



Introduction
Dyslipidemia is one of the most prevalent chronic comorbidities in modern medicine. The critical risk of cardiovascular disease is increased relative to unhealthy lipid profiles, and medications to control dyslipidemia are widely prescribed. Statins, which are HMG-CoA reductase (HMGCR) inhibitors, are the most commonly prescribed types of lipid-lowering agents and have shown solid benefits in reducing the risk of coronary artery disease [1]. In addition, monoclonal antibody inhibitors targeting proprotein convertase subtilisin/kexin type 9 (PCSK9) can lower low-density lipoprotein (LDL) cholesterol level and cardiovascular disease risk and have been recently introduced to the clinic [2,3].
Previous studies have reported conflicting results for the potential kidney effects of lipid-lowering agents, particularly statins. Some considered statins to be prophylactic agents against the risk of postoperative [4] or contrast-induced acute kidney injury [5]. Several observations have indicated that statin usage may help to reduce proteinuria or slow kidney function decline [6–8]. However, the use of HMGCR inhibitors was reported to be associated with risk of acute kidney injury or interstitial nephritis [9–11]. PCSK9 inhibitors showed certain cardiovascular benefits without higher risks of side effects in individuals with kidney function impairment [2,3]. Still, the kidney effect of the medication has yet to be determined, and clinicians are aware of the potential adverse effects of PCSK9 inhibitors, particularly those related to glucose intolerance [12].
As dyslipidemia and kidney function impairment share common metabolic risk factors (e.g., obesity), those who require lipid-lowering medications are frequently at risk of kidney dysfunction. Therefore, the possible kidney effects of drugs such as statins, the most prescribed type, and PCSK9 inhibitors—an emerging drug for which its indication needs to be established—should be investigated. However, complex confounding effects from comorbid metabolic factors and potential healthy user bias are obstacles to such studies. Until long-term evidence from clinical trials is available, Mendelian randomization (MR) studies provide an opportunity to assess the effects of genetically proxied lipid-lowering agents [12]. Previous studies have used the MR approach to assess the potential harm and benefits of lipid-lowering agents, using HMGCR and PCSK9 genetic variants as the genetic instruments [12–14].
In this study, we hypothesized that genetically predicted HMGCR and PCSK9 activities would affect kidney function. We performed MR analysis with genetic variants of the HMGCR and PCSK9 genes and assessed estimated glomerular filtration rate (eGFR) outcomes from large genetic datasets.
Methods
Ethical considerations
The study was approved by the Institutional Review Boards of Seoul National University Hospital (No. E-2203-053-1303) and the UK Biobank Consortium (application No. 53799) [15,16]. The study was performed in accordance with the Declaration of Helsinki. The requirement for informed consent was waived because public databases were analyzed in the study.
Genetic instruments for HMGCR and PCSK9 activity
We used the genetic variants of HMGCR and PCSK9 analyzed by MR in previous studies [12,14]. Briefly, all variants with low linkage disequilibrium, with genome-wide significant (p < 5E-8) association with LDL cholesterol level, and within 100 kB of either of the target genes were identified from the Global Lipids Genetic Consortium study [17]. In that genome-wide association study (GWAS) meta-analysis, the cholesterol levels of 188,578 individuals of European ancestry were assessed after excluding those who were taking lipid-lowering medications. Six single-nucleotide polymorphisms (SNPs) for HMGCR and seven SNPs for PCSK9 were included as the genetic instruments. The effect size betas were scaled and aligned toward a 50 mg/dL “decrease” in LDL cholesterol level, as the study interest was kidney function related to HMGCR inhibition (e.g., statins) and PCSK9 inhibitors along with certain lipid-lowering effects (Supplementary Table 1, available online). We studied the LDL modifying effect of the genetic instruments as LDL is the most common parameter to set dyslipidemia control targets and because of data availability.
Outcome data
The primary outcome summary data were provided by the CKDGen Consortium (https://ckdgen.imbi.uni-freiburg.de/). We used the GWAS meta-analysis summary statistics for the log-transformed creatinine-based eGFR of 1,004,040 European individuals, combining the previous CKDGen and UK Biobank data [18]. The result is one of the largest collections of GWAS meta-analysis summary statistics for kidney function traits and identified genetic architecture related to kidney function. We additionally replicated the findings in each CKDGen phase 4 GWAS meta-analysis dataset and the UK Biobank data as each of the datasets has strengths and weaknesses, and such replication is crucial for a valid genetic analysis. The details of each dataset are described in the Supplementary Methods section (available online) [19–21].
Mendelian randomization analysis and assumptions
MR analysis uses genetic instruments to demonstrate causal estimates [22]. As the genotype of an individual is fixed before birth, genetically predicted exposure is minimally affected by clinical confounders or reverse causation. Thus, genetic randomization in MR provides an opportunity to assess causal effects, and a large-scale genetic dataset is required because genotype explains a portion of the variation in exposure phenotypes. MR analysis has been performed widely in the nephrology field, revealing important causal factors related to kidney function [20,23–25].
MR requires three core assumptions to enable causal inference. The relevance assumption is that the instrument should be strongly associated with the phenotype of interest. As we are using instruments developed from large-scale GWAS meta-analyses, this assumption was considered to be confirmed. Furthermore, we retested the association between polygenic scores for HMGCR and PCSK9 inhibition and LDL cholesterol in the individual-level UK Biobank data. The independence assumption is that genetic instruments should not be associated with confounding phenotypes. In the current study, the instrumented variants were in target genes or in very proximal regions, lowering the possibility of a confounding phenotype than in conventional MR analysis using a large number of genetic variants. Nevertheless, we additionally used pleiotropy-robust MR analysis methods [26]. The exclusion-restriction assumption is that the genetic effects should occur through the exposure of interest. Although statistical confirmation of this assumption is possible, we used pleiotropy-robust MR analysis, and the weighted median method in particular waives this assumption for up to half of instrumented waives, serving as a sensitivity analysis [27].
Summary-level Mendelian randomization analysis
All genetic variants were identified in the outcome datasets. We performed Steiger filtering to ensure the direction of the genetic effects from exposure to outcome phenotype [28]. Next, harmonization of the exposure and outcome data was performed, and palindromic SNPs with intermediate allele frequencies were disregarded [29]. However, the instrumented genetic variants all passed these filters and were used to predict genetically the effects of HMGCR and PCSK9 inhibition. We used multiplicative random-effects inverse variance weighted methods as the main MR analysis, and the weighted median calculation and MR-Egger regression with a bootstrapped standard error were performed (Supplementary Methods section, available online).
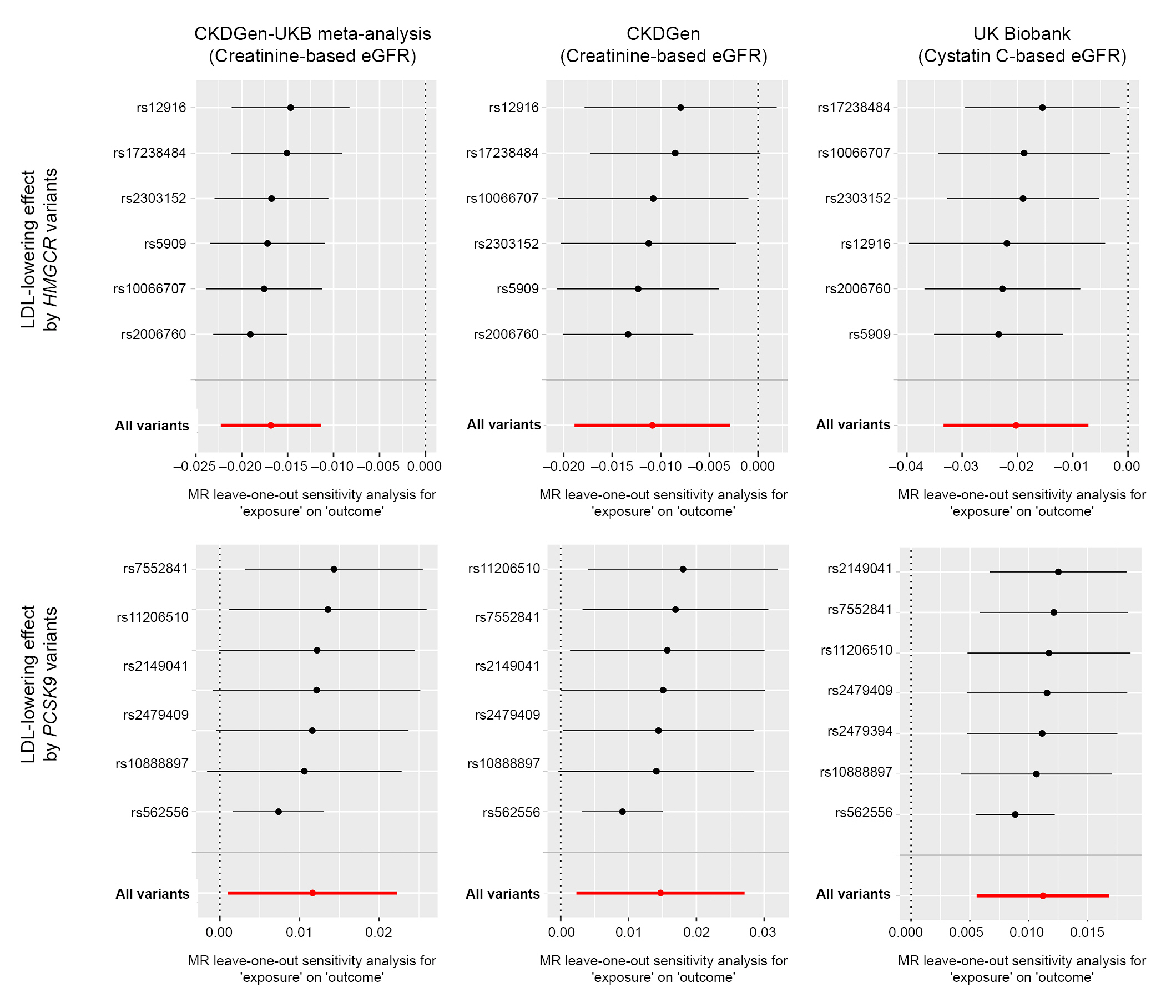
Additional sensitivity analysis was performed by leave-one-out analysis, excluding one SNP at a time, and by single-SNP analysis to assess whether there was a disproportionate effect, potentially pleiotropic, from a single SNP [29].
The summary-level MR analysis was performed using the “TwoSampleMR” package in R (version 0.4.26; R Foundation for Statistical Computing) [30]. To represent the effects of moderate to high-intensity lipid-lowering agents, all causal estimates were scaled to a 50-mg/dL decrease in LDL cholesterol. In addition, as the original outcome GWAS was performed toward log-transformed eGFR values, a raw MR causal estimate was scaled to the exponential change of eGFR, which would be difficult to interpret. Thus, we rescaled the causal estimates to units of % change.
Nonlinear Mendelian randomization analysis with individual-level data
Nonlinear MR analysis is necessary to understand the shape of the cause-effect relationship [31,32]. In nonlinear MR, the population is stratified by instrument-free exposure, and the residual variation in exposure is conditioned for the instruments (e.g., the nongenetic portion of the exposure) because directly dividing the population by exposure phenotype would invalidate MR assumptions. Next, localized causal estimates were calculated according to instrument-free exposure, and meta-regression of the estimates was performed by a fractional polynomial model to estimate the exposure-outcome association. Model degree 1 was selected by statistical calculation to identify the model that better fits the association, and the population strata were set to 100. Allele scores for the LDL levels predicted genetically by HMGCR or PCSK9 gene variants were calculated by PLINK 2.0 by multiplying the gene dosage matrix with the effect size betas of the instruments [33]. The x-axis was aligned and scaled to a continuous mg/dL increase in LDL cholesterol caused by the HMGCR or PCSK9 variant. Age, sex, and 10 genetic principal component-adjusted causal estimates were presented as the main findings. Clinical covariate-adjusted models, additionally adjusted for body mass index, systolic blood pressure, diabetes mellitus, dyslipidemia medication, and hypertension medication, are also presented. The nonlinear MR analysis was performed by the “nlmr” package in R [31].
Results
Characteristics of the outcome data
The CKDGen summary-level data (n = 567,460) included samples from individuals with a median age of 54 years old. Fifty percent of the population was male, the median eGFR was 91.4 mL/min/1.73 m2, and the prevalence of chronic kidney disease (CKD) was 9%. The meta-analyzed UK Biobank dataset, including individuals of European ancestry (n = 436,581), had a mean age of 56.8 years, and 46% of the population was male. The creatinine-based eGFR mean value was 90.5 mL/min/1.73 m2, and the cystatin C-based eGFR mean value was 88.1 mL/min/1.73 m2. The UK Biobank data of individuals of white British ancestry with phenotype information for individual-level nonlinear MR analysis (n = 320,598) showed a mean age of 56.9 years, and 48.7% of the population was male. The mean LDL cholesterol was 138.2 mg/dL with a mean eGFR of 90.4 mL/min/1.73 m2.
Summary-level Mendelian randomization analysis results
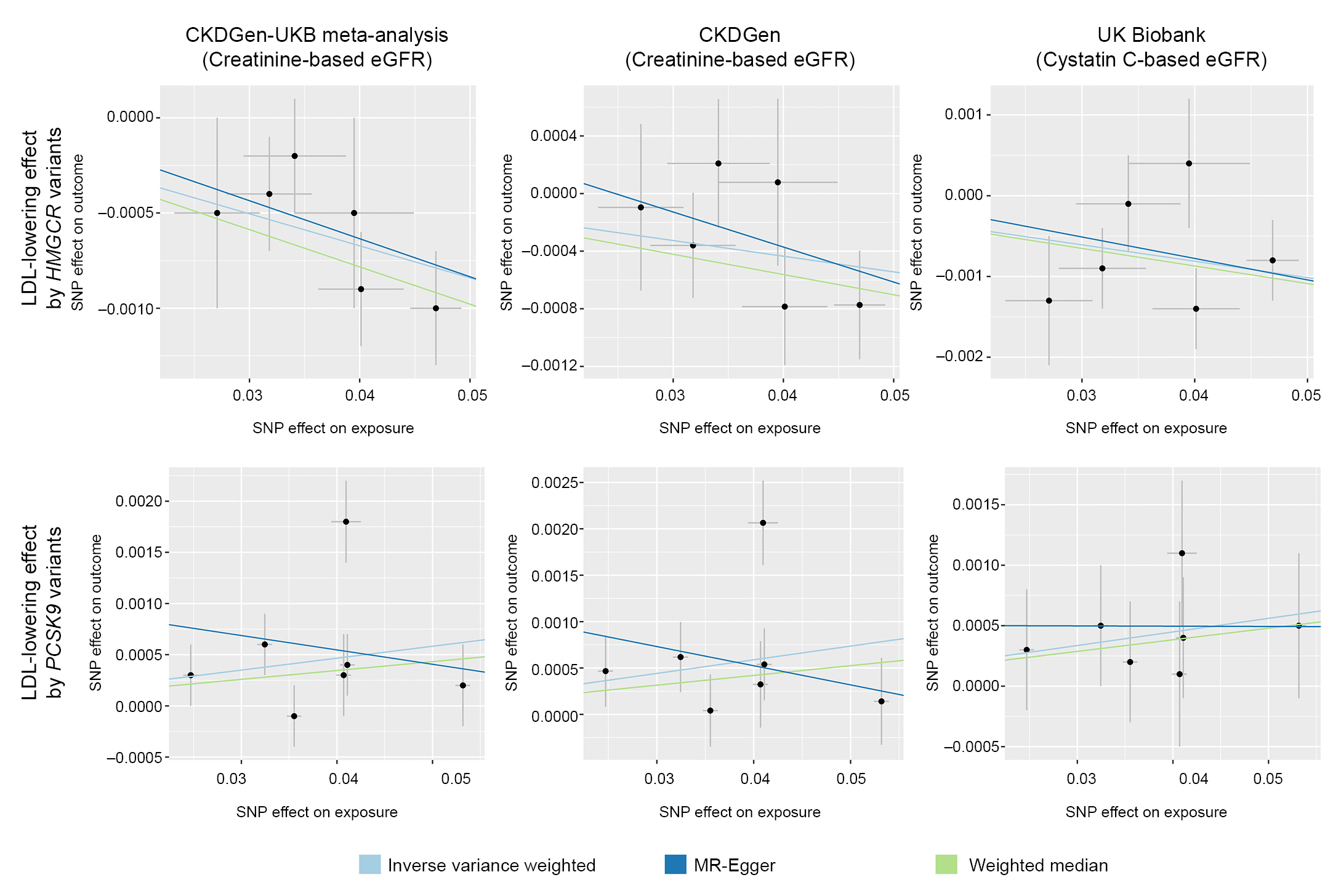
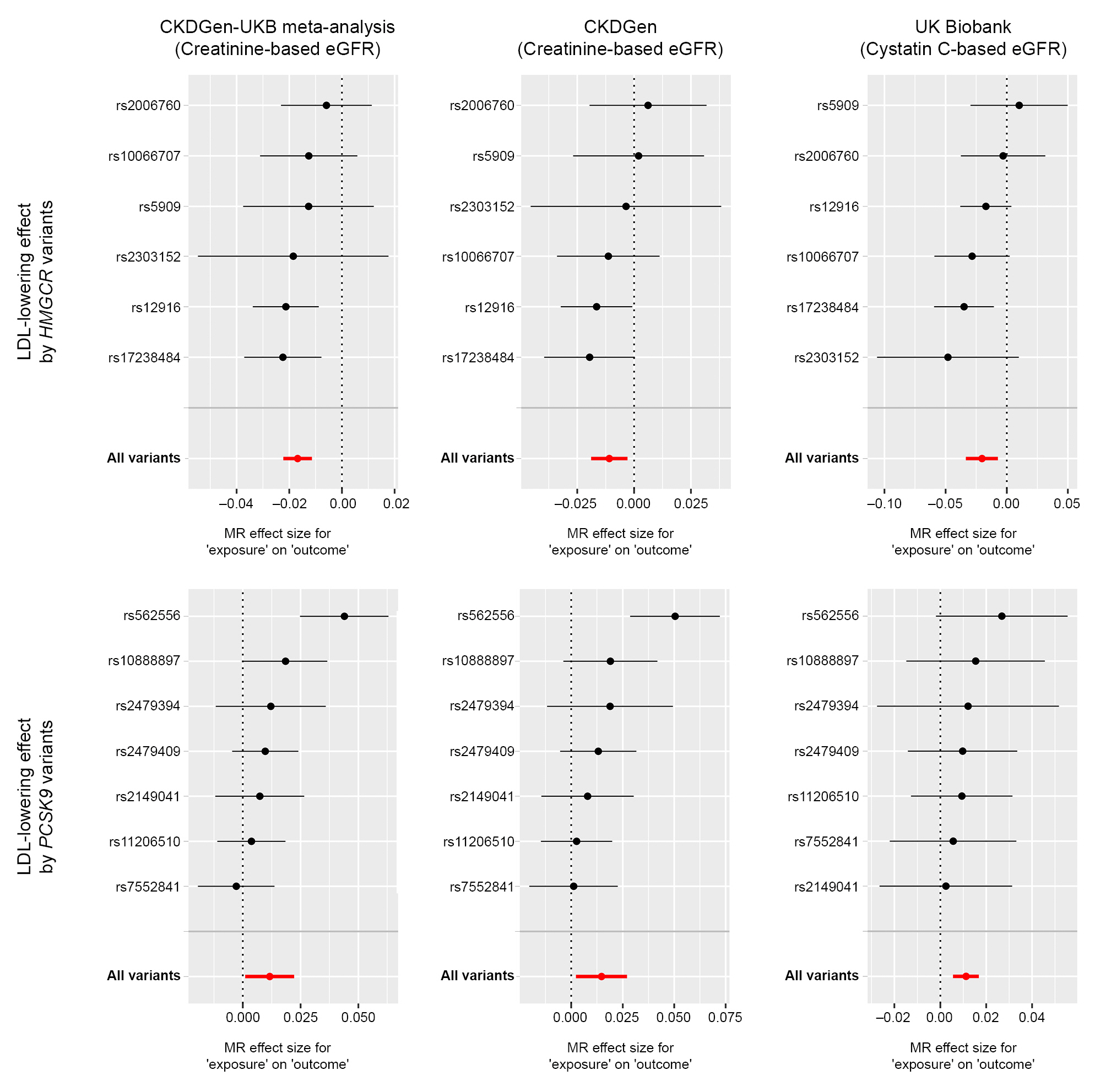
In the main GWAS meta-analysis outcome data, which included >1,000,000 samples from the CKDGen and UK Biobank data, a genetically predicted 50-mg/dL decrease in LDL cholesterol values by modulation of HMGCR was significantly associated with a –1.69% (95% confidence interval [CI], –2.37% to –0.97%) change in eGFR (Table 1, Fig. 1). The causal estimates calculated by the weighted median method and MR-Egger regression were similarly significant, and the MR-Egger intercept (p = 0.34) did not indicate a directional pleiotropic effect. On the other hand, a genetically predicted 50-mg/dL decrease in LDL cholesterol level through PCSK9 inhibition was significantly associated with a 1.17% (95% CI, 0.51%–1.84%) increase in eGFR. The main causal estimates were supported by the weighted median method. Although most variants were identified in the first quadrant, the same positive direction of the effect betas (Fig. 1) indicated a higher eGFR by genetically predicted LDL lowering due to PCSK9 variants, and MR-Egger regression showed nonsignificant results. The MR-Egger intercept p-value supported the main causal estimates by the inverse variance-weighted method in that no significant pleiotropic effects were suspected.
When the analysis was restricted to the CKDGen data, again, a genetically predicted 50-mg/dL decrease in LDL level by HMGCR inhibition was significantly associated with a –1.08% (95% CI, –1.99% to –0.17%) decrease in eGFR. Again, the results were supported by the causal estimates calculated by the weighted median and MR-Egger regression methods. However, the causal estimates from the 50-mg/dL LDL cholesterol level decrease caused by PCSK9 indicated a 1.48% (95% CI, 0.67%–2.30%) increase in creatinine-based eGFR. Again, the weighted median method supported the causal estimates, whereas the CI by MR-Egger regression was wide and in the nonsignificant range, although the MR-Egger regression intercept did not indicate directional pleiotropy.
When we used the UK Biobank data for eGFR based on cystatin C values, the above results were similarly produced. The genetically predicted 50-mg/dL decrease in LDL cholesterol level by HMG-CoA inhibition was significantly associated with a –2.01% (95% CI, –3.19% to –0.81%) change in eGFR, whereas such a lipid-lowering effect by PCSK9 was associated with a 1.13% (95% CI, 0.08%–2.18%) increase in eGFR. The pleiotropy-robust MR sensitivity analysis results supported the main causal estimates from genetic variants of HMGCR genes. On the other hand, when PCSK9 variants were instrumented, the statistical significance was attenuated by the weighted median method with a similar effect size to the causal estimate (0.96%) and by MR-Egger regression, despite the nonsignificant MR-Egger intercept p-value.
Nonlinear Mendelian randomization analysis with individual-level data
In the individual-level data, the genetically predicted inhibition of HMGCR (–15.1 mg/dL; 95% CI, –16.4 to –13.8 mg/dL) or PCSK9 gene activity (–14.1 mg/dL; 95% CI, –15.4 to –12.8 mg/dL) was strongly (p < 1E-16) associated with lower LDL level, identified from the allele-score analyses.
In nonlinear MR (Fig. 4), when the LDL effects predicted by the HMGCR or PCSK gene variants and their association with eGFR were assessed, lower LDL levels predicted by HMGCR gene variants were associated with lower eGFR; in contrast, lower LDL levels predicted by the PCSK9 gene were associated with higher eGFR. The identified association remained similar throughout the range of LDL cholesterol levels, supporting a linear relationship. Similar results were attained even when adjusting for multiple clinical covariates. However, the overall degree of effect was lower for PCSK9 gene variants than for HMGCR gene variants.
Discussion
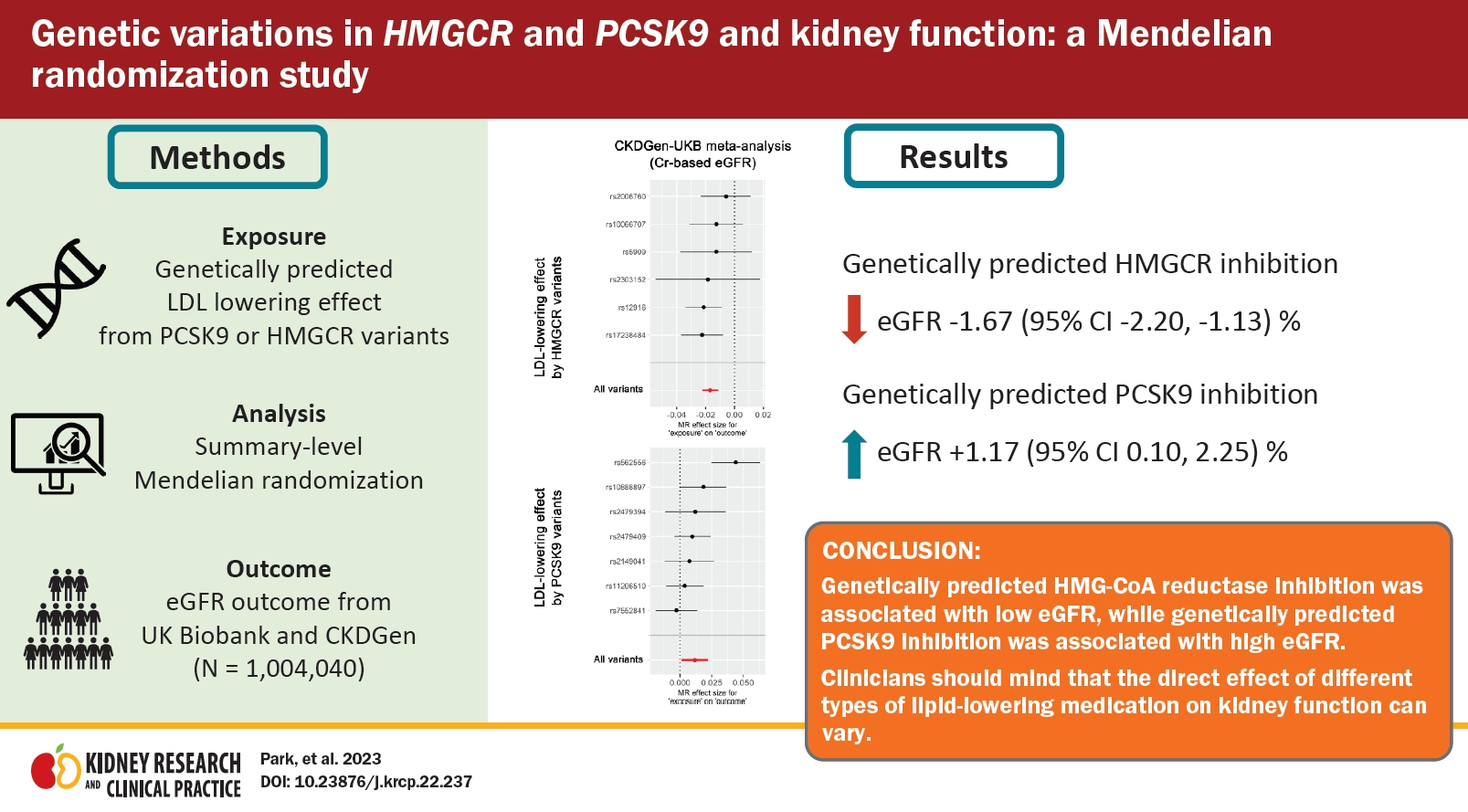
In this MR analysis, we identified significant causal estimates by LDL cholesterol lowering via HMGCR inhibition for lower eGFR. In contrast, genetically predicted LDL cholesterol lowering by PCSK9 inhibition was significantly associated with higher eGFR values. Our study suggests the possibility that the causal effect of different lipid-lowering agents on kidney function may differ according to the molecular target, which warrants further validation for clinical significance.
The direct effect of statins on kidney function remains controversial. Because statins have diverse effects that are not limited to lowering harmful lipid levels, such as anti-inflammatory and plaque-stabilizing effects, some medications can be used to prevent acute kidney injury [4,5]. Additionally, observed statin usage may be associated with proteinuria reduction or a delay in kidney function decline [8]. However, atherosclerotic causes of kidney dysfunction (e.g., renal artery stenosis) are an uncommon etiology of CKD; thus, it is uncertain whether the lipid-lowering effects of statin use may help directly in preventing kidney function impairment [34]. In addition, statin use is associated with certain side effects, including rhabdomyolysis and interstitial nephritis, which may cause kidney injury, leading to debate about observational results that indicate a higher risk of CKD or acute kidney injury related to statin use [9–11]. However, as confounding effects and reverse causation are inevitable in observational studies, additional studies are warranted to investigate the causal effects of statin usage on kidney function.
Recently, an MR study utilizing HMGCR genetic variants reported that statin use may cause kidney failure, yet as the outcome phenotype was determined based only on diagnostic codes, additional evaluation of the most widely used kidney function parameter, eGFR, was warranted [35]. In this study, we performed MR analysis investigating this issue utilizing HMGCR genetic variants and demonstrated that the lipid-lowering effect of HMGCR inhibition may be related to a decrease in eGFR. The results were also significant in the pleiotropy-robust MR sensitivity analysis; thus, our study suggests a negative effect on eGFR from lipid lowering by HMGCR inhibition.
However, this study does not discourage the use of HMGCR inhibitors for cardioprotective purposes, even for those who are at risk of kidney function impairment or who have established CKD [36]. Specifically, the overall effect size from the lifelong 50-mg/dL LDL-lowering effect, which would be achieved with moderate- to high-intensity statin use, was small (1%–2%) compared to the prominent benefits for cardiovascular disease by these drugs. In addition, we looked at the LDL-lowering effect signals of the HMGCR variants on kidney function measured in stable clinical conditions; thus, pleiotropic effects (e.g., anti-inflammation) or effects on acute kidney injury could not be assessed herein. Thus, this study encourages clinicians to monitor kidney function when prescribing statins. Additionally, clinicians may consider carefully determined dosing schedules of statins for such individuals, along with consideration of the potential side effects that may affect kidney function.
Regarding the kidney effects from PCSK9 inhibition, the ODYSSEY trial and FOURIER trial identified nonsignificant differences in eGFR values related to PCSK9 inhibition compared to placebo [2,3]. In this MR study, eGFR was estimated to increase with the LDL-lowering activity from PCSK9 inhibition, as genetically predicted LDL lowering by PCSK9 variants was significantly associated with high eGFR. Yet, even from the lifelong genetic effect was tested, the overall effect size was small, showing that such small differences might not have been evident in the clinical trial results. Furthermore, debates regarding the interpretation of the results for pleiotropy-robust MR sensitivity analysis may remain. As the weighted median method supported the results in the CKDGen-UK Biobank meta-analysis dataset and CKDGen data, the nonsignificant MR-Egger regression finding can be due to the low statistical power of the method, particularly since we utilized a relatively low number of SNPs [37]. This can also be supported by the nonsignificant MR-Egger intercept p-values, which indicates the absence of directional pleiotropy; thus, the causal estimates can be interpreted to support that LDL-lowering PCSK9 inhibition may increase eGFR. On the other hand, as the findings from the weighted median and MR-Egger regression methods were both nonsignificant for the UK Biobank data using cystatin C-based eGFR as the outcome, some may point out the limitation of the sample overlap in the CKDGen data and that the possibility of a pleiotropic effect cannot be disregarded. Together with the findings from previous trials, the current study could suggest the possibility that the direct effect on eGFR by PCSK9 inhibition may be different from that of HMGCR inhibition with a small effect size; however, the mechanism and direction cannot be confirmed herein.
This study has several limitations. First, although MR tests the lifelong effects of genetically predicted exposure, the degrees of the effect size was relatively small. In addition to MR having a limited ability to suggest the usefulness of related clinical intervention, the interpretation of the results should be carefully performed in real-world clinics [38,39]. Second, although genetic variants can be proxies of a medication effect, it should be noted that drug subtypes may have different mechanisms. In particular, monoclonal antibodies that bind to extracellular PCSK9 may not have the same effect as PCSK9 variants related to lipid levels. In addition, the effects from modulation of other types of cholesterols (e.g., triglycerides) were not tested in the current study. Therefore, the clinical utility of the current results should be additionally supported by real-world data. Third, MR analysis is based on some untestable assumptions. As subgroup analysis causes collider bias in MR, violating the untestable assumption for random allocation of genotypes, the effect of LDL modulation by PCSK9 or HMGCR inhibition in those with profound kidney function impairment could not be tested by the current study. Last, the genetic analysis of this study was restricted to populations with European ethnicity; thus, the generalizability of the results is limited.
In conclusion, genetically predicted HMGCR inhibition was associated with a low eGFR, whereas genetically predicted PCSK9 inhibition was associated with a high eGFR in large genetic databases. Clinicians should consider that the direct effect of different lipid-lowering medication types on kidney function can be different.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









