



Introduction
The survival of premature infants has improved substantially over recent decades. Increased survival of preterm newborns has raised concern regarding increased morbidities. Postnatal complications for premature infants include abnormal kidney function and, in severe cases, kidney failure [1]. Acute kidney injury (AKI) is defined as a sudden decline in kidney function that results in imbalances in fluid levels, electrolytes, and waste products. Recent studies have shown that AKI occurs in 12% to 40% of premature infants and is associated with poor outcomes [1,-3].
Obviously, premature infants are vulnerable to kidney injury because of their immature kidney structure and function. Additionally, aspects of the extrauterine environment, which are experienced indirectly during fetal development, are hostile and detrimental to optimal nephrogenesis, resulting in incomplete glomeruli and tubules. The negative effects include hypoxic damage, sepsis, the presence of nephrotoxic agents, necrotizing enterocolitis (NEC), and patent ductus arteriosus (PDA) [1,2,4,-6].
Premature infants have decreased nephron endowment, which results in low potency to reverse abnormal kidney function [7]. It has been suggested that low birth weight and preterm birth are correlated with microalbuminuria, reduced glomerular filtration rate, hypertension, and focal segmental glomerulosclerosis later in life [8,-10]. Therefore, early detection of AKI is important to prevent the progression of abnormal kidney function in these vulnerable subjects. Currently, the diagnosis of AKI is based on an increase in serum creatinine (Cr) and/or decrease in urine output. However, serum Cr level has limitations for evaluating kidney function in premature infants because neonatal serum Cr reflects maternal levels during the early postnatal period, and these levels decline over days to weeks rather than maintaining a steady state [11]. On the other hand, preterm newborns often have non-oliguric AKI, making oliguria an insensitive marker for the early detection of kidney injury. The purpose of this study was to identify useful urine biomarkers to predict AKI in premature infants.
Methods
Study participants
A prospective cohort study was conducted in a sample of premature infants born at less than gestational age (GA) 37 weeks and admitted to the neonatal intensive care units of two tertiary hospitals during the period from March 2016 to February 2017. This study is registered at ClinicalTrials.gov (NCT02813109). Exclusion criteria included the following: congenital heart anomalies except for PDA, congenital anomalies of the kidney, and transfer from another hospital. Neonates with congenital heart or kidney anomalies are at high risk for AKI because of their physiological vulnerabilities, so that they do not follow the natural course of premature infants. For analyses, infants were divided to 3 groups according to GA following the World Health Organization classification: < 28 weeks (extremely preterm), 28 to < 32 weeks (very preterm), and 32 to < 37 weeks (moderate to late preterm). This study was approved by the Institutional Review Boards of Kangnam Sacred Heart Hospital (IRB No. 2016-05-54) and Inha University Hospital (IRB No. 2016-04-002), and we obtained parental informed consent.
Laboratory evaluations and clinical information
Serum Cr and electrolytes were measured on postnatal days 1, 3, 5, 7, 10, and 14; isotope dilution mass spectrometry was used to measure serum concentrations of Cr and indirect ion selective electrodes were used for assessing serum electrolytes at both hospitals. If venous blood sampling was not required, these values were checked using the iSTAT® CHEM8+ (Abbott, Abbott Park, IL, USA) with capillary blood samples. The lowest serum Cr values after the 2nd day of life were defined as the baseline levels. AKI was classified using the neonatal modified Kidney Disease Improving Global Outcomes (KDIGO) definition [6]. We collected demographic, clinical, laboratory, and outcome data for infants and mothers before birth and during hospitalization. Neonatal severity of illness on neonatal intensive care unit admission was assessed using Apgar scores and clinical risk index for babies (CRIB) II scores [12]. Pathologic features of chorioamnionitis and placental infarction were collected if placental biopsy was performed.
Urine biomarker assays
To measure the concentrations of biomarkers, 1-3 mL of urine was collected at 1, 3, 5, 7, 10, and 14 days of life. Urine specimens were centrifuged, aliquoted, and stored at -70°C until assays were performed. A multiplex Luminex assay® (R&D Systems, Inc., Minneapolis, MN, USA) was used to measure urine biomarkers, which included neutrophil-gelatinase-associated lipocalin (NGAL), interleukin-8 (IL-8), cystatin C, epidermal growth factor (EGF), liver fatty acid binding protein (L-FABP), osteopontin (OPN), and kidney injury molecule-1 (KIM-1). Simultaneously, urine Cr levels were measured using the Cell Biolab Urinary Creatinine Assay Kit (Cell Biolabs, Inc., San Diego, CA, USA). All values were adjusted with urine Cr.
Statistical analysis
Statistical analyses were performed using IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Analyses of clinical data were performed on an intention-to-treat basis, and biochemical data for urine from subjects who completed the protocol were analyzed. We analyzed the results using non-parametric tests due to small sample size. Categorical variables were analyzed using FisherŌĆÖs exact test, and continuous variables were compared using the Mann-Whitney U test. Multivariate logistic regression analysis was performed with adjustments for factors that had P < 0.20 in the univariate analysis. Differences in biomarker levels according to the GA were analyzed using the Kruskal-Wallis test. A P value < 0.05 was considered significant.
Results
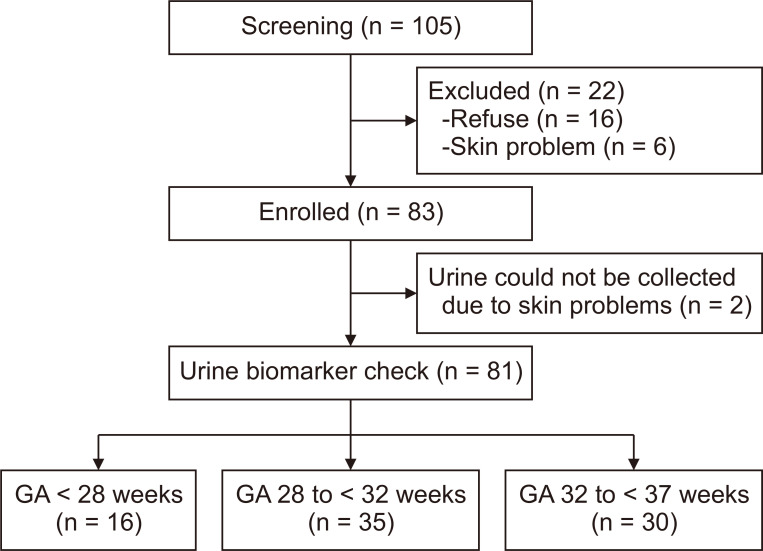
A total of 105 preterm infants were screened for the study, and 22 were excluded due to refusal to participate (n = 16) or skin problems that made it impossible to collect urine samples (n = 6). Eighty-three preterm infants were enrolled. Their median GA and birth weight were 30.7 (interquartile range [IQR], 28.5-33.3) weeks and 1,420 (IQR 1,105-1,860) g, respectively. Urine biomarkers were evaluated in 81 infants, excluding 2 patients for whom we failed to collect urine samples because of skin injuries caused by the attachment of a urine bag (Fig. 1).
AKI occurrence and clinical course
AKI occurred in 17 (20.5%) infants at a median age of 7 (IQR 5-10) days. AKI incidence varied inversely with GA: 72.2% (n = 13) for GA < 28 weeks, 11.4% (n = 4) for GA 28 to < 32 weeks, and 0% for GA 32 to < 37 weeks. Among infants born before GA 28 weeks, infants with AKI had lower incidence of maternal diabetes, lower GA and higher CRIB II scores than those without AKI in the univariate analysis. For infants of GA 28 to < 32 weeks, only birth weight was associated with AKI in the univariate analysis. However, there were no significant differences for any of the above factors in the multivariate regression analysis (Table 1).
According to the neonatal modified KDIGO definition, 10 (12.0%) infants were classified as stage 1, 5 (6.0%) as stage 2, and 2 (2.4%) as stage 3 (Table 2). No patients required kidney replacement therapy during the study period. While the most common cause of AKI was hemodynamically significant PDA (53.8%) in infants of GA < 28 weeks, NEC was the leading cause (50.0%) in infants of GA 28 to < 32 weeks (P = 0.053). The length of hospital stay was not different between the two groups among infants of GA < 28 weeks (no AKI vs. AKI group, median 91 [IQR, 79-99] vs. 96 [85-105] days, P = 0.775). However, length of stay was significantly longer in the AKI group than in no AKI group among infants of GA 28 to < 32 weeks (no AKI vs. AKI group, median 47 [IQR, 42-57] vs. 82 [70-107] days, P = 0.001) (Table 1). Infants with AKI were discharged at a median 39.7 (IQR, 38.3-41.3) weeks of postmenstrual age with estimated glomerular filtration rate of median 97.1 (IQR, 60.5-109.0) mL/min/1.73 m2. While none of them had reduced GFR or abnormal findings on ultrasonography, 30.7% had proteinuria defined as urine protein/Cr ratio greater than 0.5 mg/mg or 2+ or higher on a urine dipstick at discharge (Table 2). Patients with proteinuria could be categorized as having chronic kidney disease following AKI [13].
Urine biomarkers
In infants of GA < 28 weeks, serum Cr levels of AKI groups were significantly higher from day 5 to day 14 compared to those in the no AKI groups (Fig. 2). The levels of urine NGAL/Cr were significantly higher in the AKI group than in the no AKI group from day 3 to day 7 (no AKI vs. AKI group, median 254 [IQR, 202-275] vs. 473 [309-619] ng/mg at day 3, P = 0.027; median 278 [IQR, 252-306] vs. 384 [343-532] ng/mg at day 5, P = 0.005; median 275 [IQR, 121-326] vs. 478 [342-503] ng/mg at day 7, P = 0.013). Regarding the timing of AKI (onset at median 7 [IQR, 7-9] days after birth), urine NGAL/Cr was highest before the onset of AKI in all patients except one (the day of highest urine NGAL/Cr - onset day of AKI, median -4 [IQR, -6.5 to -2] day). The urine cystatin C/Cr levels were significantly higher in the AKI group than in the no AKI group at day 7 (no AKI vs. AKI group, median 1,799 [IQR, 1,090-2,639] vs. 5,658 [5,278-15,113] ng/mg, P = 0.04). Regarding timing with AKI, urine cystatin C/Cr was highest at a similar point with the onset of AKI (the day of highest urine cystatin C/Cr - onset day of AKI, median 0 [IQR, -3.5 to 1] day). The urine EGF/Cr levels were significantly lower in the AKI group than in the no AKI group at day 5 (no AKI vs. AKI group, median 24.9 [IQR, 23.4-29.6] vs. 16.3 [13.9-22.0] ng/mg, P = 0.019). Regarding the timing of AKI, urine EGF/Cr was lowest at a similar point with the onset of AKI (the day of lowest urine EGF/Cr - onset day of AKI, median 0 [IQR -1.5 to 1.5] day). There were no differences in the levels of other urinary biomarkers between the two groups (Fig. 2).
In infants of GA 28 to < 32 weeks, serum Cr levels were not different between the two groups because AKI was defined as decreased urine output (< 0.5 mL/kg/hour for 6 hours) without an increase of serum Cr level in 1 patient and 3 of 4 patients had stage 1 AKI (Table 2, Fig. 3). The urine NGAL/Cr levels were significantly higher in the AKI group than in the no AKI group at day 14 (no AKI vs. AKI group, median 79 [IQR, 37-146] vs. 277 [116-437] ng/mg, P = 0.034). Regarding timing with AKI, urine NGAL/Cr was highest before the onset of AKI in 2 of 4 patients, but not in the other 2 patients (the day of highest urine NGAL/Cr - onset day of AKI, -5, -4, 3 and 7 day, respectively). The levels of urine IL-8/Cr were significantly higher in the AKI group than in the no AKI group at days 7 and 10 (no AKI vs. AKI group, median 148 [IQR, 90-339] vs. 397 [303-5,954] pg/mg at day 7, P = 0.033; median 124 [IQR, 78-240] vs. 378 [241-745] pg/mg at day 10, P = 0.023, respectively). Regarding the timing with AKI, urine IL-8/Cr was highest before or at the onset of AKI in all patients (the day of highest urine IL-8/Cr - onset day of AKI, -6, -3, 0 and 0 day, respectively). There were no differences in the levels of other urine biomarkers between the two groups.
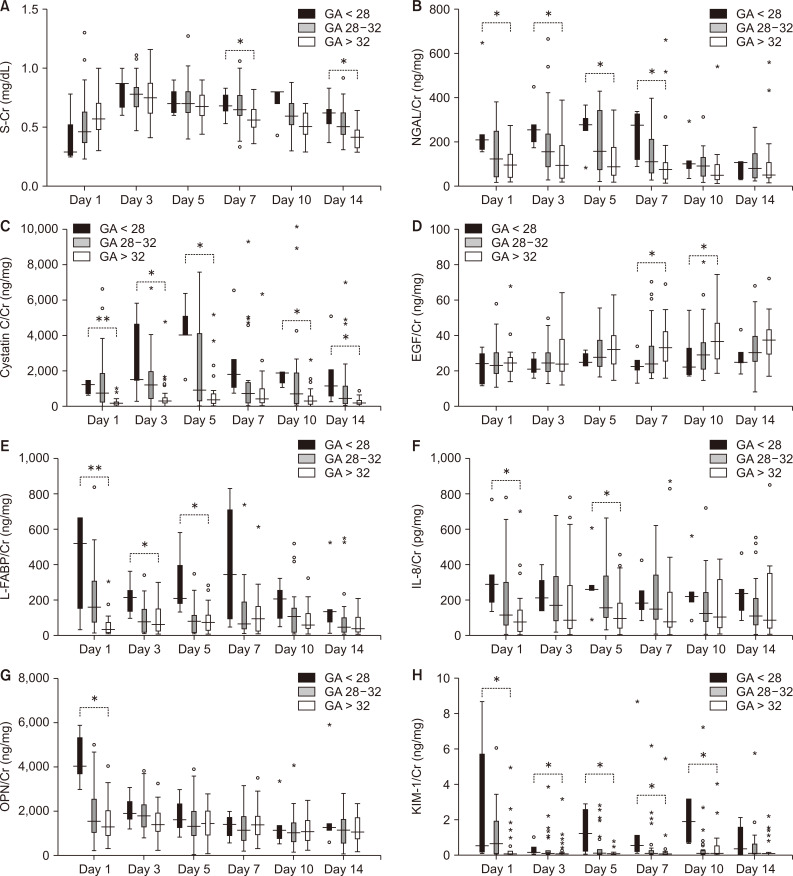
Among infants without AKI, urine biomarker levels were different according to GA groups (Fig. 4). Consistent with previous reports [14,-16], urinary levels of NGAL/Cr, cystatin C/Cr, L-FABP/Cr and KIM-1/Cr were inversely correlated with GA, especially during the first week of life. In contrast, urinary EGF/Cr levels increased significantly with GA at postnatal days 7 and 10 in this study. In addition, the urinary levels of NGAL, cystatin C and L-FABP decreased after 1 week of life compared to the first postnatal week. Urinary OPN/Cr levels were not affected by GA or the day after birth.
Discussion
In this prospective cohort study, we found that urinary biomarkers associated with the development of AKI differed according to the GA. While urinary NGAL levels were significantly higher prior to the onset of AKI among infants of GA < 28 weeks, they did not differ prior to AKI in infants of GA 28 to < 32 weeks. Similarly, while urinary cystatin C and EGF levels were significantly different at the onset of AKI between groups among infants of GA < 28 weeks, they did not differ between groups in infants of GA 28 to < 32 weeks. The urinary IL-8 levels were significantly higher in the AKI group before or at the onset of AKI only in infants of GA of 28 to < 32 weeks.
Some studies have shown urinary and serum NGAL levels can be useful as predictive markers of AKI in premature infants [17,-19]. On the other hand, one pilot study performed among premature infants with a mean GA of 29.6 weeks reported that urine NGAL levels were associated with AKI but failed to predict AKI [20]. According to a recently published case-control study based on a prospective cohort of premature infants (mean GA 25.2 weeks), urinary NGAL and EGF levels predict AKI development prior to changes in serum Cr [19]. The differences among results of previous studies may be due to differences in the GA of the infants included in these studies. Our study also showed that urinary NGAL levels were meaningful as prediction markers in infants born before GA 28 weeks but not in infants of GA 28 to < 32 weeks. In infants of GA < 28 weeks, serum Cr differed between the AKI group and the no AKI group from the fifth day after birth, but NGAL/Cr begins to differ from the third day after birth (Fig. 1). Therefore, urinary NGAL/Cr could be an early biomarker to diagnose AKI in extremely premature infants.
AKI is a very complex, heterogeneous disorder that occurs with varying degrees of severity in different clinical situations. Our results support the hypothesis that the pathophysiology of AKI in premature infants depends on immaturity and the urinary biomarkers examined and according to GA. Extremely preterm infants born before GA 28 weeks have few nephrons or very immature nephrons [21]. Their postnatal kidney maturation can be accelerated or arrested by various factors in the extrauterine environment [5,22]. In extremely premature infants, the most important mechanism of AKI would be related to the disruption or arrest of normal maturation of the kidneys. The significantly lower levels of urinary EGF in infants with AKI could be interpreted in a similar manner. One longitudinal investigation of urine biomarkers in preterm infants demonstrated that urine EGF levels increased as kidney maturation progressed with advancing gestation [23]. EGF is a growth factor that stimulates cell growth, proliferation, and differentiation by binding to its receptor. Experimental studies showed that the activation of EGF receptor located on proximal tubules is essential for kidney development and recovery from AKI [23,24].
Interestingly, the levels of urinary IL-8 were associated with AKI in infants of GA 28 to < 32 weeks. IL-8 is a powerful chemokine involved in tissue neutrophil recruitment. The high levels of IL-8 in AKI group reflect increased inflammation related to the development of AKI in this group [25,-27]. Systemic inflammation frequently occurred in premature infants, including bacterial sepsis and NEC. Although the incidence of sepsis was not different between groups, 50% of infants with AKI had stage 2 or higher NEC (vs. 12.9% in the no AKI group) among infants of GA of 28 to < 32 weeks (Table 2). One patient classified as having an unknown cause of AKI had histological chorioamnionitis, and Ureaplasma urealyticum was identified in the first gastric juice, which was regarded to have originated as amniotic fluid. This patient also showed a leukemoid reaction for the first 2 weeks of life (white blood cell, 57,000-112,800/╬╝L) without any infection focus, which resolved spontaneously. In an animal model of AKI, inflammatory cytokines including keratinocyte-derived chemokine (KC, the murine analogue of IL-8) increased early in the process of AKI [28]. In addition, KC/IL-8 receptor knockout mice were protected against colitis-induced AKI and inflammation [27]. According to these findings, inflammation might be a major cause of AKI in premature infants born after 28 weeks of gestation.
Askenazi et al [15] reported that the urine levels of NGAL, KIM-1, OPN, and cystatin C decreased with increasing GA and suggested that those findings should be considered when analyzing biomarkers in newborns with AKI. Our results support this hypothesis. In this study, urinary levels of NGAL, KIM-1, cystatin C, L-FABP, and IL-8 were inversely associated with GA in infants without AKI (Fig. 4). In contrast, urinary EGF/Cr levels increased significantly with GA after 1 week of birth. Because nephrogenesis is not complete but rather is ongoing, urinary biomarkers should be evaluated and used after stratification for gestation and postnatal day in preterm infants.
Several factors need to be considered as limitations in this study. To define AKI, we defined the lowest serum Cr level after the 2nd day of life as the baseline value because neonatal serum Cr on the first day of life reflects maternal levels, and diuresis usually occurs within 2 to 3 days after birth. Indeed, initial neonatal serum Cr levels were significantly correlated with maternal serum Cr levels in our sample (PearsonŌĆÖs correlation r = 0.556, P < 0.001). However, serum Cr after the 2nd day of life may also be affected by several co-morbidities in premature infants that impact their hemodynamic status, such as PDA, intraventricular hemorrhage, and ventilator support. Second, as the stratification for GA and lack of AKI was determined in infants of GA > 32 weeks, the number of infants actually included in the analysis was reduced from the original 83 infants to 53. Because premature infants born after GA 32 weeks are at low risk for AKI, future studies of urinary biomarkers for AKI should focus on very premature infants born before GA 32 weeks. Third, the number of AKI patients in each GA group was small. A larger prospective study could provide more meaningful results about urine biomarkers for AKI in premature infants.
In conclusion, several urine biomarkers were significantly different between infants with and without AKI and, and some of the biomarkers had changed before the onset of AKI in premature infants. Which urine biomarkers are meaningful may differ according to the causative factors of AKI and GA. Urine biomarkers could be useful for predicting the development of AKI when interpreted appropriately according to the clinical situation.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









