



Introduction
Globally, the prevalence of end-stage kidney disease (ESKD) is increasing [1], with Taiwan having the highest prevalence in the world. Also, in Taiwan, 3,317 patients per million people received dialysis in 2015, and the prevalence of dialysis, regardless of ESKD, was 3,679 patients per million in 2019. The incidence rate of dialysis has also increased from 331 per million people in 2000 to 529 per million people in 2019 [2,3].
Despite preventive guidelines and clinical measures, however, the maintenance of vascular access for hemodialysis remains a significant challenge. Restoring vascular access remains the leading medical procedure in patients undergoing maintenance hemodialysis [4,5]. Loss of vascular access patency for both arteriovenous fistula (AVF) and arteriovenous graft (AVG) is associated with inadequate dialysis, morbidity, and mortality [6ŌĆō8]. Therefore, preventing complications might lower morbidity rates, improve quality of life, and reduce the cost of health care in the dialysis population. The primary patency rate reported in a meta-analysis consisting of 46 articles was 60% (95% CI, 56%ŌĆō64%) among 4,111 AVF cases (13 studies/21 cohorts) at 1 year and 51% (95% CI, 44%ŌĆō58%) among 2,694 AVF cases (seven studies/12 cohorts) at 2 years [9]. Findings from the Dialysis Outcomes and Practice Patterns Study reported the primary AVF patency rates for patients from Europe/Australia/New Zealand and Japan to be 51% and 72% at 1 year and each 40% to 60% at 2 years [10]. In a study using a national database in Taiwan, the primary patency rates, from creation of AVF to intervention, were 55.4% and 40.8% at 1 and 2 years, respectively, while the primary patency rates of AVG were 33.4% and 13.7% at 1 and 2 years [11].
Clinical practice guidelines for vascular access recommend increased use of autogenous AVFs and the prevention of access dysfunction with surveillance and preemptive intervention [12]. To improve patient quality of life and care, the 2006 Kidney Disease Outcome Quality Initiative (K/DOQI) has recommended either clinical monitoring or routine vascular access flow surveillance for early identification of potential vascular access problems, allowing for timely intervention of access dysfunction. Vascular interventions are recommended when vascular access flow becomes <600ŌĆēmL/min in grafts, <400ŌĆō500ŌĆēmL/min in fistulae, decreases by 25%, or decreases to <1,000ŌĆēmL/min over a 4-month period [12]. However, no clear consensus has been reached regarding optimal surveillance to identify a failing access route [13]. Subsequently, the 2019 K/DOQI guideline placed less emphasis on routine surveillance due to insufficient evidence to make a recommendation for surveillance in addition to routine clinical monitoring [14].
From our experience, supplementary routine surveillance provides an objective assessment for actively identifying potential vascular access problems at an early stage in hospital settings [8,15]. However, whether this would also benefit dialysis clinics is not known. In general, in Taiwanese patients who attend dialysis clinics (as opposed to hospital dialysis centers) for hemodialysis have few comorbidities, are stable, and have stable or no severe medical conditions [3]. For this reason, these dialysis clinics usually do not have surveillance equipment or certified technicians to perform regular tracking of vascular access flow rate (Qa), and they are also not able to perform vascular intervention even when problems are detected with clinical monitoring. Collaborative networks to support dialysis clinics with resources from hospital dialysis access management centers are critical for timely identification and intervention of potential vascular access problems, such as stenosis and thrombosis, in hemodialysis patients [16]. Our hospital-based dialysis access management center (Dialysis Access Management Center in Shin Kong Wu Ho-Su Memorial Hospital [SKH]) began to cooperate with regional dialysis clinics in 2018 to implement vascular access clinical monitoring and supplementary surveillance programs. Services provided included evaluation protocols for potential vascular access risk identification, which, once detected, facilitated the timely referral of patients to the dialysis access management center for further evaluation and/or intervention if necessary.
The aim of this investigation was to examine the effect of this collaborative program involving supplementary routine surveillance on the prognosis of vascular access in dialysis clinics and satisfaction rates from the participating clinics. The goal was to bridge the current system deficiencies to improve quality of care, patient navigation, and interprofessional collaboration. It was hypothesized that this collaborative model could improve the quality of care for patients with dialysis through early evaluation of vascular access problems with supplementary surveillance and enhance the quality of care at dialysis clinics.
Methods
Study design
This retrospective observational study was performed at six nonŌĆōhospital-based dialysis clinics as part of a collaborative program with a hospital-based dialysis access management center (Dialysis Access Management Center in SSKH) between January 2019 and December 2020. In addition to clinical monitoring as per the 2019 K/DOQI clinical practice guidelines, the Qa was measured by ultrasound dilution. Vascular access flow surveillance was performed every 3 months during the study period. The incidence of preemptive intervention and vascular access failure due to thrombotic occlusive events within both periods (including needing to perform percutaneous transluminal angioplasty [PTA], new AVG creation, or AVG creation) was recorded to determine the effect of the access flow-based collaborative program. A total of 392 hemodialysis patients with vascular access (AVF, n = 339 and AVG, n = 53) were included.
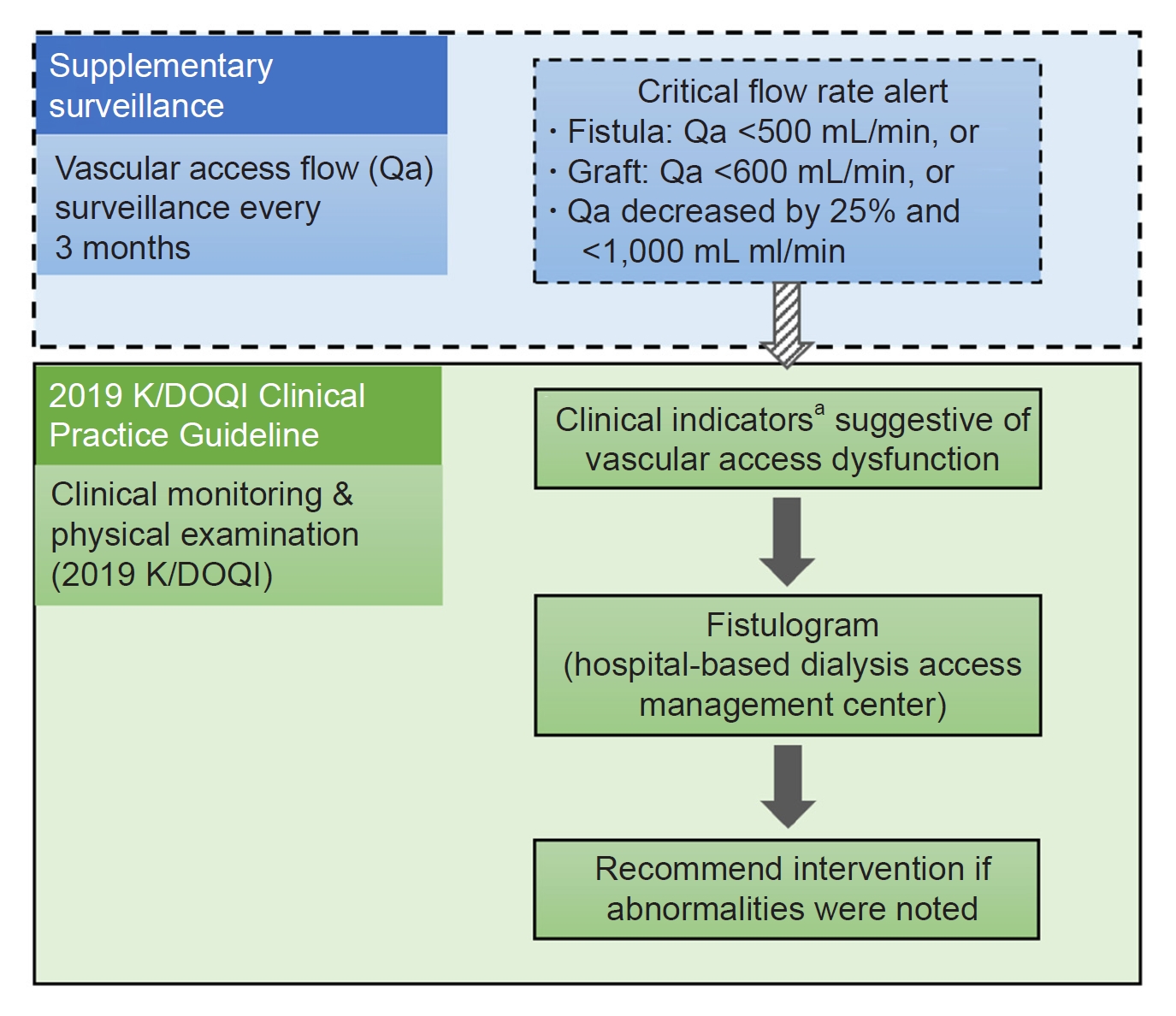
A fistulogram to evaluate the need for vascular interventions was recommended to patients with clinical indicators suggestive of dysfunction. In the event of a critical flow problem detected by surveillance (e.g., low-vascular access flow or a substantial flow decline based on the following definition adopted from K/DOQI clinical practice guidelines for vascular access), clinical indicators suggestive of dysfunction also needed to be present before scheduling a fistulogram to further evaluate the need for vascular intervention.
Outcome parameters and definitions
The main outcome measures included prognosis of vascular access in clinic dialysis patients (i.e., vascular access flow, incidence of critical flow, vascular access reconstruction rate, and vascular access balloon dilatation rate), satisfaction of the dialysis clinic with the collaborative model, and the referral rate to the surveillance program provider (i.e., the hospital-based dialysis access management center).
The incidence of critical flow events was defined as: event ratio = number of critical flow events / number of flow records. Vascular access flow problem was defined as having critical Qa of <600ŌĆēmL/min in grafts and <500ŌĆēmL/min in fistulae, or Qa declined by >25% and falls below 1,000ŌĆēmL/min over a 3-month period (Fig. 1).
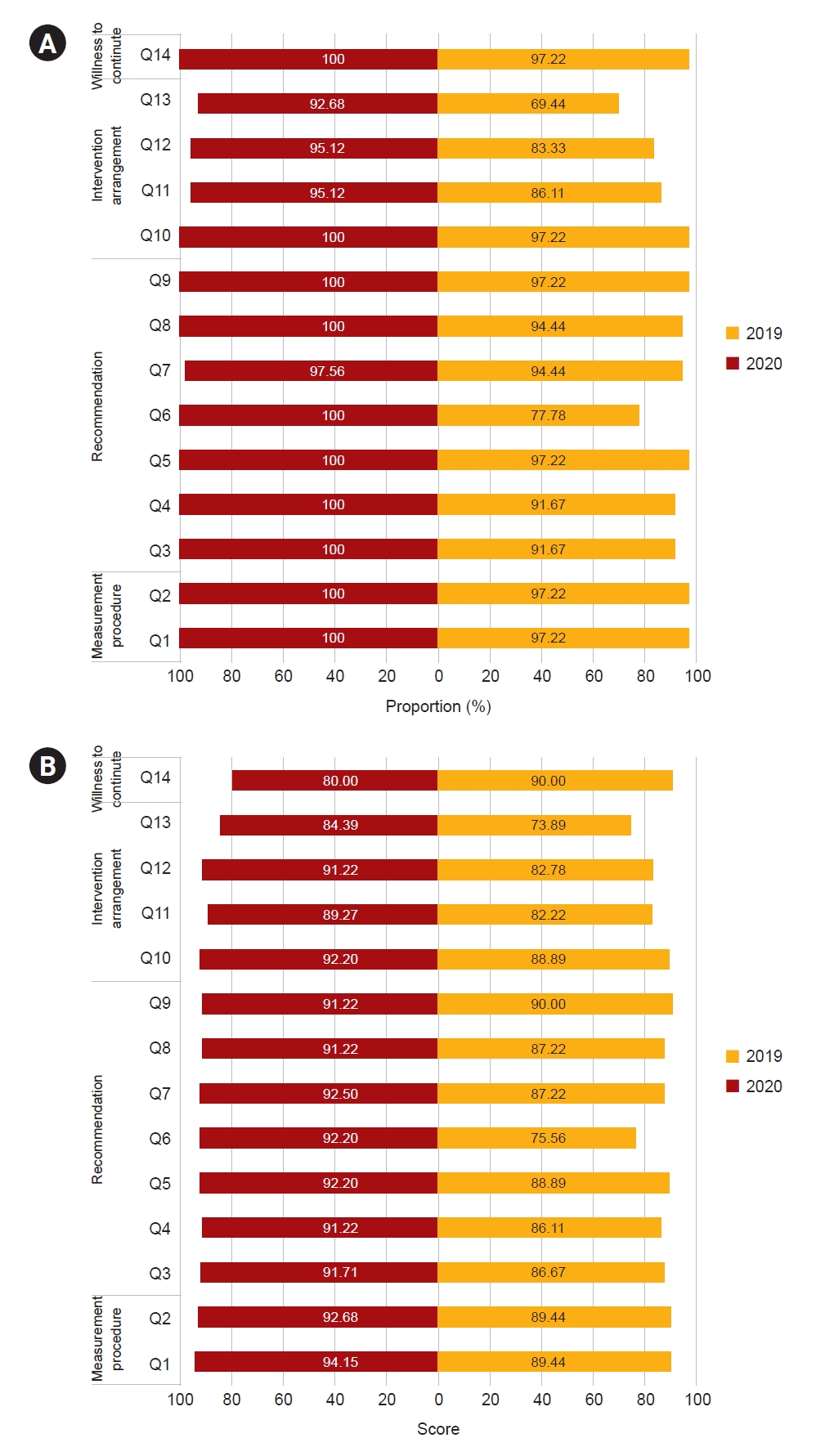
The collaborating dialysis clinics were asked to complete a 5-point Likert satisfaction survey at the end of both 2019 and 2020. The survey consisted of 14 questions grouped into four categories, as follows: 1) satisfaction with the instructions provided regarding the measurement procedure; 2) satisfaction with the recommended critical flow criteria; 3) satisfaction of intervention planning upon identification of a critical flow problem; and 4) willingness to continue with the collaboration program (Supplementary Table 1, available online).
Access flow measurements by ultrasound dilution technique
The access flow measurement technique involves reversing the access lines during dialysis and using the ultrasound dilution methodology, as introduced by Krivitski [17], to measure the resulting fraction of recirculated blood entering the dialyzer. Vascular access flow was measured by a certified technician. A dilution ultrasound exam was performed during dialysis on the same day, in the first hours of dialysis. Qa was calculated using the formula as follows: Qa = Qb ├Ś ([1 ŌłÆ R]/R), where Qb is the extracorporeal pump pressure and R is the fraction of recirculated blood.
Statistical analysis
Nonparametric continuous variables are presented as median and interquartile range values and tested with the Mann-Whitney U test. Parametric continuous variables are presented as mean and standard deviation values and tested with the t test for normal distribution. Categorical variables are presented as counts and percentages and tested with the chi-square test. The significance level was set at two-sided p-value of <0.05. All statistical analyses were performed using SAS version 9.4 (Windows NT version; SAS Institute, Inc.).
Ethical considerations
This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of SKH Memorial Hospital (no. 20170921R). Informed consent was waived by the same committee in view of the retrospective nature of the study and the fact that all procedures being performed were part of routine care.
Results
Improved quality of patient care
A total of 392 patients from the five participating dialysis clinics (clinics AŌĆōE) were enrolled into this study (including 339 patients with AVF and 53 patients with AVG). Baseline patient demographics are reported in Table 1. The demographics for individual clinics are reported in Supplementary Table 2 (available online). The median age was similar between groups (65 years for AVF patients vs. 67 years for AVG patients). There were statistically significant increases in the median systolic blood pressure and median diastolic blood pressure in the AVF group compared to the AVG group (p < 0.05). There was also a statistically significant greater proportion of women in the AVF group (p = 0.001).
The overall ratio of critical flow events significantly decreased from the first year to the second year of surveillance in the AVF group (18.3% vs. 12.7%, p < 0.001) (Table 2). A similar trend was demonstrated in critical flow events in the AVG group (26.2% vs. 20.1%, p = 0.30). Increased vascular access flow from the first-year surveillance period to the second-year surveillance period was observed in both the AVF and AVG groups, respectively, although the difference was not significant (Table 2).
Clinical outcomes associated with participation in the collaborative program are shown in Table 2. The number of PTA events decreased in both groups over the 2-year surveillance period, with a significant decline observed in the AVG group (0.77 per person-year vs. 0.51 per person-year, p = 0.005). The number of new AVF or AVG creations was similar between groups and remained low over time.
Clinician satisfaction
Pooled results from the satisfaction with collaboration survey from the five participating nonŌĆōhospital-based dialysis clinics are shown in Fig. 2. A total of 35 medical personnel, including attending physicians, nurses, and certified dialysis technicians, replied to the satisfaction survey. At least three surveys were obtained from each of the clinics. Overall, dialysis clinics were satisfied with the collaborative program. The satisfaction rate increased from the first year of surveillance to the second year in all domains, including in the guidelines given for measurement procedures, the recommended critical flow criteria, the arrangement of subsequent evaluations, and intervention upon identification of critical flow problems. The rate of willingness to continue with the collaboration program was 100% by the end of the second year.
Enhanced interprofessional collaboration
The overall hospital referral rate (SKH) from the five participating clinics increased from year 1 to year 2 (65.7% vs. 72.0%). The referral rate was not directly associated with the physical distance between the nonŌĆōhospital-based dialysis clinics and the participating hospital (Fig. 3; Supplementary Table 3, available online).
Discussion
Vascular access is critical for patients undergoing dialysis. Failure to obtain vascular access is associated with morbidity, discomfort, inconvenience, and increased costs [18]. In this study, we reported outcomes following the implementation of an integrated collaborative model for care and treatment of vascular access issues in hemodialysis patients based on clinical monitoring and supplementary access flow surveillance. We demonstrated an overall increase in the Qa, a decline in critical vascular flow events, and a reduction in both the number of PTA interventions and new AVG and AVF creations. The strength of this program is its introduction of supplementary routine surveillance to dialysis clinics. To the best of our knowledge, this is the first study to report outcomes like these from this type of collaborative model.
The implementation of access surveillance in dialysis clinics aims to detect problems at an early stage. Unfortunately, this type of program is problematic for many dialysis clinics for several reasons, including a lack of surveillance equipment due to cost; a lack of certified technicians to perform regular tracking of vascular access; and an inability to perform vascular intervention at some local dialysis clinics, even when access flow problems are detected (such as in Taiwan). Ozgen and Ozcan [16], in reaction to findings from a study that examined facility characteristics, commented that most facilities are functioning technically inefficiently. Interestingly, technical efficiency was significantly associated with the type of ownership.
Our study demonstrated that, by providing detailed guidance on criteria for identifying critical vascular access problems and having medical center support for the early evaluation of potential vascular access dysfunction, the quality of vascular access was improved (thus achieving the standard recommended by KDOQI guidelines). We reported that the number of PTAs was significantly decreased in the AVG group, while the number of new AVF and AVG creation events was maintained at low levels during the collaboration period (0.006 per patient-year in the AVF group; 0.057 per patient-year in the AVG group).
In Taiwan, the hemodialysis quality guidelines recommend the vascular access reconstruction rate to be monitored every 6 months and to be lower than 1.1 times the average rate of the previous 3 years. The ratio of vascular access reconstruction, as indicated in an annual report of kidney disease, was 1 to 2 cases per 1,000 patient-months from 2010 to 2014 [19]. By the end of 2019, the upper limit of the inter-hospital reconstruction rate (defined as the total number of patients who need re-creation of AVF or AVG per 100 total patient-months) was Ōēż0.49, while the upper limit of fistula reconstruction was Ōēż0.13 in the same hospital [20]. If the reconstruction rate of medical facilities exceeds the upper limit, a portion of the hemodialysis reimbursement may be deducted by the National Health Insurance in Taiwan.
Team-based interprofessional collaboration is warranted because vascular access care is a multistep process with different providers involved at different levels of care [21]. Our collaborative model supports the team-based approach and demonstrated improved vascular access outcomes. By providing coordinated care that includes a dialysis access management specialty center, interprofessional communication was improved, which facilitated early identification of potential vascular access problems, such as stenosis and thrombosis, in hemodialysis patients [22ŌĆō24]. As noted by Murea and Woo [22] in 2021, a fragmented approach to hemodialysis patient care has, unfortunately, been the norm. Going forward, dialysis clinics, which are usually isolated in health care settings, should shift toward a patient-tailored care approach. In our current study, the satisfaction of the collaborating dialysis clinics was demonstrated by the results of the satisfaction survey, and during the collaboration period, there was also an increase in referrals to SKH for vascular access evaluation and intervention, regardless of the distance needed to travel. This indicates that both patients and dialysis clinics have gained more trust with the collaborating hospital and that the collaborative model has provided a system of support to improve the quality of care, patient navigation, and interprofessional collaboration.
There are several limitations associated with this study. First, because patient medical histories and data about vascular access before collaboration were not available, the heterogeneity in the health status of the study group was not considered. Vascular access outcomes may be affected by comorbidities, dialysis duration, and cause of end-stage renal disease. Second, because all dialysis patients in the participating clinics joined our collaborative program at the same time, this study lacked a control group. Future prospective studies should be designed to compare vascular flow and critical events between participants with or without collaborative surveillance to rule out possible confounding factors. Third, this study did not investigate the cost-effectiveness of an access flow-based surveillance program; however, previous studies have demonstrated the cost-effectiveness of such a program. In their study, McCarley et al. [25] reported a reduction in thrombosis rates in both AVG and AVF patients, which improved patient comfort and health care costs, and Wijnen et al. [26] reported that quality improvement programs, based on periodic access flow measurements, reduced the number of acute vascular access failures due to thrombotic events and also significantly reduced health care costs in patients with AVG.
This study demonstrates the success of a collaborative model between dialysis clinics and a hospital center for improving the quality of vascular access care and intervention. The strength of this program is its introduction of supplementary routine surveillance to dialysis clinics, which can be used as a model for other hospitals and their management of dialysis patients with vascular access. Establishing an integrated collaborative model for vascular access care and treatment between dialysis clinics and referral hospitals can alleviate some of the current difficulties encountered by dialysis clinics when caring for patients with a vascular access route. Importantly, a satisfactory prognosis of the vascular access for dialysis patients can be maintained with a collaborative program. The establishment of trust between patients, dialysis clinics, and partner referral hospitals benefits all stakeholders and encourages referrals to the partner hospitals. Pursuing this ŌĆ£triple winŌĆØ situation between patients, local dialysis clinics, and partner specialist hospital centers should be considered in other regions.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









