



Introduction
Sarcopenia is characterized by the loss of muscle mass and strength, decreased physical performance, decreased quality of life (QoL), morbidities, and immobility with age, and it is associated with protein-energy wasting in chronic kidney disease (CKD) and end-stage kidney disease (ESKD) patients [1]. There have been several recommendations for sarcopenia criteria in Europe and Asia (Table 1) [2,3]. These recommendations use muscle strength, muscle quantity or quality, and physical performance to diagnose and classify sarcopenia.
Sarcopenia is primarily the age-related progressive loss of muscle mass and strength (muscle atrophy). Uremic sarcopenia means a progressive decrease in muscle mass, strength, and function despite normal skeletal muscle physiology in CKD patients. Uremic sarcopenia is not solely associated with the advanced age. It is mainly associated with the characteristics of uremia, such as metabolic acidosis, chronic inflammation, vitamin D deficiency, insulin resistance, hormonal changes, and gut dysbiosis, which contribute to the development of increased protein catabolism and reduced protein synthesis.
I will deal with the clinical significance, prevalence, risk factors, and strategies to prevent and treat sarcopenia with CKD in this review.
Clinical significance and prevalence of sarcopenia in chronic kidney disease
Sarcopenia is an important issue in dialysis-independent CKD and ESKD patients because it increases the risk of death, cardiovascular complications, the hospitalization rate, and disabilities. Sarcopenia is a strong predictor of mortality in dialysis-independent CKD and hemodialysis (HD) patients (hazard ratio [HR], 2.89; 95% confidence interval [CI], 1.40–5.96; p < 0.004 and HR, 6.99; 95% CI, 1.84–26.58; p = 0.004, respectively) [4,5]. Sarcopenia is a risk factor for cardiovascular events in HD patients (HR, 4.33; 95% CI, 1.51–12.43; p = 0.006) [5]. Sarcopenia is associated with a higher risk of hospitalization in HD patients (relative risk, 2.07; 95% CI, 1.48–2.88; p < 0.001) [6]. Sarcopenic patients exhibited a higher risk of falls than nonsarcopenic patients [7].
Physical inactivity due to sarcopenia results in poor prognosis in CKD patients. Several reports have shown a significant association of physical inactivity with kidney survival and mortality [8,9]. Therefore, maintaining physical performance to prevent sarcopenia is a critical factor in improving the prognosis of CKD patients. The prevalence and incidence of ESKD in Korea are increasing, with >100,000 and 18,642 patients at the end of 2019, respectively [10]. Therefore, the prevention and treatment of sarcopenia in CKD patients are highly important.
Altogether, sarcopenia is a major public health problem and will be even more important in the future given the aging society. The prevalence of sarcopenia in Korean older adults (mean age of 70.3 years) was 32.5% (total), 15.1% (male), and 42.1% (female) based on the Asian Working Group for Sarcopenia (AWGS) 2019 [11].
The prevalence of sarcopenia increases with CKD stage: 17% in stage 3a, 20% in stage 3b, 29% in stage 4, and 38% in stage 5 [12]. A lower lean mass and appendicular skeletal muscle mass index (ASMI) are correlated with glomerular filtration rate (GFR) decline, and a 1 mL/min/1.73 m2 decrease in GFR was associated with a 0.03 ± 0.01 kg/m2 decrease in the ASMI [13].
The prevalence of sarcopenia ranges from 4% to 42% according to the definition used, the population studied, and the stage of CKD [4,13–17]. A sarcopenia prevalence of 5.9% to 14% was found in dialysis-independent CKD patients [4,13], and that of peritoneal dialysis (PD) patients was from 4% to 15.5% based on the European Working Group for Sarcopenia criteria [15,16]. It was from 1.9% to 40% based on AWGS cutoffs in PD and HD patients [14,17].
The issue is the application of these criteria in clinical practice and the lack of recommended cutoff points in specific populations, such as CKD and ESKD patients. CKD is a condition associated with muscle loss [1,18–20]. There is a possibility of underestimating the clinical significance of sarcopenia in CKD patients [21].
Risk factors of uremic sarcopenia
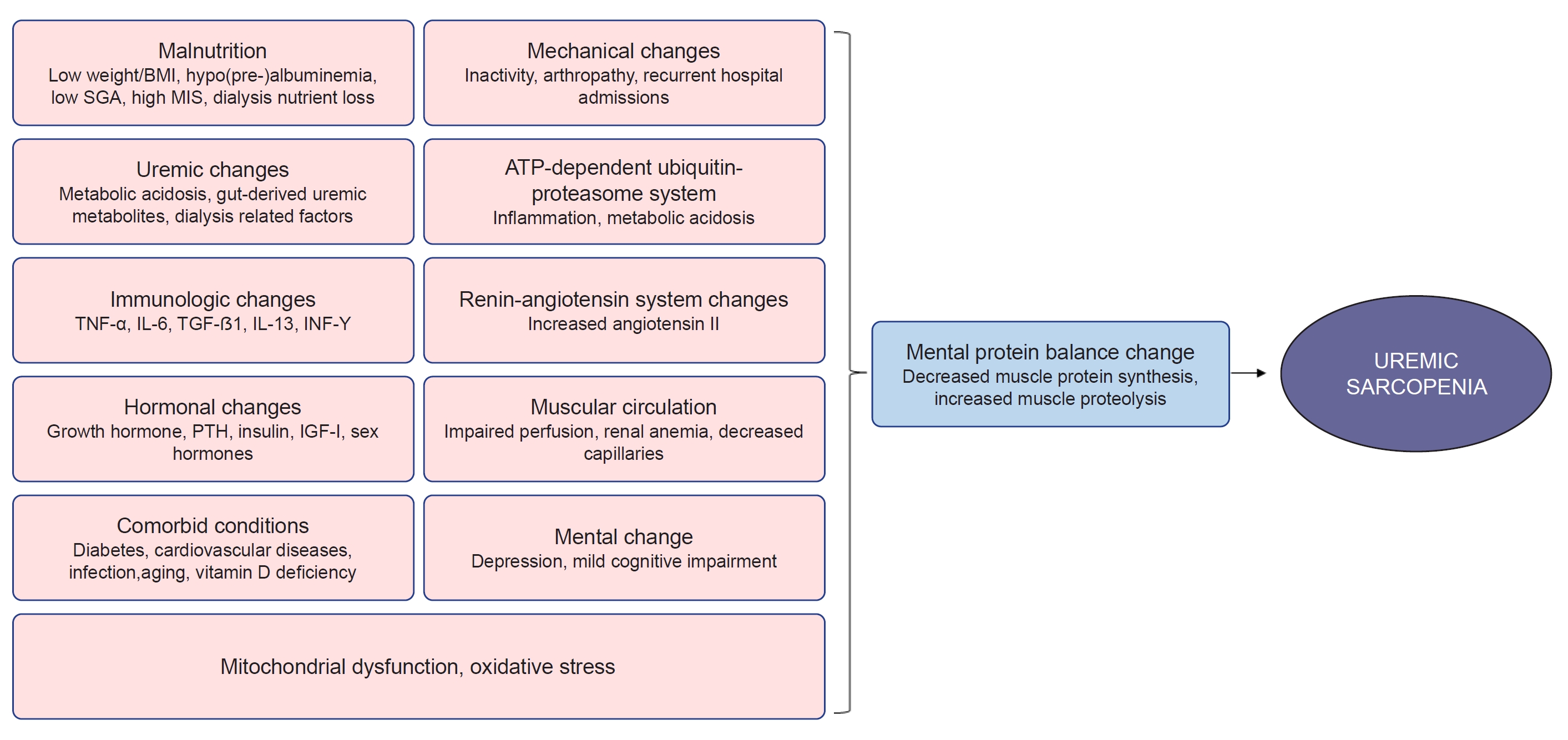
Several risk factors for sarcopenia are alleged in CKD and ESKD patients (Fig. 1).
Aging is associated with sarcopenia and an increased prevalence of CKD, which accelerates normal physiological muscle wasting [22]. CKD is associated with chronic low-grade inflammation leading to progressive weight loss, muscle weakness, and disabilities. Inflammatory cytokines, oxidative stress, and inactivity-mediated destruction of protein homeostasis result in the catabolic destruction of structural and functional proteins, resulting in skeletal muscle wasting and a decrease in exercise capacity [23,24].
Inflammation status, i.e., a high malnutrition-inflammation score (MIS) and high levels of high-sensitive C-reactive protein (CRP), interleukin (IL) 6, β2-microglobulin, and IL-4 is associated with sarcopenia in CKD patients [5,14,25–28].
Older age, male sex, low body mass index (BMI), and longer vintage of dialysis are associated with sarcopenia [12,17,29,30]. Malnutrition, i.e., low albumin/prealbumin levels, a high MIS, and poor nutritional status based on subjective global assessment are also associated with sarcopenia [5,14,17,25,27,31,32]. Low serum vitamin D levels and diabetes mellitus are risk factors for sarcopenia [5,12,17,32]. Depression (odds ratio [OR], 6.87; 95% CI, 2.06–22.96; p = 0.002) and mild cognitive impairment (OR, 6.36; 95% CI, 1.62–34.96; p = 0.008) are associated with sarcopenia [25,27].
Impaired perfusion due to chronic heart failure, decreased oxygen supply to skeletal muscles due to anemia, and decreased skeletal muscle capillaries are other risk factors for sarcopenia [33]. Insulin resistance-associated skeletal muscle atrophy and changes in muscle composition, including fat accumulation, are risk factors for sarcopenia in CKD [33,34]. Inactivity and renin-angiotensin system activation are also mechanisms of exercise intolerance in CKD [33].
Mitochondrial dysfunction of skeletal muscle in CKD is considered to be a cause of loss of muscle mass and exercise capacity [35–38]. CKD patients have decreased muscle mitochondrial content and oxidative capacity along with suppressed activity of various mitochondrial enzymes, leading to impaired energy production. These changes can be found from the early stages of CKD and are aggravated along with CKD progression [37].
Metabolic acidosis can induce glucocorticoid secretion and insulin resistance and increase branched-chain amino acid oxidation in skeletal muscles, which is associated with decreased muscle protein synthesis [39–41]. Acidosis also induces reprogramming of cellular metabolism to mitigate oxidative stress, although this originates from cancer cells [42].
Gut microbiome and uremic metabolite
Influx of urea and other retained toxins exerts a change in the gut microbiome in CKD, favoring pathobiont overgrowth. The abundance of bacteria that contain tryptophanase and urease and produce uremic toxins such as indoxyl sulfate (IS), p-cresyl sulfate (PCS), and trimethylamine-N-oxide (TMAO), increases, while the abundance of beneficial bacteria producing short-chain fatty acids, an essential nutrient for the colonic epithelium, decreases [43]. Lactobacillus and Bifidobacterium are decreased, while Proteobacteria, Enterobacter, Escherichia coli, Acinetobacter, Clostridium perfringens, and Proteus species are increased in the colon of CKD patients [44].
Disruption of the colonic epithelial tight junction associated with urea influx, increased ammonium production, and decreased epithelial survival results in the loss of integrity and increased intestinal permeability, which allows the translocation of bacteria and lipopolysaccharide (LPS). LPS can activate immune cells through the toll-like receptor 4 (TLR-4) dependent and nuclear factor kappa-B (NF-κB) pathway. And pathobionts can stimulate dendritic cells and produce inflammatory cytokines [45]. Prolonged colonic transit time, dietary restriction of fiber, and metabolic acidosis also directly and indirectly contribute to dysbiosis and the altered intestinal environment [46].
Role of the gut microbiome and uremic metabolite on the maintenance of skeletal muscle mass
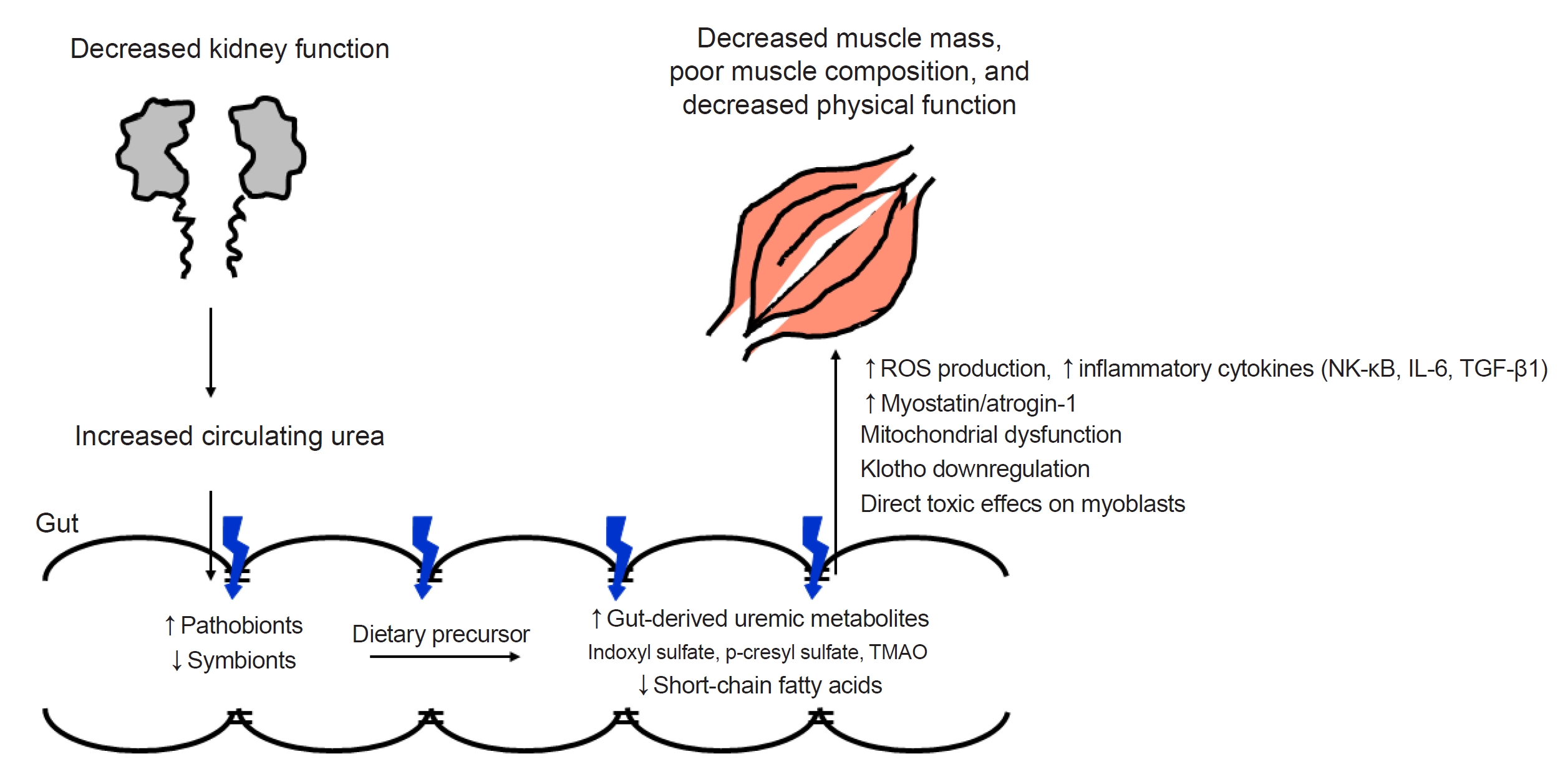
Reduced muscle mass, altered muscle composition, i.e., increased deposition of lipids or adipocytes within and/or between muscles, and poor physical function are prevalent in ESKD patients. ESKD patients have elevated uremic metabolite levels combined with an altered gut microbiome, increased gut-derived uremic metabolites, and increased epithelial permeability. In turn, the fecal levels of short-chain fatty acids are reduced. The accumulation of gut-derived uremic metabolites within skeletal muscle results in decreased muscle mass or increased lipid content [47]. Increased urea due to decreased kidney function, gut dysbiosis, increased circulating uremic metabolites, and the resultant reduced muscle mass, altered muscle composition, and poor physical function is called the kidney-gut-muscle axis (Fig. 2).
Protein-derived tryptophan is metabolized into indole, which is then absorbed into the bloodstream and oxidized into IS in the liver [48]. Uremic toxins enter target cells via specific transporters, such as the organic anion transporter (OAT), and then, exert their toxicity via the activation of cellular nicotinamide adenine dinucleotide phosphate hydrogen (NADPH) oxidase, which results in the overproduction of reactive oxygen species (ROS) and inflammatory cytokines [49,50]. IS also enters various cells via OATs (OAT1 and OAT3), and OATs are expressed in muscles [51–53].
IS and PCS accumulate in various organs, including skeletal muscle, in the CKD mouse model [54]. IS exposure inhibited cell proliferation and cell viability and decreased mitochondrial function in mouse muscle cells. CKD patients also showed a significant inverse association between plasma IS levels and skeletal muscle mass [55]. High IS levels were associated with longer HD vintage, and IS was negatively correlated with the skeletal muscle mass index in HD patients. HD patients with high IS levels showed greater loss of hand grip strength (HGS) [56].
Accumulated IS in muscle cells via OAT activates NADPH oxidase and the aryl hydrocarbon receptor (AHR) pathway to cause increased ROS production. Enhanced ROS trigger inflammatory cytokines, such as tumor necrosis factor alpha (TNF-α), IL-6, and transforming growth factor beta 1 (TGF-β1), and induce myostatin (negative regulator of muscle growth) and atrogin-1 (muscle-specific ubiquitin ligase family) expression, which are involved in muscle wasting [52].
IS also induces mitochondrial network disintegration through metabolic alterations, such as an increase in antioxidative responses (pentose phosphate pathway and glutathione metabolism), and a decrease in energy generation-related pathways (tricarboxylic acid cycle, glutamine metabolism, and mitochondrial oxidative phosphorylation) in muscle cells, which results in reduced adenosine triphosphate (ATP) production [55]. Muscle mitochondrial dysfunction was found from the early stage of CKD and muscle atrophy followed by exercise impairment [37]. Muscular mitochondria were decreased in the early stage of CKD in mice.
In addition, IS downregulated Klotho expression through ROS-associated NF-κB activation [57]. Klotho levels and skeletal muscle physiology are closely related [58,59]. Klotho-deficient mice showed significantly decreased body weight and forelimb grip strength, and Klotho overexpression restored grip strength and running capacity [60]. It is possible that downregulation of Klotho by IS in muscles is one of the mechanisms of sarcopenia in CKD. IS also has direct toxic effects on myoblasts by decreasing their viability and increasing cell apoptosis [61].
Strategies to prevent and treat sarcopenia
Researchers can acquire an impression regarding the treatment strategies based on all of the risk factors mentioned above. Many drugs have been developed to prevent or treat sarcopenia. However, there are no drugs approved by the U.S. Food and Drug Administration for the treatment of sarcopenia [64]. Only a few of them, i.e., Bimagrumab from Novartis and Sarconeos from Biophytis SAS, have recently shown favorable results.
Bimagrumab (BYM338) is a fully human monoclonal antibody, which was developed to treat pathological muscle loss and weakness. It binds to and inhibits activin receptor type-2B and prevents the actions of natural ligands that negatively regulate skeletal muscle growth [65,66]. Activin receptor type-2B blockade with Bimagrumab resulted in the significant loss of fat mass, gain in lean mass, and metabolic improvements during 48 weeks in patients with overweight or obesity who had type 2 diabetes in a phase 2 trial [66].
20‐Hydroxyecdysone (20E) is a polyhydroxylated plant steroid that has pharmacological effects in aging and sarcopenia. Sarconeos (BIO101) is a 20E purified investigational drug (≥97%). It targets proto-oncogene protein-c-MAS-1, MAS receptor. BIO101 showed a good safety and pharmacokinetic profile in a phase 1 study for healthy young and older adults [67]. In a phase 2 study (NCT03452488), BIO101 was orally administered for 26 weeks to community-dwelling men and women aged ≥65 years, suffering from age-related sarcopenia (including sarcopenic obesity), and at risk of mobility disability. It was a double-blind, placebo-controlled clinical trial. BIO101 at the highest dose (350 mg, twice daily) showed a clinically meaningful improvement in the 400-m walk test [68].
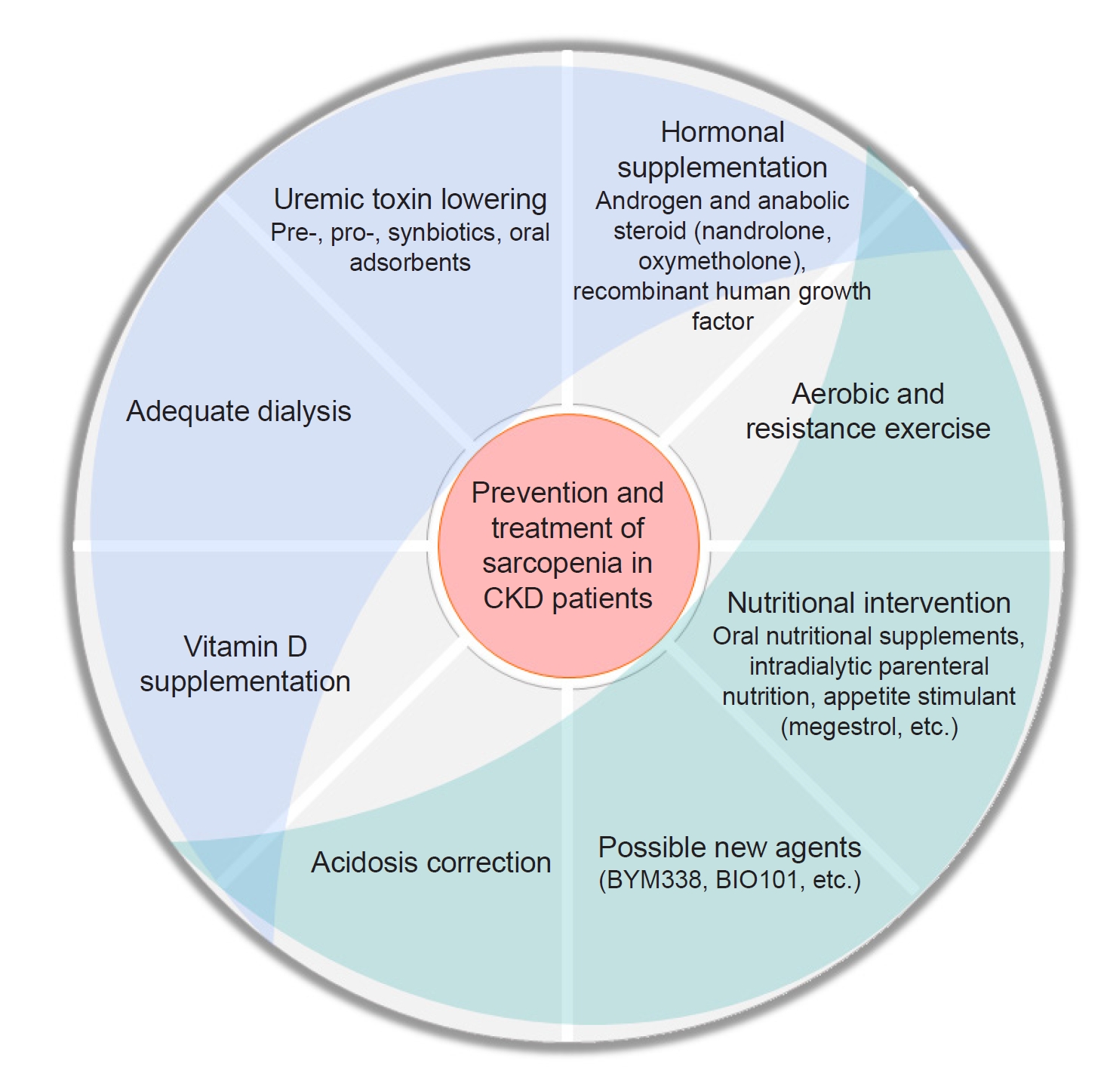
The main interventions for sarcopenia in CKD patients are aerobic and resistance exercises along with nutritional interventions. Furthermore, optimizing dialysis, vitamin D status, acidosis, and the management of comorbidities such as depression are mandatory [69].
Megestrol acetate
HD patients with no residual kidney function (age of 40–80 years) treated with a daily dose of 160 mg of megestrol acetate for 2 to 12 months, experienced an increase in weight (2–9 kg) associated with an increase in the protein catabolic rate, albumin concentration, serum creatinine and urea [70]. In addition, megestrol improved body water distribution with an increase in the intracellular water component and muscle mass.
A review of small retrospective studies showed an increase in BMI, albumin levels, and protein-energy intake after megestrol acetate [71]. A systematic review, especially of dialysis patients, showed a significant increase in body weight, albumin levels, and appetite, although they were small studies (n = 9–32) with a short duration (8–24 weeks) and a high degree of bias. Megestrol acetate was also associated with overhydration, excessive fluid gain, diarrhea, hyperglycemia, suppressed cortisol levels, thrombophlebitis, nausea, and vomiting [72].
Hormonal therapies
Nandrolone (decanoate), an androgen and anabolic steroid medication, which is used in the treatment of wasting syndrome and is given through intramuscular or subcutaneous way, injection in HD patients for 6 months significantly increased lean body mass, improved functional capacity (walking and stair-climbing test), and increased appendicular lean mass in a dose-responsive manner [73,74]. Nandrolone combined with intradialytic resistance training for 12 weeks increased the quadriceps muscle cross-sectional area in an additive manner [75].
Oxymetholone, an oral androgen and anabolic steroid, which is also used in the treatment of wasting syndrome and promotion of weight gain and muscle growth, has a higher anabolic effect and lower androgenic activity than testosterone. HD patients showed an increase in fat-free mass, HGS, and physical functioning scores as well as an increase in mRNA expression for myosin heavy chain, and insulin-like growth factor (IGF)-I/II in muscles after oxymetholone administration for 24 weeks [76].
Recombinant human growth hormone (rhGH) increased protein synthesis and decreased protein catabolism in HD and PD patients [77–80]. rhGH increased lean body mass and improved QoL [81]. rhGH also increased HGS after 6 months in elderly HD patients [82]. However, another large randomized controlled trial (RCT) study (OPPORTUNITY) failed to show an increase in albumin levels, lean body mass, physical capacity, or QoL [83]. rhGH also showed adverse effects, including soft tissue edema, arthralgia, carpal tunnel syndrome, gynecomastia, and dysglycemia [83].
Vitamin D
CKD patients in stages 3 to 4 and PD patients with vitamin D deficiency became vitamin D sufficient after vitamin D replacement. They showed improvements in physical function (timed up and go, gait speed, timed chair stand, stair climb, static and dynamic balance) and isometric strength [84]. Vitamin D supplementation in male HD patients also improved muscle mass [85].
However, supplementation of cholecalciferol 50,000 units/week with the target of 25(OH)D concentration >80 nmol/L in HD patients with an initial 25(OH)D concentration <50 nmol/L had no effect on muscle strength or symptoms [86]. Treatment with 50,000 units of oral cholecalciferol supplementation, once weekly for 8 weeks and then monthly for 4 months, to HD patients with a 25(OH)D concentration <60 nmol/L showed higher 25(OH)D and 1,25(OH)2D levels without increased calcium or phosphorus levels. However, muscle strength, functional capacity, and QoL did not change [87].
Correction of acidosis
Advanced CKD patients (eGFR of 15–30 mL/min/1.73 m2) with metabolic acidosis presented an increase in the mid-arm circumference, protein intake, and serum albumin levels after oral sodium bicarbonate administration for 2 years [88]. An RCT of PD patients showed an increased body weight and mid-arm circumference and decreased hospitalization after 1 year of high alkali dialysate [89]. In addition, a high bicarbonate dialysate concentration of 40 mmol/L resulted in better control of acidosis and increased triceps skin fold thickness compared to a bicarbonate concentration of 30 mmol/L [90].
Biotics
Because gut dysbiosis is associated with systemic inflammation, the administration of biotics can be an indirect target to ameliorate muscle wasting. Lactobacillus species and Bifidobacterium ameliorated muscle wasting in mouse models, and Lactobacillus exhibited the potential to restore microbiome balance, and the gut permeability, which was associated with the improvement in muscle mass or strength, was reduced [91]. However, probiotics containing Lactobacillus and Bifidobacterium did not show meaningful effects on muscle mass and function in humans, because of the scarcity of studies, the variability in the populations, and the difficulty in accurately and reproducibly measuring muscle mass and function [92].
Nonetheless, Bifidobacterium longum was significantly increased after prebiotic administration in super-elderly patients with sarcopenia. The skeletal muscle mass index was increased, while the body fat percentage was decreased [93]. A randomized, double-blind, placebo-controlled, crossover trial using synbiotics over 6 weeks in predialysis CKD patients showed an increase in Bifidobacterium and Lactobacillus after synbiotic therapy as well as a decrease in Clostridiales. The Bifidobacterium change showed an inverse correlation with the concentration of serum IS and PCS [94].
Although there is no data about the effect of biotics on muscle mass, muscle strength, or physical function, there are several reports about the relationship between biotics and surrogate outcomes such as inflammation, oxidative stress, uremic toxins, and endotoxins.
Probiotic supplementation in HD patients reduced systemic inflammatory responses, which was associated with an increase in Tregs and a decrease in proinflammatory monocytes [95]. Probiotic, prebiotic, and synbiotic administration also reduced CRP, IL-6, and IS levels, and increased high-density lipoprotein cholesterol in dialysis patients [96]. Synbiotics were more effective than probiotics in improving inflammatory markers, endotoxins, and anti-heat shock protein70 serum levels in HD patients [97]. Synbiotics also reduced serum IS, PCS, and urea in HD patients [98].
Oral adsorbents
AST-120 adsorbs uremic toxins and precursors, including indole, and excretes them into the feces.
AST-120 administration increased Lactobacillus in CKD rats. The microbiota composition after AST-120 treatment was between that of normal and CKD rats [99]. CKD rats showed elevated plasma endotoxin, IL-6, TNF-α, monocyte chemoattractant protein-1 (MCP-1), cytokine-induced neutrophil chemoattractant-3 (CINC-3), L-selectin, intercellular adhesion molecule-1 (ICAM-1), and malondialdehyde levels and depletion of the colonic epithelial tight junction proteins, claudin-1, occludin, and zonular occludens-1 (ZO-1). AST-120 showed partial restoration of epithelial tight junction proteins and a reduction in plasma endotoxin and markers of oxidative stress and inflammation [100].
AST-120 prevented the tissue accumulation of IS and PCS in skeletal muscle, which resulted in the amelioration of muscle atrophy (cross-sectional area) [54]. AST-120 prevented CKD-induced physical inactivity mainly by maintaining mitochondrial function, suppressing atrogin-1/myostatin expression, and recovering Akt phosphorylation in skeletal muscle [101]. A reduction in oxidative stress via AST-120 improved exercise capacity and mitochondrial biogenesis of skeletal muscle [33,101]. AST-120 significantly restored skeletal muscle weight in CKD mice. In addition, AST-120 increased the renal expression of Klotho, which was decreased under uremic conditions [102]. Klotho levels and skeletal muscle physiology were closely related, as we mentioned above [58,59].
In a human RCT, gait speed significantly increased over 1 year after carbonaceous oral adsorbent administration. Bodily pain, vitality, symptoms/problems, and cognitive function also improved in the oral adsorbent group, while the quality of social interactions and kidney disease effects decreased in the control group [103]. Prospective studies with longer follow-up durations, larger sample sizes, and interventions to lower uremic toxins are necessary to elucidate the role of uremic toxins in CKD patients with sarcopenia.
The effectiveness of pharmacologic interventions mentioned above is summarized in Table 2.
In conclusion, aerobic and resistance exercise, along with nutritional interventions, including oral and intradialytic parenteral nutritional supplements, has been the main preventive or treatment strategies for sarcopenia in dialysis-independent CKD and ESKD patients. In addition, anabolic hormones, including anabolic steroids and growth hormones, and appetite stimulants showed beneficial effects on biochemical markers such as serum albumin level, both muscle strength and mass, and physical function. Correction of metabolic acidosis and vitamin D status also showed favorable effects on physical function, muscle mass, and strength. Biotics improved the gut microbiome composition and the level of uremic toxins, endotoxins, inflammation, and oxidative stress. Oral adsorbents also showed beneficial effects on the restoration of the gut microbiome composition and intestinal wall integrity as well as on the skeletal muscle physiology. A multifaceted approach can be helpful to lessen the burden of sarcopenia in CKD patients (Fig. 3).
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









