


Introduction
Idiopathic membranous nephropathy (iMN) is a common cause of nephrotic syndrome in adults and the major cause of end-stage renal disease (ESRD) [1–3]. Deposition of immunoglobin G and other immune complexes on the subepithelial layer of the glomerular capillary wall is associated with the pathogenesis of iMN [4]. Typically, one-third of patients with iMN will progress to ESRD and the remaining two-thirds will maintain stable renal function or achieve spontaneous remission of proteinuria [5,6]. Considering the clinical course and natural history of iMN, and because the risks associated with the use of immunosuppressive agents should not outweigh the short-term risks of nephrotic syndrome, delaying the use of immunosuppressants may be acceptable for up to 3 years in patients with minimal symptoms and preserved renal function [7]. The Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference recommended treatment with immunosuppressive agents only for high-risk patients after risk stratification [8].
Treatment goals for patients with iMN include improving quality of life and reducing adverse events associated with therapy, such as infections and cardiovascular or thromboembolic events, as well as clinical outcomes such as remission of proteinuria and preservation of renal function [9,10]. Although various immunosuppressive agents have been shown to produce more favorable outcomes with respect to remission of proteinuria compared with conservative treatment [11–13], other studies of different types of immunosuppressants reported conflicting results in terms of renal survival or mortality [14,15].
Therapeutic regimens for iMN, and cytotoxic agents in particular, can induce various adverse effects, such as infections, malignancies in the bladder, lung cancer, leukopenia, and infertility. Although calcineurin inhibitors (CNIs) such as cyclosporine (CsA) or tacrolimus (TAC) are promising alternatives to cyclophosphamide (CYP) in some circumstances as they can induce remission at frequencies similar to those of CYP [16,17], their usefulness in patients with impaired kidney function is limited, and the consequences of long-term therapy are uncertain. Randomized controlled trials with mycophenolate mofetil (MMF) and corticosteroids for steroid-sparing or avoidance of CNI nephrotoxicity have demonstrated comparable, or at least non-inferior, effects on remission rates in patients with iMN [18,19].
The discovery of the anti-phospholipase A2 receptor (anti-PLA2R) resulted in a paradigm shift in treatment strategies [20]. Rituximab (RTX), which targets anti-CD20 monoclonal antibodies, can achieve remission of proteinuria in approximately two-thirds of patients with iMN [21,22]. Because of significantly fewer adverse events, RTX is suggested as a first-line immunosuppressant therapy for patients with iMN [23]. Recently published randomized controlled trials found that pronounced remission was obtained with RTX [24].
Recently, we described the clinical features and outcomes of iMN from a multi-center cohort study [25]. One of the limitations of that study was a lack of data on medications, such as immunosuppressants, that could provide a basis for predicting prognoses and establishing optimal management in patients with iMN. The use of immunosuppressants is an important factor influencing clinical outcomes. However, few comparative studies have been conducted on the long-term effects of immunosuppressive agents in large-scale cohorts of patients with iMN. We therefore evaluated the effect of immunosuppressants on clinical outcomes from a cohort of patients with iMN.
Methods
Study population and treatment protocol
We reviewed the records of 2,027 patients diagnosed with iMN between 1979 and 2018 in the Korean GlomeruloNEphritis sTudy (KoGNET), which examined a cohort of patients with renal biopsy at multiple centers in Korea. Patients younger than 15 years of age and those with grafts or repeated biopsy were excluded. Of the 2,027 iMN patients, drug use history, follow-up laboratory results, and outcomes were obtained from the records of 520 patients from four university-based hospitals: Seoul National University Hospital, Seoul National University Bundang Hospital, Kyungpook National University Hospital, and Kyungpook National University Chilgok Hospital. Thirty-one patients with an inaccurate drug history or who were lost to follow up were excluded. Finally, data on 489 iMN patients between 2001 and 2020 were included in the analysis. This study was approved by the Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital (No. KNUCH 2017-09-001). As this study is retrospective and the study subjects have been deidentified, the IRB waived the need for written consent from patients.
Patients with iMN patients were divided into those receiving conservative treatment and those receiving immunosuppressants. Conservative treatment consisted of blood pressure control and reduction of proteinuria with an angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB). For treatment of hypercholesterolemia, statins were added. Immunosuppressants (oral CsA, TAC, MMF, oral or intravenous CYP, and intravenous RTX) combined with steroids were used if the attending physician determined they were needed.
Data collection and outcomes
Demographic and laboratory data were acquired at the time of iMN diagnosis and follow-up. Clinical characteristics, including age, sex, body mass index, and comorbid conditions (e.g., hypertension, diabetes, coronary heart disease, or cerebrovascular disease), were investigated. Laboratory data were collected on levels of hemoglobin (Hb), total protein, albumin, blood urea nitrogen, serum creatinine, total cholesterol, low-density lipoprotein cholesterol, uric acid, and spot urine protein-to-creatinine ratio (PCR). The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation. The time of remission and urine PCR data at that time were also acquired for the follow-up period.
Primary outcomes were complete or partial remission (CR or PR) of proteinuria. CR was defined as a decrease in proteinuria to ≤300 mg/day. PR was defined as a decrease in proteinuria to <3,500 but >300 mg/day and a decrease of >50% compared with baseline. Secondary outcomes were ESRD, death, and infection. ESRD was defined as a need for renal replacement therapy, such as maintenance of dialysis or kidney transplantation. Maintenance renal replacement therapies and deaths between the time of iMN diagnosis and the last follow-up were recorded. An infectious event was defined as a viral or bacterial infection requiring treatment with antiviral agents or antibiotics.
Anti-PLA2R antibody (Ab) levels in patients were measured with an enzyme-linked immunosorbent assay during outpatient follow-up after 2018. Anti-PLA2R Ab was defined as positive if levels reached ≥20 RU/mL at least once during the follow-up.
Statistical analysis
The Student t tests were applied to continuous variables and the chi-square tests to categorical variables as appropriate. All data were summarized as mean ± standard deviation or as percentages. Demographics and outcomes were analyzed for each patient according to immunosuppressant use. Given the differences in baseline characteristics between the conservative and immunosuppressant treatment groups, propensity score matching was performed. The propensity score, the conditional probability of receiving conservative versus immunosuppressant treatment, was estimated by applying a multivariable logistic regression model to age, sex, and spot urine PCR, eGFR, serum albumin, cholesterol, and Hb levels. Matching was performed using a 1:1 protocol without replacement (greedy-matching algorithm), with a caliper width equal to 0.2 standard deviations of the logit of the propensity score. Standardized differences were estimated for all baseline covariates to assess the balance between the two groups. A difference of <0.1 for a given covariate indicated a relatively small imbalance. Subgroup analyses were performed to assess the effects of immunosuppressant treatment across strata of age (<65 years vs. ≥65 years), sex (male vs. female), spot urine PCR (<4.0 g/g vs. ≥4.0 g/g), and eGFR (<60 mL/min/1.73 m2 vs. ≥60 mL/min/1.73 m2) in a Cox proportional hazards model. The cumulative incidence of CR or PR and survival was estimated using the Kaplan-Meier method. Loss of follow-up, death, initiation of dialysis, or kidney transplantation were considered censoring. Statistical analyses were performed in R version 4.0.3 (R Foundation for Statistical Computing; www.r-project.org). A p-value of <0.05 was assumed to indicate significance.
Results
Characteristics of patients
The characteristics of the 489 patients with iMN at the time of iMN diagnosis are presented in Table 1. The mean patient age was 56.2 ± 13.5 years and 266 (54.4%) were male. One hundred ninety-six patients (40.1%) had hypertension and 64 (13.1%) had diabetes. Mean serum creatinine was 1.0 ± 0.6 mg/dL; eGFR, 87.8 ± 26.4 mL/min/1.73 m2; serum albumin, 2.7 ± 0.7 g/dL; and total cholesterol, 275.3 ± 100.7 mg/dL. Mean urine PCR was 5.8 ± 4.7 g/g, and 261 patients (53.4%) had nephrotic-range proteinuria (≥3.5 g/g).
Of the 489 patients, 357 (73.0%) received immunosuppressants. These patients were significantly older and comorbidity, such as hypertension and cerebrovascular disease, was prevalent, compared with patients receiving conservative treatment. Patients in the immunosuppressant treatment group had a significantly lower mean albumin level (2.6 ± 0.6 g/dL vs. 3.3 ± 0.8 g/dL), higher total cholesterol (287.9 ± 101.2 mg/dL vs. 234.0 ± 90.8 mg/dL), heavier proteinuria (6.5 ± 4.7 g/g vs. 3.8 ± 4.3 g/g), and higher proportion of nephrotic-range proteinuria (60.5% vs. 34.1%) compared with the conservative treatment group. However, we found no significant differences in sex, age, body mass index, comorbid conditions (e.g., diabetes, coronary heart disease, cerebrovascular disease, serum creatinine, and eGFR) between the conservative and immunosuppressant treatment groups. An ACEi or ARB was used in 447 (91.4%) of 489 patients in the immunosuppressant group, and the proportion of patients receiving an ACEi or ARB did not differ significantly between the two groups.
Using propensity score matching, 82 patients who received immunosuppressive agents were matched with 82 patients who received conservative treatment. After propensity score matching, the standardized differences were <0.1 for covariates of age, sex, urine PCR, eGFR, serum albumin, cholesterol, and Hb levels, indicating only small differences between the two groups.
Of the 357 patients who used immunosuppressants, 152 used CYP as the first-line immunosuppressive agent, followed by CsA in 122 patients, whereas TAC was chosen for 23 patients and MMF for 20 (data not shown). The mean time from diagnosis of iMN to initiation of immunosuppressive agents was 8.8 ± 24.4 months (in subjects who had urine PCR < 3.5 g/g) vs. 4.0 ± 11.0 months (urine PCR ≥ 3.5 g/g) in the total population and 12.4 ± 32.0 months (urine PCR < 3.5 g/g) vs. 2.1 ± 4.1 months (urine PCR ≥ 3.5 g/g) in the propensity score-matched population, respectively.
Clinical characteristics based on immunosuppressant type are presented in Supplementary Table 1 (available online). Age, cerebrovascular disease, and eGFR were significantly different among immunosuppressant subgroups. Sex, body mass index, comorbidity (hypertension, diabetes, coronary heart disease), serum albumin, total cholesterol level, and urine PCR levels did not differ among patients receiving each type of immunosuppressant. Of the 495 cases treated with immunosuppressants, CYP was most commonly used (n = 182), followed by CsA (n = 158).
Primary outcomes
Over a median follow-up of 89.0 months (first to third quartile, 56.5–131.5 months), 428 patients (87.5%) achieved remission (CR or PR). In the immunosuppressant group, 320 patients (89.6%) reached a CR or PR, compared with 108 patients (81.8%) in the conservative treatment group during follow-up. The proportion of patients who achieved a CR or PR during the follow-up period was significantly higher in the immunosuppressant treatment group in the total population (p = 0.003) (Table 2). In addition, the time to reach a CR or PR was significantly longer in the conservative treatment group than it was in the immunosuppressant group (25.6 ± 31.8 months vs. 17.3 ± 21.9 months, p = 0.001). However, the proportion of patients who achieved a CR or PR during the follow-up period and the time to reach a CR or PR did not differ significantly between the two groups in the propensity score-matched population (p = 0.29 and p = 0.53, respectively).
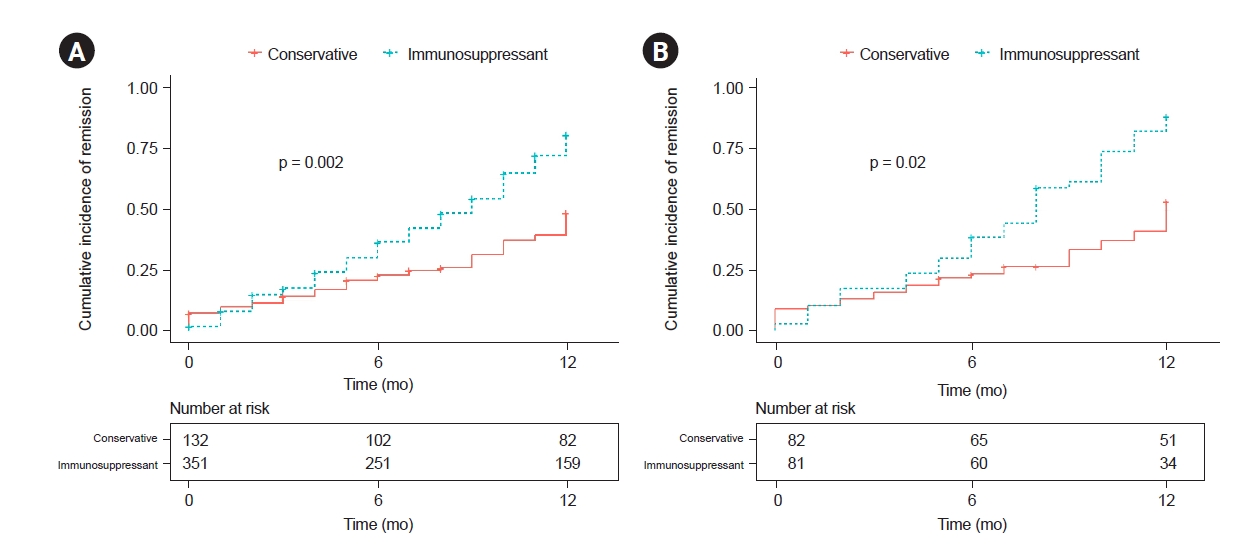
In the total population, 192 patients (53.8%) in the immunosuppressant treatment group achieved a CR or PR at 12 months, compared with 50 patients (37.9%) in the conservative treatment group. The cumulative incidence of CRs or PRs was significantly higher in the immunosuppressant group compared with the conservative treatment group at 12 months in both the total population (p = 0.002) (Fig. 1A) and the propensity score-matched population (p = 0.02) (Fig. 1B).
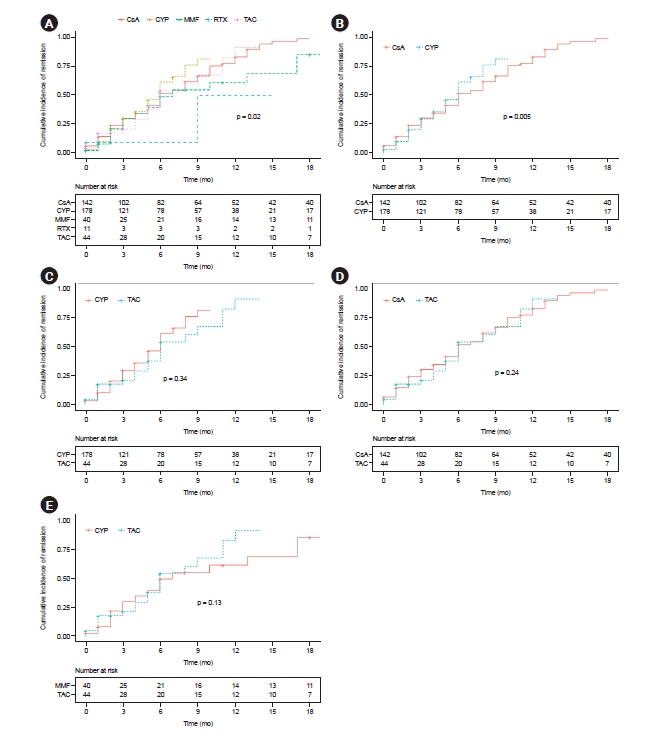
The cumulative incidence of achieving a CR or PR differed significantly by type of immunosuppressant (p = 0.02) (Fig. 2A). In addition, the time to reach remission from treatment was also significantly different among the five immunosuppressants (p = 0.02) (Table 3). Cumulative incidence of a CR or PR was significantly higher in patients treated with CYP than in those treated with CsA (p = 0.005) (Fig. 2B), but it was comparable with respect to CYP vs. TAC, CsA vs. TAC, and TAC vs. MMF (Fig. 2C–E).
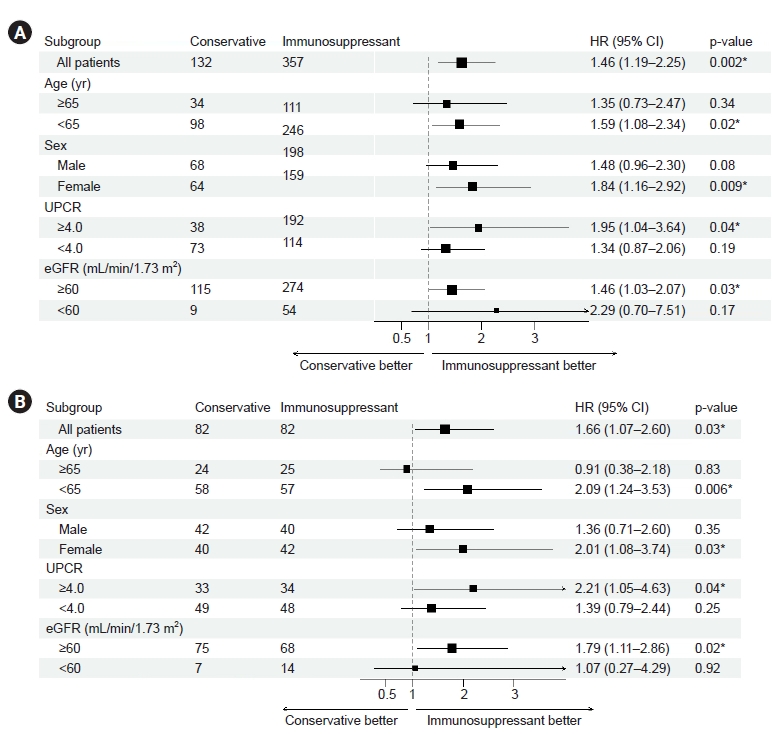
In subgroup analyses of the total population, the use of immunosuppressants significantly improved the likelihood of achieving a CR or PR at 12 months in the group of patients who were under 65 years of age (hazard ratio [HR], 1.59; 95% confidence interval [CI], 1.08–2.34; p = 0.02), female sex (HR, 1.84; 95% CI, 1.16–2.92; p = 0.009), spot urine PCR of ≥4.0 g/g (HR, 1.95; 95% CI, 1.04–3.64; p = 0.04), and eGFR of ≥60 mL/min/1.73 m2 (HR, 1.46; 95% CI, 1.03–2.07; p = 0.03) (Fig. 3A). These results were maintained in the propensity score-matched patients (Fig. 3B).
Secondary outcomes
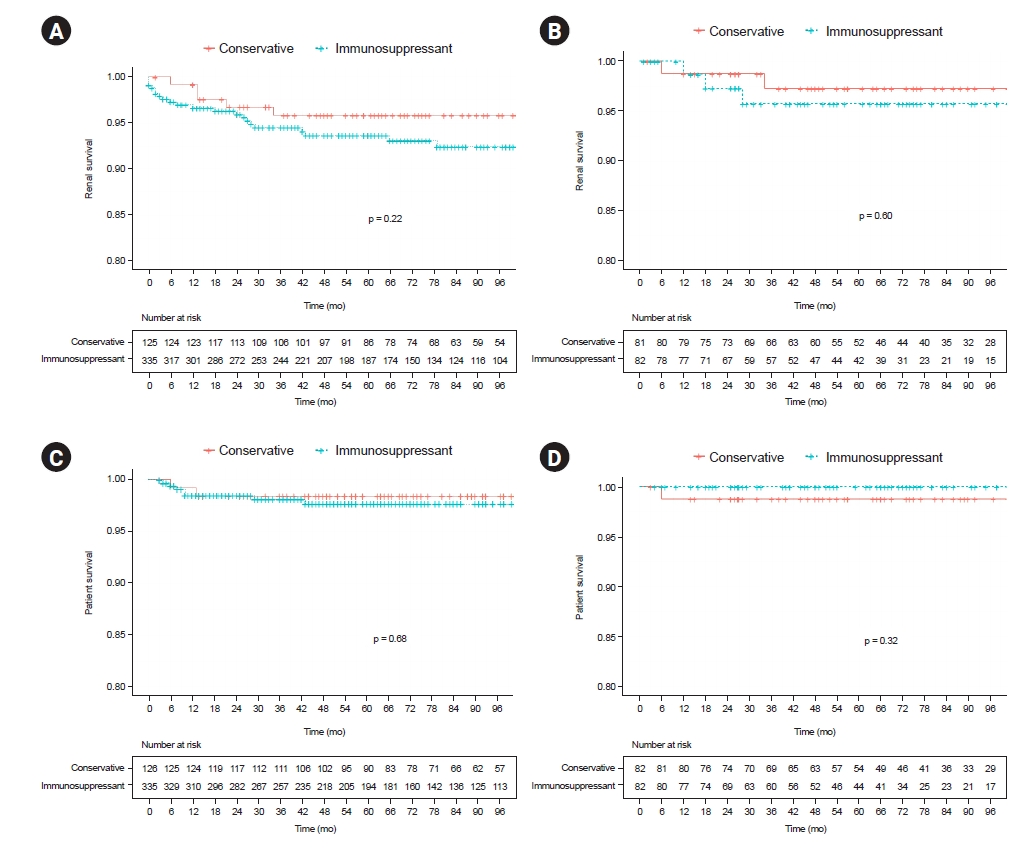
In the total population, five patients (3.8%) in the conservative treatment group and 22 (6.2%) in the immunosuppressant group progressed to ESRD (p = 0.30) (Table 2). Renal survival was similar between the two treatment groups in the Kaplan-Meier analysis (p = 0.22) (Fig. 4A). Similar results were found in the propensity score-matched population (p = 0.60) (Fig. 4B). However, the proportion of patients who progressed to ESRD differed among the five types of immunosuppressants (Table 3).
Two patients (1.5%) in the conservative treatment group and seven patients (2.0%) in the immunosuppressant group died over the follow-up. We found no significant difference in patient survival between the conservative and immunosuppressant treatment groups in the total population (p = 0.68) (Fig. 4C) or propensity score-matched population (p = 0.32) (Fig. 4D).
Infection was significantly more common in the immunosuppressant group (n = 78, 21.8%) than in the conservative treatment group (n = 18, 13.6%) in the total population (p = 0.03) (Table 2). However, it was comparable between the two groups in the propensity score-matched population (p > 0.99). Among the five types of immunosuppressants, patients treated with RTX (31.3%) had the highest rate of infection, followed by CYP (28.0%) and TAC (23.5%) (Table 3).
Anti-PLA2R Ab positivity differed significantly between the two groups in both the total population (p = 0.007) and propensity score-matched population (p = 0.04).
Discussion
This study reveals the effect of immunosuppressants on clinical outcomes in a cohort of iMN patients over 20 years. Remission of proteinuria was achieved in 87.5% of all patients receiving conservative or immunosuppressant treatment, which was a favorable long-term outcome, as was the case in other studies [14,15,26]. Spontaneous remission was attained by 37.9% of the conservative treatment group, compared with approximately 30% of affected patients reported in a previous study [27]. Here, the proportion of patients who achieved remission was significantly higher, and remission occurred sooner in the immunosuppressant group than in the conservative treatment group for the complete follow-up period in the total population. In addition, the cumulative incidence of remission was significantly higher in the immunosuppressant group than in the conservative treatment group at 12 months. Renal survival was similar between the two groups. The use of immunosuppressants may therefore have resulted in a favorable remission rate and stabilized kidney function in the total population, as have been previously reported [14,15,28]. However, the patients treated with immunosuppressants in this study had significantly lower albumin levels and heavier proteinuria. Given the differences in baseline characteristics between the two groups, propensity score matching to estimate the probability of receiving immunosuppressants was also performed for the analysis. In the propensity score-matched population, the cumulative incidence of remission was significantly higher in the immunosuppressant group compared with the conservative treatment group at 12 months in the total population, even though the characteristics of the patients who achieved remission were similar between the two groups. In addition, renal survival was comparable between the two groups in the total population.
Propensity score matching has been used previously to analyze outcomes between immunosuppressant and conservative treatments in iMN patients [29,30]. Although a previous study by Sato et al. [30] found no significant differences in long-term outcomes between the two groups after propensity score matching, Cattran et al. [29] reported a significant difference in renal survival. In addition, to determine the patient group in which immunosuppressants were the most useful, we performed a subgroup analysis. The analyses found that immunosuppressants were significantly more effective at inducing remission at 12 months in the group of patients who were under 65 years of age, or female, or had a urine protein level of ≥4.0 g/g, or had eGFR of ≥60 mL/min/1.73 m2 in the total and propensity score-matched populations, which is consistent with the KDIGO guidelines that suggest the use of immunosuppressants in patients with relatively good renal function and heavy proteinuria [8].
Debate persists about which immunosuppressants should be used in patients with iMN, although various regimens have been proposed for 30 years. In this study, the remission rate differed by immunosuppressant regimen. When comparing the differences among the types of immunosuppressants, differences may arise from the relatively superior remission rate in the CYP group of 78.7% at 12 months, which was similar to other studies reporting 70% to 80% [16,31]. Cases treated with CYP reached remission more rapidly and had a significantly higher cumulative incidence of remission during follow-up, as revealed in Kaplan-Meier curves, compared with patients treated with CsA, even though the CYP-treated patients tended to be older and have a lower eGFR. However, we found no significant differences in the remission rate among other immunosuppressants. CYP was associated with more CRs after 9 months of treatment compared with a CsA-based regimen in a prospective randomized trial [11], whereas CsA combined with corticosteroids reportedly resulted in higher remission rates of nephrotic syndrome compared with cytotoxic drugs plus corticosteroids [32]. In addition, TAC resulted in an improved remission rate compared with CYP, even with the same CNI [33]. As the study populations and designs differed by study, further research is needed to choose appropriate immunosuppressant regimens that can improve remission rates. A recent prospective randomized trial, MENTOR (Membranous Nephropathy Trial of Rituximab), reported that RTX was superior to CsA in maintaining proteinuria remission in high-risk patients [24]. Lower remission rates in RTX-treated patients in this study appear to be related to the lower number of cases produced by a lack of insurance coverage for RTX in Korea. RTX is used primarily as a rescue therapy, and as most of the patients received RTX within 1 year prior to analyses, the follow-up period is considered too short to assess clinical outcomes. The proportions of patients who progressed to ESRD and death also differed by type of immunosuppressants in this study. However, the numbers of patients who reached ESRD and death were relatively small, and it is difficult to compare our results to those of previous studies.
Infection is an important safety issue to be addressed when considering immunosuppressant treatment for iMN patients. Patients receiving immunosuppressants can experience severe adverse events, including infections. The probability of an infection in the immunosuppressant treatment group was 21.8%, which was comparable to the findings of a previous study [14]. Patients in this study experienced infection more frequently when treated with immunosuppressants compared with conservative treatment in the total population, particularly in cases treated with CYP and RTX compared with other immunosuppressant regimens. However, infection events were similar between the two groups in the propensity score-matched population. Anti-PLA2R Ab positivity in the immunosuppressant treatment group was significantly higher in both the total and propensity score-matched populations, suggesting that patients in the immunosuppressive treatment group were more likely to be at high risk, with a low probability of spontaneous remission and a high likelihood of frequent relapses.
As this was a retrospective study, the therapeutic regimen for immunosuppression was chosen at the discretion of the physician, not randomly. In addition, information related to relapse events is lacking. However, the present research is considered to be a meaningful study showing that clinical outcomes were associated with immunosuppressant treatment over the long term in a relatively large number of iMN patients. This study also provides information on the clinical effects of immunosuppressant agents using a propensity score-matched population to reduce the effect of differences in the baseline clinical characteristics of the iMN patients.
In conclusion, the remission rate was significantly higher in the immunosuppressant group compared with the conservative group. The use of immunosuppressants was significantly more effective at achieving remission at 12 months in the subgroup of patients who were young or female or who had relatively heavy proteinuria, and those with good renal function. The cumulative incidence of remission differed significantly by type of immunosuppressant. Further large-scale, well-designed studies are needed to evaluate the effects of immunosuppressants on long-term clinical outcomes in iMN patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









