


Introduction
Yersinia pseudotuberculosis is a gram-negative organism and a zoonotic pathogen detected in various animal reservoirs [1]. It is widespread in the environment and transmitted through unsterilized water or contaminated food (such as iceberg lettuce and carrots) [2,3]. Gastro-enteritis and mesenteric lymphadenitis are the most common forms of Y. pseudotuberculosis infection [4], presenting with fever and abdominal pain, mimicking appendicitis [5,6]. Y. pseudotuberculosis infection is known to be self-limited [7], but in severe cases with bacteremia or gastrointestinal bleeding, it needs to be treated with antibiotics because it shows high mortality [8–10]. Y. pseudotuberculosis infection can also be accompanied by cutaneous rash and desquamation or thrombocytosis resembling Kawasaki disease [11]. It may also impair renal function; in previous reports from Korea, acute kidney injury (AKI) developed in 13.6% of cases [12,13], which had a benign course, and renal replacement therapy was required in 2% to 14% [12,14,15].
There were a few publications on Y. pseudotuberculosis infection associated with mountain well or unsterilized water in Korea [12,15,16]. In Japan, outbreaks of infection by Y. pseudotuberculosis also occurred frequently in the late twentieth century, which was called Izumi fever before the etiology was discovered as being linked to Y. pseudotuberculosis infection [17]. Most patients had fever, gastrointestinal symptoms, and desquamation, resembling acute appendicitis or Kawasaki disease [11]. Multiple outbreaks of Yersinia infection have been increasingly reported worldwide and were found to be associated with raw food and animals by epidemiological and environmental investigation [2,3,18].
In Korea, since 1996, there has been no report of any Y. pseudotuberculosis outbreaks, leading us to consider it as eradicated due to improvements in public health. However, in 2017, we encountered several children who presented with a typical clinical course of Y. pseudotuberculosis-associated AKI. Here, we report our experience thereof.
Methods
We retrospectively reviewed children who presented at Seoul National University Children’s Hospital in 2017 with AKI, which was suspected to be associated with Y. pseudotuberculosis infection. Clinical diagnosis of Y. pseudotuberculosis-associated AKI was made when the patient had AKI, gastrointestinal symptoms, and fever, and other plausible causes including hypovolemia were not found. AKI was defined when there was an increase in creatinine (Cr) level by 0.3 mg/dL, a 50% increase in Cr level from baseline, or urine output less than 0.5 mL/kg/hour for more than 6 hours. Serum Cr concentration at discharge from hospitalization was considered as the baseline value [19]. Their medical records including demographics, clinical manifestations, laboratory findings, and treatment were reviewed. Ultrasonography findings or abdomen computed tomography (CT) scan results were also reviewed.
When patients and their guardians agreed, blood samples from patients were tested for anti-Yersinia antibodies as previously reported [20]. Serum samples were analyzed at the Division of Bacterial Diseases, Center for Laboratory Control of Infectious Diseases, Korea Centers for Disease Control and Prevention (KCDC). Immunoglobulin (Ig) A and IgG binding to Yersinia outer proteins (Yops) was quantified by enzyme-linked immunosorbent assay (ELISA) using a commercial kit, Serion ELISA classic Yersinia IgG/IgA (Serion, Würzburg, Germany). Measurements were repeated six times, and the mean value was reported. The result was regarded as positive when the optical density (OD) (405 nm) of IgG was more than 0.35 and the OD (405 nm) of IgA was more than 0.56 according to the manufacturer’s instructions. To culture the Yersinia species in the stool, cefsulodin-irgasan-novobiocin agar was used.
Estimated glomerular filtration rate (eGFR) was calculated by the updated bedside Schwartz equation: eGFR = 0.413 × height (cm)/serum Cr (mg/dL). Proteinuria was referred to as urine protein/urine Cr ≥ 0.2 mg/mg in the first morning urine or albuminuria ≥ 1+ in dipstick urinalysis.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee under which the studies were conducted (Institutional Review Board [IRB] of Seoul National University Hospital, IRB approval number: H-1810-146-983) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Results
Demographics
In 2017, a total of nine patients (male:female, 6:3) at our center were clinically diagnosed with Y. pseudotuberculosis-associated AKI and enrolled in this study. The presenting months were May for six patients, and February, April, and November for the others. The mean age was 7.5 years (range, 2.9–12.1 years). Six patients resided in Seoul, two in Gyeonggi Province, and one in Jeollabukdo. Only three patients recalled a history of drinking untreated well or mountain water. Another three patients had other family members having similar symptoms diagnosed as acute gastroenteritis or scarlet fever within one week of the patient’s visit. Since we experienced a cluster of patients with clinical diagnosis of Y. pseudotuberculosis-associated AKI in May, we reported this presumed outbreak to the KCDC. Epidemiological and environmental investigations were conducted by KCDC; however, infection sources were not identified [21].
Clinical manifestation
Table 1 shows the clinical manifestation and clinical course of the patients. Generally, fever was the first symptom, followed by gastrointestinal symptoms, rash, and renal manifestation, and desquamation developed as the last symptom when present. Every patient first presented with fever. The mean duration of fever was 13 days (range, 6–20 days). Fever was persistent (monophasic) in six patients, while it had subsided but returned once (biphasic) in two patients or twice (triphasic) in one patient. Then, gastrointestinal symptoms of abdominal pain and/or diarrhea or loose stool were seen. Maculopapular rash was later observed in four patients, and three showed desquamations, resembling Kawasaki disease. None of them showed strawberry tongue or erythema nodosum-like cutaneous manifestation. In a median of six days after fever onset, oliguria < 0.5 mL/kg/hour of urine output was noted in five patients, and two showed decrease in urine output to < 1 mL/kg/hour. Oliguria persisted for a median of five days (range, 4–17 days) accompanied by generalized edema or pleural effusion that resolved along with improvement in renal function. Hypertension also developed in four patients, and one of them presented with posterior reversible encephalopathy syndrome.
Laboratory and imaging findings
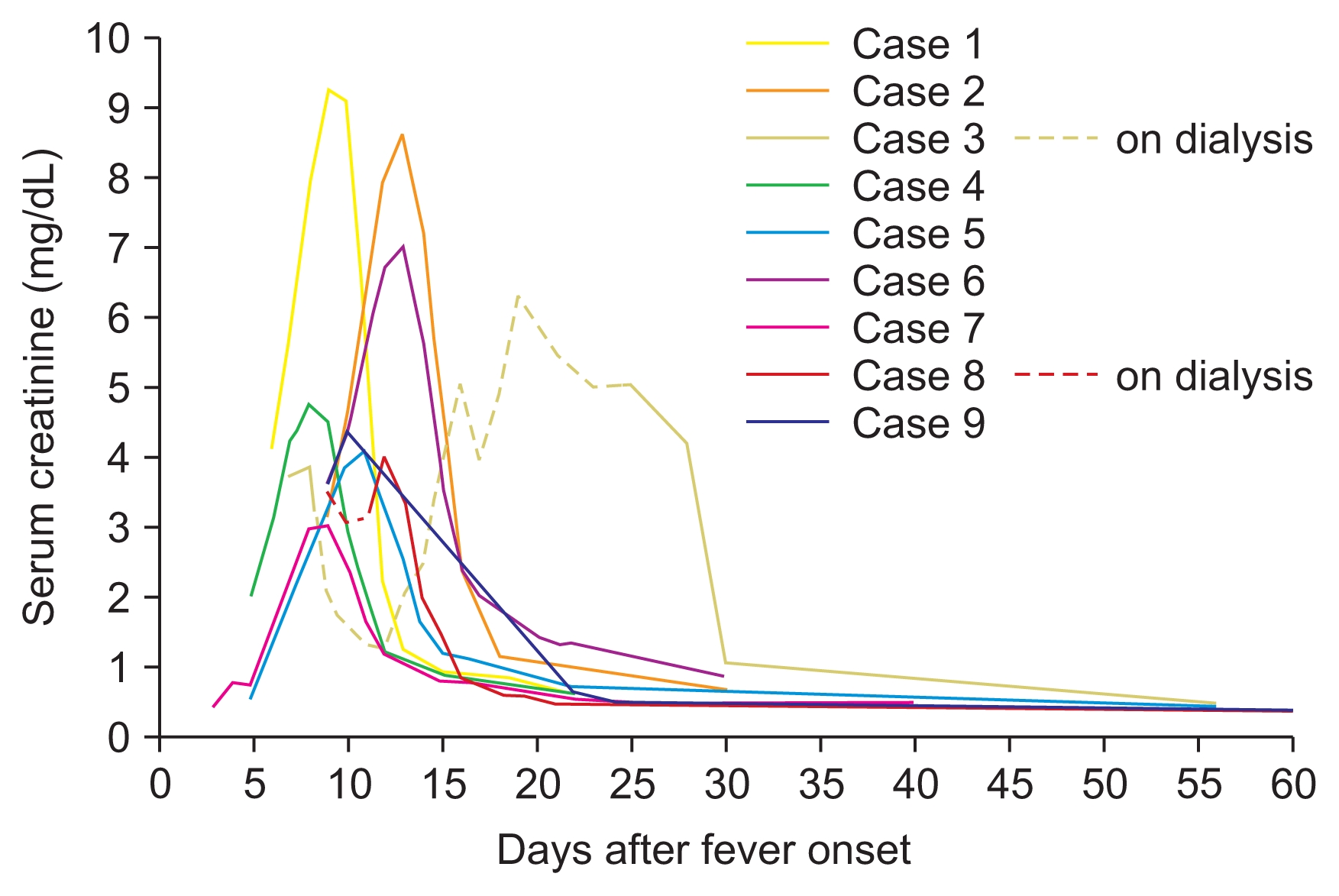
Leukocytosis (white blood cell [WBC] count > 10,000/mm3) and anemia (hemoglobin level lower than the normal value adjusted for sex and age) were noted in all patients. Thrombocytosis (platelet count > 400,000/mm3) was detected in seven cases (77.8%). C-reactive protein level was markedly elevated in all patients; the mean value was 24.04 mg/dL. Erythrocyte sedimentation rate also accelerated to > 20 mm/hour when tested (n = 5). Serum Cr level increased in all patients, with the average peak value of 5.72 mg/dL (range, 3.03–9.22 mg/dL; Fig. 1). Urine analysis revealed proteinuria (median peak urine protein/Cr level, 2.28) in every patient, glucosuria in eight (88.9%), sterile pyuria in seven (77.8%), and microscopic hematuria in four patients (44.4%) (Table 2). Fractional excretion of sodium (FENa) was greater than 1% in eight patients tested, with average value of 4.8% (range, 1.2–13.4). The Widal test, which is known to cross-react with the Yersinia antigen [22], was performed in eight patients, but only one patient showed a positive result with a Widal test O titer of 1:160. Complement levels of C3 and C4 were normal when tested (n = 6). Stool culture was done in every patient, and Y. pseudotuberculosis was isolated in only one patient.
Increased renal parenchymal echogenicity or renal parenchymal swelling was found in all seven patients who underwent kidney ultrasonography (100%). In abdominal ultrasonographic (n = 6) or CT (n = 3) findings, the wall of the terminal ileum or ascending colon was thickened in five patients (71.4%, 5/7). Increased or enlarged echogenicity of mesenteric lymph nodes was noted in four patients (57.1%, 4/7). Furthermore, four patients showed gallbladder wall edema (44.4%, 4/9), and six had ascites (66.7%, 6/9). Echocardiography was performed in eight patients, revealing that there was neither coronary artery dilatation nor cardiac dysfunction.
Management and follow up
The mean disease duration between the onset of symptoms and discharge from hospitalization was 19 days (10–32 days). All patients received conservative treatment including fluid therapy. All patients were initially treated with antibiotics including 3rd-generation cephalosporin, piperacillin/tazobactam, or metronidazole, targeting bacterial enteritis. Antibiotic administration was discontinued when Y. pseudotuberculosis infection was suspected and blood culture turned out negative. Diuretics were administered in six patients to manage oliguria and generalized edema. Renal replacement therapy was required in two patients, intermittent hemodialysis in one, and continuous renal replacement therapy in another. At discharge, serum Cr level was normalized in every patient (Fig. 1).
Seven patients were followed for more than three months (median, 216 days; range, 198–517 days). At the last follow-up, one patient (case 7) showed decreased eGFR (81.8 mL/min/1.73 m2). No proteinuria was noted.
Anti-Yersinia species antibody
The serum samples were collected within three months after their first presentation of symptoms to test for the presence of anti-Yersinia antibodies (median, 55 days; range, 49–72 days). Anti-Yersinia IgA and IgG were assessed in six patients, and every patient showed positive results compared to their earlier sample (Table 3). The median IgG titer was 1.49 (range, 1.37–1.68), and the mean IgA titer was 0.9 (range, 0.66–1.98). Follow-up samples after six months were available in four patients. The IgG titers of the four patients were still positive in the second test with a mean value of 1.48. Meanwhile, the IgA value decreased in two patients and increased in the rest.
Discussion
Only four cases of Y. pseudotuberculosis infection were previously reported in Korea since 2000 [16,23–25]. While Y. pseudotuberculosis has been considered to have been eradicated for a decade in Korea, we encountered a cluster of patients clinically diagnosed with Y. pseudotuberculosis-associated AKI in 2017. Similar to previous reports from Korea and Japan [11,15,17], fever was the first presenting symptom in every case of this study, followed by gastrointestinal symptoms and AKI approximately six days later. None of the patients had conjunctival injection nor erythema nodosum, unlike in previous reports [13]. The laboratory findings of our cases, which included azotemia, thrombocytosis, leukocytosis, anemia, and elevated inflammatory markers, were also common. Abnormal urine findings including sterile pyuria, glucosuria, elevated urine beta-2-microglobulin (data not shown), and elevated FENa implied tubulointerstitial nephritis. Three of the nine patients demonstrated eosinophilia (data not shown). Imaging findings were also compatible with a Y. pseudotuberculosis-associated condition; ileal wall thickening and enlarged mesenteric lymph nodes suggesting ileitis and mesenteric lymphadenitis are known as characteristic findings in yersiniosis [26,27]. Ultrasonographic examination of the kidney also revealed characteristic features of tubulointerstitial nephritis, including increased renal parenchymal echogenicity and renal swelling, consistent with previous reports [28,29]. All cases recovered eventually with conservative management only or renal replacement therapy. Compared to patients that did not receive dialysis, dialyzed patients had more severe pyuria. Both patients who received dialysis had urine WBC greater than 50/high power field (HPF), while all the others had urine WBC below 50/HPF. There were no significant differences in clinical manifestations.
Y. pseudotuberculosis used to be diagnosed with stool culture, blood culture, or hemagglutination test [11,13]. These methods are useful to detect active enteritis, but there are limitations to the diagnosis of other manifestations of yersiniosis and chronic infection [30]. Furthermore, culture of this bacterium is difficult, has low sensitivity, and is time consuming, requiring cold temperature and special media [11,31]. Since 1979, ELISA has been used to detect yersiniosis [32], and the plasmid encoded proteins Yops were found to be pathogenic and specific antigens helpful in the serodiagnosis of yersiniosis [33]. Several studies reported that ELISA and immunoblot assay for Yop-specific antibodies were more sensitive and specific than the routine agglutination test or stool culture [34,35], and these methods were proven useful for Y. pseudotuberculosis infection as well [20,27]. Reportedly, antibodies of all classes (IgG, IgA, IgM) appear during the acute phase of Yersinia infection, and IgG antibodies may exist for several years while IgM disappears about three months after infection. The presence of IgA has been regarded as an indicator of recent infection but usually decreases following IgM antibodies [34,36]. However, the persistence of IgA antibodies for more than two years after infection has also been reported, in association with probable chronic infection [37].
In the present study, marked elevation of IgG and IgA against Yops was noted from every sample obtained within three months after the onset of disease. In the follow-up test carried out six months later, IgA titer decreased in two patients and increased in the others, while IgG remained positive in all four patients, implying recent infection of Yersinia. However, elevation of IgG and IgA antibodies to Yops implicates Yersinia species infection, not exclusively Y. pseudotuberculosis infection. However, Y. pseudotuberculosis is the only organism among Yersinia species that causes tubulointerstitial nephritis to our knowledge; therefore, the results of anti-Yersinia antibodies in our cases support the diagnosis of Y. pseudotuberculosis infection along with their clinical course, laboratory findings, and imaging findings.
AKI in children with gastrointestinal symptoms raises suspicion of a few conditions. One should consider (i) prerenal azotemia in gastroenteritis, where hydration often reverses azotemia. However, our patients did not recover renal function despite adequate hydration. Moreover, their azotemia was associated with tubulointerstitial nephritis from early on since their FENa was over 1%, therefore not compatible with prerenal azotemia from dehydration. (ii) Hemolytic uremic syndrome also presents as AKI along with gastrointestinal symptoms and anemia; it can be distinguished by the presence of schistocytes in a peripheral blood smear, thrombocytopenia, and Escherichia coli growth in stool culture [38]. None of our patients had thrombocytopenia; therefore, hemolytic uremic syndrome could be ruled out. (iii) Gastrointestinal symptoms mimicking appendicitis often lead to an investigation with abdominal CT with contrast media; three of the nine patients underwent abdominal contrast CT; therefore, contrast-induced AKI needs to be considered as the cause of AKI; however, one patient already had azotemia before taking abdominal CT, and another had Y. pseudotuberculosis growth in stool culture. Thus, we assume that AKI in these cases was mainly associated with Y. pseudotuberculosis rather than contrast media. Still, there is a possibility that contrast usage affected the kidney function in these patients.
Prolonged fever, rash, sterile pyuria, and desquamation are symptoms of Kawasaki disease; there have been several reports that Y. pseudotuberculosis-infected children fulfilled the criteria of Kawasaki disease [11] Furthermore, 9% of patients with Kawasaki disease showed elevated antibody titers of Y. pseudotuberculosis and/or positive stool culture in a Japanese study [39]. It has also been suggested that Y. pseudotuberculosis infection might play a role in Kawasaki disease [40]. Among our cases, however, none met the criteria of Kawasaki disease. Echocardiography was performed in eight of nine patients, and none of them showed coronary aneurysm or cardiac dysfunction.
Y. pseudotuberculosis is a zoonotic pathogen and transmitted through unsterilized water [1]. Currently, Y. pseudotuberculosis is not included in the sentinel or mandatory surveillance systems in Korea; therefore, presence or absence of Y. pseudotuberculosis in unsterilized water in Korea is unclear. However, our report indicates that Y. pseudotuberculosis is still present in Korea. In Finland and France, clinical microbiology laboratories routinely report Y. pseudotuberculosis, so that the increase in Y. pseudotuberculosis isolations was rapidly recognized [3,18]. It might be necessary to build a surveillance system or laboratories available for early detection also in Korea.
Y. pseudotuberculosis-associated AKI should be considered when a patient presents with fever, acute gastroenteritis, and AKI not resolving despite hydration. Since Y. pseudotuberculosis-associated AKI is usually self-limiting, early suspicion and appropriate supportive care could save medical resources. Y. pseudotuberculosis-associated AKI is likely to be under-recognized because of inadequate knowledge, lack of diagnostic tools, and low surveillance in Korea; therefore, surveillance for Y. pseudotuberculosis is necessary, as are laboratory tests to diagnose Y. pseudotuberculosis infection.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









