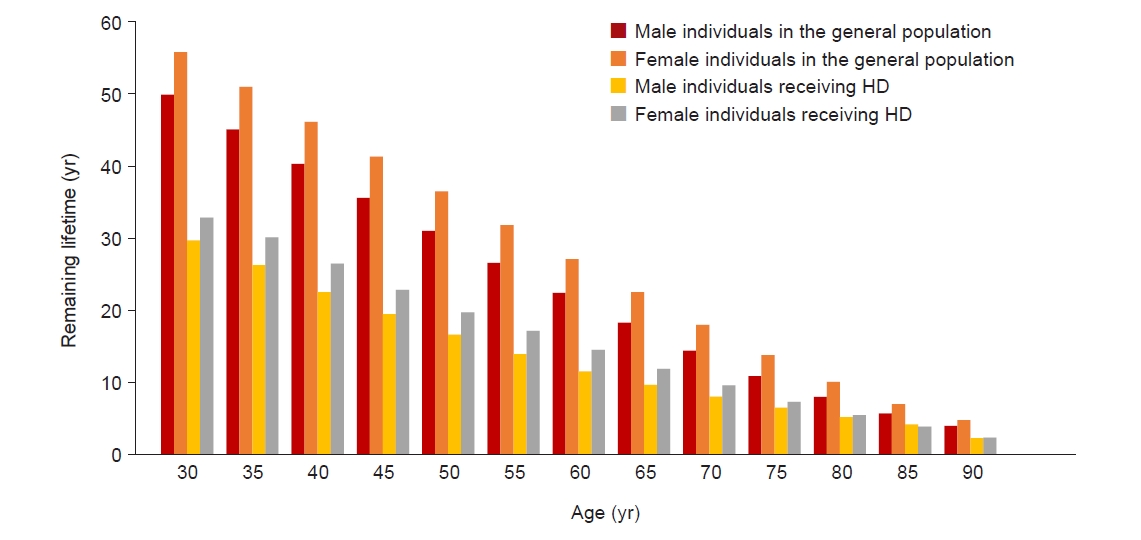
Remaining life expectancies in the maintenance hemodialysis (HD) patients compared to the general population in Korea.
Comparison of remaining life expectancy among hemodialysis patients from different countries
Table 3 demonstrates the comparison of life expectancy among HD patients in different countries. Korean HD patients showed a similar remaining life expectancy with Japanese HD patients. The KJ-R ranged from 0.93 to 1.26 in males and 0.98 to 1.26 in females. However, both Korean and Japanese HD patients showed 1.5 to 2 times longer life expectancy compared to European or American HD patients.
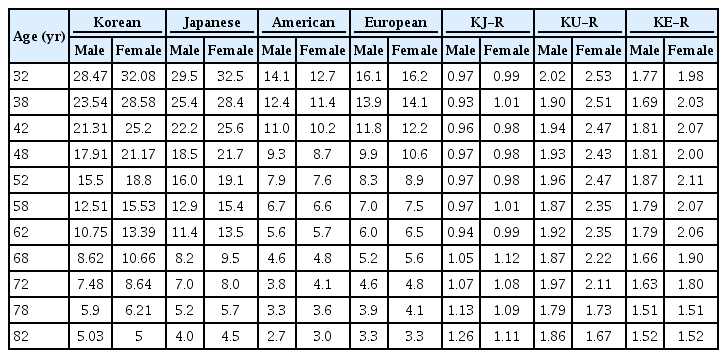
Comparison of the remaining life expectancy of hemodialysis patients between Korea, Japan, the United States, and Europe
Discussion
Universally, the incidence and prevalence of ESKD patients on renal replacement therapy increased while the mortality rate decreased over decades [3,14,15]. The possible reasons for the longevity of HD patients not only include improvement in dialysis-related technologies and new drugs but also may include improvement in the dialysis environment and policy [2,16]. Nevertheless, ESKD patients still demonstrate a high rate of hospitalization and mortality due to decreased immune function and multiple comorbidities.
Our study showed that HD patients have a shorter life expectancy compared to the general population. A previous study by the Italian Dialysis and Transplantation Registry also demonstrated that the dialysis population has shorter relative survival compared to the general population [8]. Our study also demonstrated that male patients have shorter survival compared to females, which is in line with the previous studies performed in Japan [13,17]. The differences in life expectancy between sexes became negligible in HD patients older than 80 years. This finding is also in line with the previous Japanese study [13]. However, interestingly, American or European HD patients did not show differences in life expectancy between the sexes. Indeed, American female HD patients even showed shorter remaining life expectancys at younger ages (Table 3). The previous study performed among the United States incident HD patients using data from the Dialysis Outcomes and Practice Patterns Study also demonstrated no difference between sexes in mortality [18]. The different phenomena between Asian and Western countries may be due to ethnic or genetic differences. However, this cannot be elucidated further in this study.
Our study also demonstrated that the remaining life expectancy was much shorter in American or European countries compared to Asian countries. Compared to the Japanese study, Korean HD patients showed a similar survival profile [13]. This can be explained by ethnic or genetic differences. The previous studies performed in the United States and the United Kingdom also demonstrated that white HD patients showed inferior survival compared to non-whites [14,18–21]. In the general population, non-whites, especially African Americans show a poorer survival rate. However, in the dialysis population, paradoxical survival benefit was shown in African Americans compared to Caucasians. It may be due to the younger age to start dialysis in African Americans or higher body mass index or nutritional index in them [19].
Lastly, our study showed a shorter life expectancy in patients with diabetic nephropathy. This is in line with USRDS or ERA-EDTA (European Dialysis and Transplant Association) annual reports [14,15]. However, the differences in remaining life expectancy decreased as the patient’s age increased. This suggests that the cause of ESKD is less influential than the age factor.
Our study has some limitations. Firstly, we did not include HD patients younger than 30 years. They may have greater survival when included. Secondly, we could not compare the remaining life expectancy according to the cause of ESKD in the population with extreme age due to a small number of patients in those age groups. Thirdly, other variables such as smoking, alcohol intake, exercise, or dialysis vintage were not adjusted in the analysis of life expectancy. The variables such as smoking, alcohol intake, or exercise were not collected from the HD quality assessment. The dialysis vintage was not adjusted when calculating life expectancy because when we include the variable, the number of patients in each age group becomes too small for comparison. Since we only included prevalent HD patients and we know the mortality rate is the highest in the first 3 months of HD treatment [22,23], we may underestimate the actual mortality rate. In international comparison, data from other countries comprise both HD and peritoneal dialysis populations, but our data only includes the HD population. In addition, initial data collection includes outpatient HD data and excludes hospitalized or transferred cases. Data from Japanese, European, and American include both inpatient and outpatient data. Also, the data collection method and period were quite different by country. This may lead to selection bias since outpatients may represent a ‘healthier’ population compared to hospitalized patients. Therefore, better life expectancy in Korean HD patients can be the result of selecting a healthier total cohort. However, the Japanese study analyzed data from both inpatients and outpatients and still demonstrated better outcomes compared to Western countries. In addition, our follow-up survival data includes all possible data regardless of hospitalization. We assume that genetic or ethnic factors may weigh heavier than the selection bias. We could not validate our result using statistical methods except the lifetable method. Finally, we could not assess the improvement in survival rate among HD patients over the years. This should be further elucidated in the future study.
Despite many limitations, this is the first study to assess the remaining life expectancy in the prevalent HD patients in Korea. This study can help clinicians explain the prognosis to their HD patients. Longitudinal analysis should be warranted to analyze the effect of advanced dialysis technology on improved survival rates among the HD population.
Supplementary Materials
Supplementary data are available at Kidney Research and Clinical Practice online (https://doi.org/10.23876/j.krcp.23.241).
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Funding
This study was supported by a grant from the Korean Nephrology Research Foundation (Baxter 2023).
Data sharing statement
The data presented in this study are available upon reasonable request from the corresponding author.
Authors’ contributions
Conceptualization: HCP, DHK, YKL
Data curation: DHK, BYK, ML, GOK
Methodology: HCP, DHK, JK
Formal analysis: DHK, AJC, JK
Writing–original draft: HCP, AJC, YKL
Writing–review & editing: HCP, DHK, AJC, BYK, ML, GOK, JK, YKL
All authors read and approved the final manuscript.
Acknowledgements
The authors participated in the Joint Project on Quality Assessment Research, and HIRA collected and provided the claims data and quality assessment data to the authors. We used HIRA research data (M20220125786) for the current analysis.