The differential effects of anemia on mortality in young and elderly end-stage renal disease patients
Article information

Abstract
Background
The aim of this study was to compare the effect of anemia on clinical outcomes according to age in patients with end-stage renal disease (ESRD).
Methods
A total of 3,409 patients from the Clinical Research Center for ESRD were included and divided into three groups by age: age < 40 (n = 488), 40 ≤ age < 60 (n = 1,650), and age ≥ 60 (n = 1,271). We compared overall and cardiovascular mortality, and all-cause and cardiovascular hospitalization according to mean hemoglobin (Hb) concentration.
Results
Among participants ≥ 60 years of age, the Hb < 10 g/dL group had greater all-cause mortality (adjusted hazard ratio [HR], 2.098; 95% confidence interval [CI], 1.567-2.808; P < 0.001) than the 10 ≤ Hb < 12 g/dL group, whereas among participants < 40 years of age, the Hb ≥ 12 g/dL group had greater mortality than the 10 ≤ Hb < 12 g/dL group. Moreover, in participants ≥ 60 years of age, the HR for all-cause hospitalization for the Hb < 10 g/dL group was significantly greater than that of the 10 ≤ Hb < 12 g/dL group (HR, 1.472; 95% CI, 1.057-2.051; P = 0.022), whereas it was significantly lower in the Hb ≥ 12 g/dL group (HR, 0.544; 95% CI, 0.362-0.820; P = 0.004) However, among participants < 40 years of age, the incidence of all-cause hospitalization did not differ according to the Hb concentration (HR, 1.273; 95% CI, 0.814-1.991; P = 0.290 for the Hb < 10 g/dL group; reference, 10 ≤ Hb < 12 g/dL; HR, 0.787; 95% CI, 0.439-1.410; P = 0.265 for Hb ≥ 12 g/dL group).
Conclusion
The impact of anemia on mortality was more significant in elderly ESRD patients. Strict monitoring and management of anemia should be required for elderly ESRD patients.
Introduction
Anemia is an important complication of end-stage renal disease (ESRD), and treatment of anemia is correlated with an improvement in the patient’s quality of life, and with a reduction in morbidity and mortality [1-3]. Therefore, it is strongly recommended to use erythropoiesis-stimulating agents (ESAs) and iron therapy, which are considered beneficial for the correction of anemia, in patients with ESRD [4,5]. However, the results of some studies have suggested potential harm due to overtreatment of anemia when employing ESAs, defined as achieving a hemoglobin (Hb) concentration of 12 g/dL and above, which may potentially lead to increased cardiovascular events and mortality [6,7]. The Kidney Disease Improving Global Outcomes (KDIGO) guidelines therefore currently recommend maintaining Hb concentrations between 10 to 12 g/dL in clinical practice [4].
Despite these recommendations, a previous report suggested that the optimal Hb concentration may vary according to the patient’s age [7]. This report found that in children on hemodialysis (HD), Hb concentrations of 12 g/dL and above are not associated with increased incidences of cardiovascular visits, mortality, or all-cause and cardiovascular disease (CVD)-related hospitalizations, in contrast to the reported harmful impact of overcorrected Hb in adult ESRD patients. Another study reported that anemia resulted in a more significant impact in elderly ESRD patients than in younger patients with respect to CVD and ESRD-related mortality of that population demographic [6,7]. These studies suggest that anemia and/or overcorrected Hb are associated with differential impacts on patient outcomes according to the patient’s age.
Based on above findings, the aim of this study was to investigate whether anemia is associated with differential impacts on clinical outcomes according to age group using a well-established nation-wide ESRD cohort within Clinical Research Center for ESRD (CRC-ESRD).
Methods
Study population
We analyzed the CRC-ESRD data. The CRC-ESRD database contained a total of 5,244 cases from 31 centers in Korea. The cohort was established in April 2009, and included adult (> 18 years of age) dialysis patients. For the present study, we excluded patients whose age data was not available, or whose Hb concentrations had not been measured at least three times during the study period; a total of 1,835 patients were excluded, and 3,409 patients were included in the final analyses (Fig. 1).
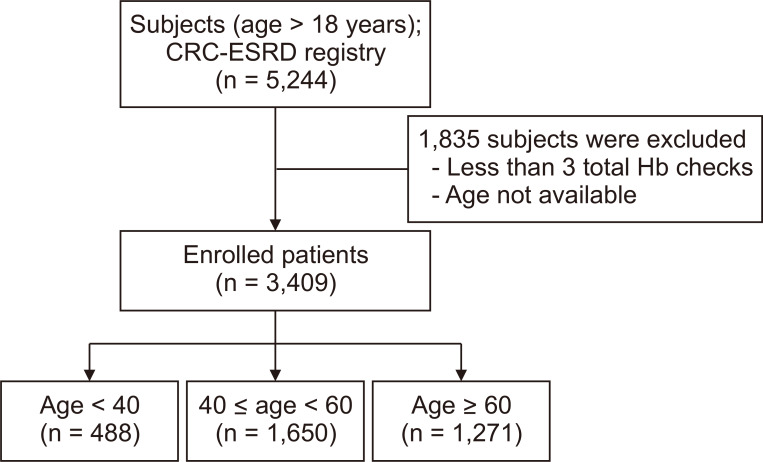
Distribution of patient population according to patient age.
Of the 5,244 subjects included in the Clinical Research Center for end-stage renal disease (CRC-ESRD) registry, 1,835 subjects were excluded due to lack of information regarding age or hemoglobin (Hb) concentration. Therefore, 3,409 patients were included: 488 were younger than 40 years of age, 1,650 were between 40 and 60 years of age, and 1,271 were 60 years of age or older.
A total of 2,058 patients on HD, 1,332 patients on peritoneal dialysis (PD), 7 patients with changes in treatment modality (HD → PD or PD → HD), and 12 patients with missing data regarding treatment modality were enrolled in this cohort. Additionally, 1,157 incident and 2,252 prevalent dialysis patients were included in the analyses.
The CRC registry for ESRD was approved by the medical ethics committees of all participating hospitals, and informed consent was obtained from all patients before inclusion. All participants were assigned to one of three groups (age < 40, 40 ≤ age < 60, or age ≥ 60 years) according to their age at enrollment of this study for maintained HD patients, or according to their age at the initiation of dialysis for incidental dialysis patients.
Data collection
This was a prospective cohort study of dialysis patients in Korea receiving HD for ESRD during the years 2009 to 2015. The baseline demographic and clinical data, including age, sex, and laboratory investigations, were recorded for all patient participants. For the assessment of mean Hb concentration, we calculated the average of every serum Hb measurement during the follow-up period. The patients were divided into 3 groups according to their mean Hb concentration as Hb < 10 g/dL, 10 ≤ Hb < 12 g/dL, and Hb ≥ 12 g/dL [7]. We also categorized patients according to age as < 40 years, 40 ≤ age < 60 years, and age ≥ 60 years [8].
Baseline demographic and clinical data including age, gender, height, weight, co-morbidities, laboratory investigations, and therapeutic characteristics were recorded. Additionally, serum Hb, albumin, ferritin, transferrin saturation (TSAT) concentrations were determined from the patients’ blood samples. The single-pool Kt/V (spKt/V) was determined using two-point urea modelling based on the intradialytic reduction in blood urea and intradialytic weight loss. For assessment of co-morbidities, modified Charlson comorbidity scores were used.
Outcomes
The primary outcome of this study was a review of all-cause mortality. For each death, the principal investigator at the given institution completed a form recording the cause of death according to the CRC registry for ESRD study classification. The median follow-up duration was 24.4 months (3 to 81 months), and the dates and causes of mortality were immediately reported throughout the follow-up period. Additionally, the secondary outcomes of this study were CVD-related mortality, all-cause hospitalization, and CVD-related hospitalization. A report of CVD-related mortality or hospitalization referred to death or admission due to a cardiovascular event, such as heart failure, arrhythmia, ischemic cardiovascular event, or stroke.
Statistical analyses
The patient characteristics were examined using descriptive statistics for continuous variables (mean, median) and categorical variables (number [%]), and the results were stratified by patient Hb concentration at baseline. A χ2 tests for independence was used to test for differences by Hb group. Similarly, we summarized the outcomes (death, hospitalizations, and cardiac events) with descriptive statistics (number [%]). Broadly speaking, the confidence intervals (CIs) were estimated using a normal approximation of the Poisson distribution. Last, we estimated the adjusted HR of mortality using a Cox proportional hazards model. In this case, the models were adjusted for all patient demographic and clinical characteristics studied, such as gender, primary renal disease, duration of dialysis, modified Charlson comorbidity index, and mean intact parathyroid hormone level (iPTH). All results were stratified by mean Hb groups with Hb concentrations with 10 to < 12 g/dL as the reference, P values less than 0.05 were considered statistically significant. All analyses were conducting using IBM SPSS Statistics for Windows ver. 21.0 (IBM Corp., Armonk, NY, USA) and MEDCALC version 15.5 (MedCalc, Mariakerke, Belgium).
Results
Baseline characteristics
Among the study population, 14.3% (n = 488) were < 40 years of age, 48.4% (n = 1,650) were 40 ≤ age < 60 years of age, and 37.3% (n = 1,271) were ≥ 60 years of age. Table 1 presents the baseline characteristics among different groups according to the patient’s age. Generally, the gender distribution was not different within groups. The cause of ESRD was different according to the patients’ ages, and diabetes mellitus (DM) was the most common cause of ESRD in the age ≥ 60 years group (49.3%). In contrast, glomerulonephritis was the most common cause of ERSD in both of the younger age groups (age < 40 years and 40 ≤ age < 60 groups; P < 0.001 for each). There were no differences between the mean durations of dialysis in all the groups (P = 0.106), which were 24.6 months (± 1.8) in the age < 40 group, 29.3 (± 1.1) months in the 40 ≤ age < 60 group, and 28.0 (± 1.2) months in the age ≥ 60 months group. Mean serum albumin concentrations, which generally reflect the nutritional status of dialysis patients, did not differ among the three age groups (P = 0.337). Other anemia profiles, such as mean serum ferritin and TSAT concentrations also did not differ between the groups (P = 0.126, P = 0.136 for each).

Comparison of the baseline characteristics of the study population according to patient age
Overall patient survival
A total of 363 deaths were reported among the overall study population during the follow-up period (24.4 months; range, 3-81 months). In the overall patient population, the patient survival rate was greatest in the 10 ≤ Hb < 12 g/dL group, but there was no difference between the Hb ≥ 12 g/dL and Hb < 10 g/dL groups (P = 0.459; Fig. 2A). Within the 40 ≤ age < 60 years and age ≥ 60 years groups, the 10 ≤ Hb < 12 g/dL group had significantly superior overall patient survival compared to the Hb < 10 g/dL group (P = 0.006 for the 40 ≤ age < 60 years; P < 0.001 for the age ≥ 60 years). There was a trend toward better overall patient survival in the Hb ≥ 12 g/dL group compared to the Hb < 10 g/dL group, but the difference was not statistically significant (P = 0.919 for the 40 ≤ age < 60 years group; P = 0.086 for the age ≥ 60 years group; Fig. 2C, D). The Hb ≥ 12 g/dL group had inferior overall survival than the 10 ≤ Hb < 12 g/dL group (P = 0.034), whereas survival of the Hb < 10 g/dL group was comparable to that in the 10 ≤ Hb < 12 g/dL group (P = 0.475; Fig. 2B).
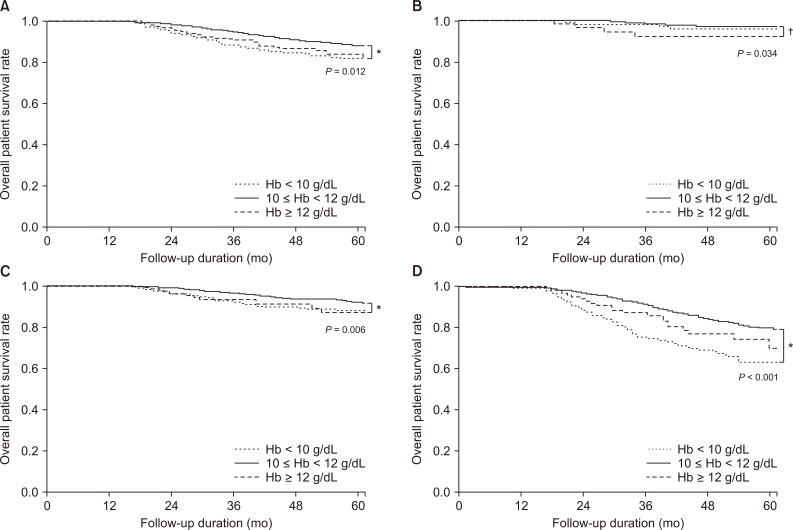
Comparison of patient survival according to patient age.
(A) Survival according to hemoglobin (Hb) concentration in the overall population and in patients (B), under 40 years of age, (C) between 40 to 60 years of age, and (D) over 60 years of age.
*P < 0.05 vs. Hb < 10, †P < 0.05 vs. 10 ≤ Hb < 12.
In a Cox proportional hazards model, for both the 40 ≤ age < 60 years and age ≥ 60 years groups, a lower Hb concentration (Hb < 10 g/dL) was associated with significantly increased risk of all causes of death (adjusted HR, 1.719; 95% CI, 1.158-2.252; P = 0.007 in the 40 ≤ age < 60 years group; and adjusted HR, 2.098; 95% CI, 1.567-2.808; P < 0.001 in the age ≥ 60 years group; Fig. 3B, C), but no such association was found for the age < 40 years group (Fig. 3A).
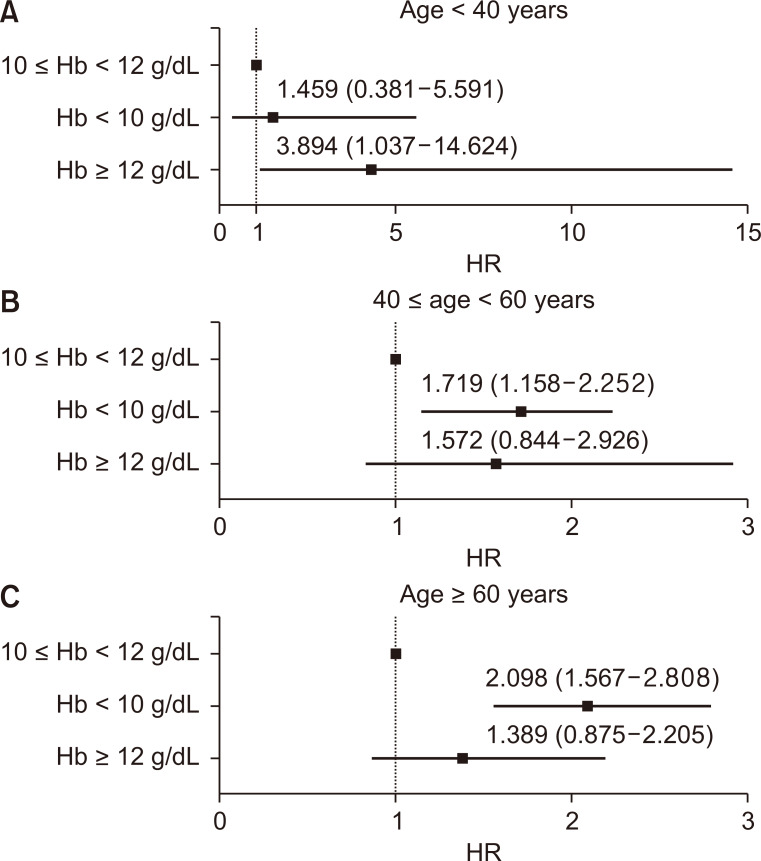
Forest plot of hazard ratios (HR) for overall mortality.
All-cause mortality stratified by hemoglobin (Hb) level for patients (A) under 40 years of age, (B) aged between 40 to 60 years, and (C) over 60 years of age.
Cardiovascular disease (CVD)-related death
A total of 105 cases of CVD-related death occurred during the follow-up period. Among the overall study population, the 10 ≤ Hb < 12 g/dL group had the lowest incidence of CVD-related death (P < 0.001). In the age < 40 years and 40 ≤ age < 60 years groups, the incidence of CVD-related death was not different among the three Hb concentration groups (Fig. 4B, C). In contrast, in the age ≥ 60 years group, the lower Hb group (Hb < 10 g/dL) had the greatest incidence of CVD-related death among the three groups (P < 0.001; Fig. 4D). In the multivariate analyses, after adjustment for sex, primary renal disease, and duration of dialysis, a lower Hb concentration (Hb < 10 g/dL) was an independent risk factor for CVD-related death in the age ≥ 60 years group (adjusted HR, 2.796; 95% CI, 1.669-4.686; P < 0.001; Fig. 5C). The Hb concentration was not significant associated with the incidence of CVD-related death in the age < 40 years and 40 ≤ age < 60 years groups (Fig. 5A, B).
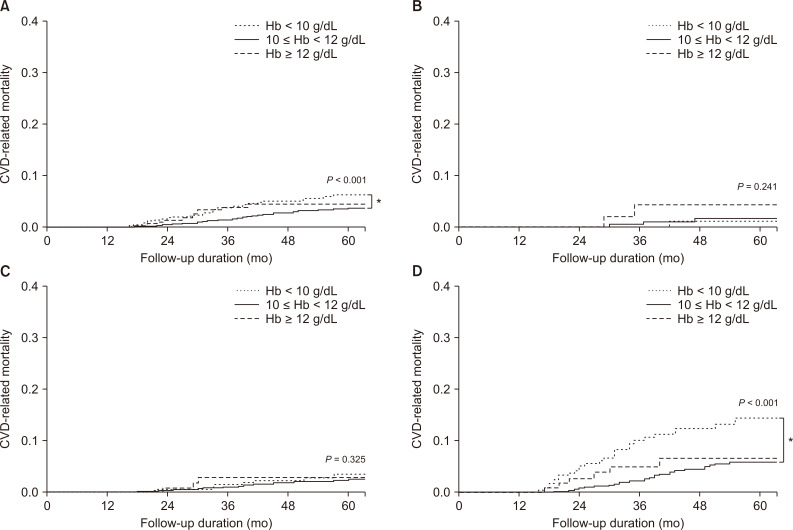
Comparison of cardiovascular disease (CVD)-related death according to patient age.
(A) CVD-related death according to hemoglobin (Hb) concentration in the overall population, (B) in patients under 40 years of age, (C) aged between 40 to 60 years, and (D) over 60 years of age.
*P < 0.05 vs. Hb < 10.

Forest plot of hazard ratios (HR) for cardiovascular disease (CVD)-related mortality.
All-cause mortality stratified by hemoglobin (Hb) level for patients (A) under 40 years of age, (B) between 40 to 60 years of age, and (C) over 60 years of age.
Overall hospitalization and cardiovascular hospitalization
A total of 2,188 (64.2%) patients were hospitalized during the follow-up period. In the overall study population, the Hb < 10 g/dL group had a significantly greater incidence of hospitalization (n = 605, 70.5%) than the 10 ≤ Hb < 12 (n = 1,392, 62.8%) and Hb ≥ 12 g/dL groups (n = 191, 57.0%; P values for all < 0.05). Fig. 6 shows the hazard ratios (HR) of all-cause and CVD-related hospitalization according to patient age and mean Hb concentration, after adjustment for sex, primary renal disease, and duration of dialysis. In the age < 40 years group, there were no significant differences in overall hospitalization according to the mean Hb concentration. However, among the 40 ≤ age < 60 years and age ≥ 60 years groups, Hb < 10 g/dL itself increased the risk of overall hospitalization as compared to 10 < Hb ≤ 12 (adjusted HR, 1.572; 95% CI, 1.213-2.036; P = 0.001, for the 40 ≤ age < 60 years group; adjusted HR, 1.455; 95% CI, 1.037-2.043; P < 0.001, for the age ≥ 60 years group). Among the age < 40 years and 40 ≤ age < 60 years groups, a target Hb ≥ 12 g/dL did not significantly influence CVD-related hospitalization; whereas, among elderly patients (age > 60 years), a target Hb ≥ 12 g/dL significantly reduced the risk of all-cause hospitalization (adjusted HR, 0.544; 95% CI, 0.362-0.820; P = 0.004) and CVD-related hospitalization (adjusted HR, 0.463; 95% CI, 0.242-0.887; P = 0.020).
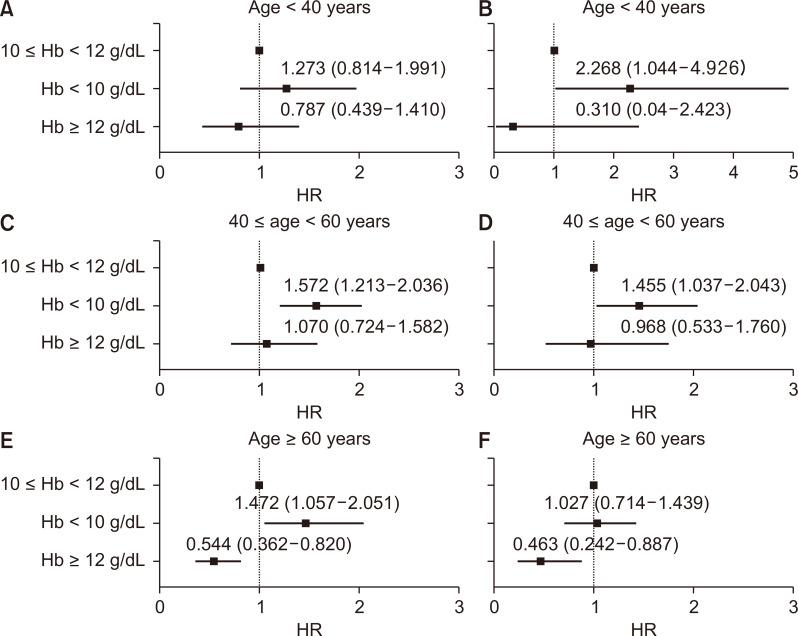
Forest plot of hazard ratios (HR) of (A) all-cause hospitalization and (B) cardiovascular disease (CVD)-related hospitalization of patients under 40 years of age, (C) all-cause hospitalization and (D) CVD-related hospitalization of patients between 40 and 60 years of age, (E) all-cause hospitalization and (F) CVD-related hospitalization of patients over 60 years of age stratified by hemoglobin (Hb) concentration.
Discussion
In this study, we found that overcorrected Hb concentrations or anemia in dialysis patients had differential impacts on the clinical outcomes according to the patient’s age. The impact of anemia was more significant in elderly ESRD patients than in the young patients. In contrast, overcorrected Hb concentrations had more significant impact in the younger ESRD patients. Therefore, our results suggest that a differential approach based on the patient’s age is required for the management of anemia in dialysis patients.
We first compared the baseline characteristics according to the ages of the participants. We divided the patients into three age groups, age < 40, 40 ≤ age < 60, and age ≥ 60. The results of the baseline laboratory study indicated in all three age groups, most patients fell into the 10 ≤ Hb < 12 g/dL group (56% to 69%), followed by the Hb < 10 g/dL and Hb ≥ 12 g/dL groups respectively. Compared to the other age groups, the overcorrection rate was slightly greater in the age < 40 years group with Hb ≥ 12 g/dL, which reflects the tendency to set higher Hb targets for younger patients. However, the serum albumin concentration, which reflects the nutritional status of dialysis patients, did not differ among the three age groups, nor did serum ferritin or TSAT concentrations. Other markers related to anemia, such as iPTH, and C-reactive protein concentrations, also did not differ according to the patient’s age. These findings suggest that the baseline condition associated with anemia may not differ according to the patient’s age.
Next, we investigated the impact of anemia on overall patient survival in each age group. As we expected, patient survival was greatest when the patient’s Hb concentration ranged between 10 and 12 g/dL, in both the overall patient population and each age subgroup. However, anemia (Hb < 10 g/dL) had differential effects on overall patient survival according to the patient’s age: anemia was associated with lower patient survival in elderly patients, but did not influence survival in the younger patient groups. When we compared the incidence of CVD-related death between the young and elderly patients according to their Hb concentrations, the incidence of CVD-related mortality was greater when Hb < 10 g/dL, which indicated that undercorrection of anemia in elderly patients is associated with greater risk of CVD-related deaths. These trends were also confirmed in a review of the multivariate analyses.
This differential impact may be partially accounted for by the association between frailty and anemia in elderly patients [9,10]. In elderly populations, mild anemia is independently associated with an increased risk of frailty, and the poorer prognosis associated with lower Hb concentrations may be related to decreased physical activity [11,12]. The risk of CVD-related death may be attributed to the tissue hypoxia caused by anemia, which promotes left ventricular hypertrophy (LVH), thereby causing death in elderly patients [13]. Previous studies have reported that aging increases the incidence and severity of LVH in dialysis patients. Furthermore, Hb was found to be an age-dependent risk factor for LVH [14]. The effect may be more pronounced in elderly patients, who are vulnerable to LVH [15]. Anemia promotes cardiac structural and functional abnormalities, and is a CVD-related death risk factor in ESRD, especially in elderly dialysis patients [16,17]. Thus, further considerations or investigations are required [18].
Indeed, many previous reports have suggested that the incidence of hospitalization in ESRD patients is associated with a significant decline in Hb [19], and aging and frailty synergistically increased the risk of all-cause and CVD-related hospitalization [20]. Interestingly, among elderly dialysis patients, higher Hb concentrations were associated with significantly reduced risk for all-cause and CVD-related hospitalization, a finding which was seen to be inconsistent with young dialysis patients. This result may suggest that maintaining Hb concentrations within a more physiologically normal range (≥ 12 g/dL) may be adequate for reducing the short-term risk of all-cause and cardiovascular morbidity in elderly HD patients; however, further investigation may be required to clarify this issue and its clinical applications.
Some studies have reported that the effect of anemia on overall or cardiovascular mortality may be less significant in young ESRD patients as compared to elderly ESRD patients, since they have fewer comorbid conditions [21-23]. In addition, the prevalence of CVD among young adults with ESRD is lower than in elderly ESRD patients, and the types of CVD are also considered different. For example, the most common cardiovascular diagnoses in young ESRD patients have been reported to include LVH, congestive heart failure, and arrhythmias, whereas coronary artery disease is most commonly found in elderly ESRD patients [24]. Thus, young ESRD patients do not appear to share the specific cardiovascular risk factors that are commonly present in elderly ESRD patients, and which may contribute to cardiovascular deaths associated with higher Hb concentrations. Therefore, young ESRD patients with may be better able to tolerate elevated Hb concentrations than elderly ESRD patients.
Accordingly, this present study must be understood in the context of the limitations of a large-scale registry analysis, and the possibility of unmeasured confounders. For example, the details of the patients’ type of cardiovascular disease or of comorbidities were not available for analysis. Secondly, the follow-up duration of this registry was relatively short and the death and CVD-related death rarely occurred during this period. Third, this study defined old age as being greater than 60 years of age; however, the cut-off value defining ‘old age’ or ‘elderly’ status may be controversial and may differ from this assessment. Finally, the under 40 years of age group comprised a relatively small proportion of the overall study population, hence, the incidence of overall or CVD-related death may have been underestimated in this age group.
Taken together, anemia had a more significant impact on overall and CVD-related mortality and on the incidence of hospitalization in elderly patients on dialysis in comparison with the relatively young ESRD patients in our study. In contrast, elderly ESRD patients with a Hb concentration ≥ 12 g/dL did not have an increased short-term risk of all-cause mortality. Our results may suggest that more strict management of anemia in ESRD patients may be required in elderly ESRD patients, and also that there is a need for future prospective, randomized trials to identify an appropriate Hb target range to minimize the risk of CVD morbidity and mortality in elderly HD patients.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HC15C1129) and the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT (2018M3A9E802151).
Authors’ contributions
Eun Jeong Ko participated in designing this study and writing the paper. Yong Kyun Kim, Jang-Hee Cho, Yon Su Kim, Shin-Wook Kang, Nam-Ho Kim, and Yong-Lim Kim participated in collecting and analyzing the data. Chul Woo Yang participated in performing the study. Byung Ha Chung participated in designing the study.