



Introduction
The incidence and prevalence of diabetes mellitus are on the rise in most countries. Globally, approximately one in 10 adults have diabetes, and the International Diabetes Federation has estimated that over 700 million people will have diabetes by 2045 [1]. Patients with type 1 diabetes (T1D) or type 2 diabetes (T2D), as well as diabetes secondary to various metabolic disorders or associated with systemic corticosteroid use, can develop kidney disease, with T2D accounting for the bulk of the disease burden. As many as 25% to 40% of all patients with diabetes will develop kidney problems after 25 years of diabetes, especially those with T2D, thus rendering diabetes the leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) worldwide [2]. Consequently, in the context of the so-called “diabetes pandemic,” effective therapies for diabetic kidney disease (DKD) and its associated complications will greatly impact health outcomes for many people worldwide.
In recent years, a lower risk of ESKD in patients with T1D has been reported in many countries. Furthermore, when ESKD does occur in T1D, it appears to occur at an older age [3]. It has been suggested that a combination of treatment strategies including optimized glucose control, blood pressure (BP) management, and the use of renin-angiotensin system (RAS) inhibitors (RASi) likely explain these encouraging data in T1D, a goal not yet achieved in T2D.
This paper aims to present an updated review of DKD and its current therapeutic strategies. Momentous strides in pharmacological therapy have been made in recent years, particularly for T2D patients with DKD, though there remains significant residual cardiovascular (CV) and kidney risks. Important ongoing challenges that clinicians confront in the care of these patients will be highlighted.
Diagnosis and pathogenesis of diabetic kidney disease
The term DKD refers to a presumptive diagnosis of CKD caused by diabetes. Diabetic glomerulosclerosis, on the other hand, is a histopathologic descriptor, used to describe the characteristic findings of an increased mesangial substrate, nodular lesions, and tubulointerstitial fibrosis on kidney biopsies.
The pathogenesis of DKD is complex and incompletely understood. Critical metabolic changes, along with genetic and epigenetic factors, glomerular hypertension and hyperfiltration, upregulation of the renin-angiotensin-aldosterone system (RAAS), accumulation of advanced glycation end products (AGEs), oxidative stress, kidney inflammation, and fibrosis, are believed to contribute to the initiation and progression of the disease. Abnormal urinary albumin excretion (UAE) precedes impaired renal function in many, though not in all patients with DKD. Particularly in T2D, it is increasingly recognized that a substantial proportion of patients have a progressive loss of renal function without significant albuminuria [4]. The putative mechanism for the loss of renal function is unclear. Renal vascular disease, hypertension, interstitial inflammation, and fibrosis may all be reasonable contributions to the functional decline of kidneys in diabetes. Therefore, DKD represents a broad term that encompasses a spectrum of vascular, glomerular, and tubulointerstitial components of CKD attributed to diabetes. This heterogeneity in patients recruited in randomized clinical trials (RCT) represents an important limitation in studies of DKD, as the efficacy of a drug will likely vary in patients with different manifestations of the disease.
Most patients with diabetes do not need a kidney biopsy to establish the presumptive diagnosis of DKD, because the diagnosis can usually be made in patients presenting with a classic finding of elevated UAE and diabetes duration greater than 7 to 10 years. However, maintaining suspicion for non-DKD is essential, especially in patients with atypical features. These may include the absence of retinopathy or albuminuria developing <5 years after the onset of diabetes in T1D, the sudden onset of severe proteinuria, rapid kidney function deterioration, active urinary sediment, serologic findings, or other concurrent systemic diseases. An estimated glomerular filtration rate (eGFR) loss of greater than 1 mL/min/mo in a patient with good glycemic and BP control may also suggest an alternate cause of CKD and a need for a kidney biopsy. In general, there is a high prevalence of non-DKD in retrospective studies of biopsies from patients with T2D, although selection bias is inherent in these studies because these patients often have atypical clinical features [5].
Both the level of albuminuria and eGFR have independent predictive importance for progression to ESKD and CV morbidity and mortality, although neither is specific to DKD. Despite an ongoing quest to find novel biomarkers to identify early-stage DKD and to improve risk stratification, none is yet available for clinical application. Patients with a consistent finding of severely elevated albuminuria (urine albumin/creatinine ratio of >300 mg/g) have an elevated risk of rapid progression and should be referred to a nephrologist for evaluation even if eGFR is normal or mildly decreased.
Extrarenal microvascular and macrovascular disease
The presence of DKD is often associated with extrarenal manifestations of microvascular disease and macrovascular disease. In T1D, DKD and diabetic retinopathy are highly concordant, whereas only 50% to 60% of T2D patients with DKD have retinopathy [6]. Other diabetic complications, including sensory and autonomic polyneuropathy, gastroparesis, and vascular diseases involving coronary, cerebral, and peripheral vasculature, frequently coexist with DKD.
Although progressing to ESKD is consequential, a greater concern is that patients with DKD are more likely to die from nonrenal causes than to survive long enough to contend with ESKD [7]. As glomerular filtration rate (GFR) declines, both kidney and non-kidney complications develop. Anemia and disorders of bone mineral metabolism develop earlier in patients with DKD compared with patients with nondiabetic CKD and comparable eGFR [8]. Importantly, the risk of death from cardiovascular disease (CVD) or infection is significantly elevated. Therefore, it is critical to consider extrarenal risks in the care of patients with DKD.
Since 2008, the U.S. Food and Drug Administration mandated that new therapies seeking approval for the treatment of diabetes must show CV safety. Greater attention is now focused on clinically pertinent endpoints such as major adverse cardiovascular events (MACE), major adverse renal events (MARE), and all-cause mortality in the development and testing of novel therapeutic agents for diabetes mellitus. Indeed, the novel study designs for sodium-glucose cotransporter-2 inhibitors (SGLT2i), glucagon-like peptide-1 receptor agonists (GLP-1 RA), dipeptidyl peptidase-4 inhibitors (DPP4i), and the nonsteroidal mineralocorticoid receptor antagonist (MRA) finerenone resulting from this mandate have gone far beyond demonstrating lack of CV compromise. For many of these medication classes, studies have affirmed CV protection while providing concomitant kidney protection. Current practices can offer patients with T2D the prospect of a longer life and a higher quality of health.
Pharmacological treatment for diabetic kidney disease
In patients with established DKD, treatment goals include albuminuria regression, preservation of kidney function, and lower CVD-associated morbidity and mortality. It is generally recognized that potentially modifiable factors affecting the rate of DKD onset and progression include hyperglycemia, hypertension, dyslipidemia, smoking, nutrition, weight, and physical activity. For any given patient, successfully targeting all of these factors requires extraordinary motivation and persistence. Accordingly, treatment for DKD requires shared decision-making with a focus on individual risk-benefit assessment within the context of the degree of renal impairment as well as the comorbidities and preferences of the patient.
Glycemic control
Large clinical trials have demonstrated that strict glycemic control prevents microvascular complications including DKD in diabetic patients [9]. In fact, benefits gained from strict glycemic control extend beyond the period of trial treatment intervention. Ongoing beneficial effects on diabetic complications after a period of improved glycemic control, even if followed by a return to less intensive metabolic control has been described as a metabolic memory or legacy effect. For example, after the termination of the UKPDS (United Kingdom Prospective Diabetes Study), which ran for 20 years (1977–1997), patients were observed for a further 10 years. The difference in glycated hemoglobin (HbA1c) was lost within a year, but a lower risk of microvascular disease (–24%) and myocardial infarction (–15%) persisted in the group randomized to tight glycemic control. All-cause mortality was also reduced (–13%). These results underscore the importance of early glycemic control before complications develop.
In patients with DKD, glycemic targets need to be tailored individually. Important trials, including ACCORD (Actions to Control Cardiovascular Risk in Diabetes), VADT (Veterans Affairs Diabetes Trial), and ADVANCE (Action in Diabetes and Vascular Disease, Perindopril and Indapamide Controlled Evaluation), have tested whether strict glycemic control improves clinical outcomes. In all of these studies, no significant decreases in CV events were observed. Hypoglycemia and weight gain were greater in the intensive-therapy group. In the ACCORD trial, very tight glycemic control (HgA1c of <6% vs. 7%–7.9%) was associated with higher mortality (increase in risk by 22%, p = 0.04) [10].
Major guidelines, including Kidney Disease Improving Global Outcomes (KDIGO), recommend lowering HbA1c to a goal ranging from <6.5% to <8.0% [11]. In younger healthier patients, strict glycemic control to <6.5% is beneficial in reducing kidney disease and other microvascular complications. In contrast, for patients with advanced age, long-standing diabetes, preexisting CVD, and other severe comorbidities, or patients particularly susceptible to hypoglycemia, the risk of strict glycemic control likely outweighs any potential benefit. In these patients, the HbA1c goal may be set closer to 8.0%.
In terms of glycemic monitoring, HbA1c is widely used and should be performed routinely in all patients with diabetes as part of continuing care. The assay has limitations, however, because the result can be influenced by conditions that affect the turnover of red cells, such as anemia states and hemoglobinopathies. Supplementary options for glycemic monitoring, including daily self-monitoring or continuous glucose monitoring, play a greater role in patients with advanced-stage CKD or patients with conditions that can lead to unreliable HbA1c levels. Alternative glycemic biomarkers, such as glycated albumin or fructosamine, are used in some research settings. Experience with these in most clinical settings is limited.
Specific antihyperglycemic therapies for type 2 diabetes
For T1D, antihyperglycemic treatment is based on daily insulin injections or the use of an insulin pump. For T2D, glycemic control is best achieved with a combination of lifestyle modifications (e.g., dietary restrictions, physical activity, and weight control) and pharmacologic therapy. Before 1994, selecting an oral agent for T2D was as simple as choosing which sulfonylurea to use. Today, options for antihyperglycemic therapy with unique mechanisms of action have expanded significantly. Many of these confer additional CV and kidney protections beyond their glycemic effects. Consequently, the choice of an antihyperglycemic regimen for T2D requires careful consideration of various factors, including evidence for kidney and CV benefits, risk of medication-associated adverse events, cost, and convenience of therapy. Importantly, the kidney function of patients can impact the efficacy and safety of many antihyperglycemic therapies (Table 1) [12]. Dosing adjustments and careful monitoring for adverse effects may be required for patients with a more advanced-stage kidney disease.
For most patients with T2D and DKD, metformin and an SGLT2i are recommended as the first-line pharmacologic treatment if eGFR is above 30 mL/min/1.73 m2. For patients with lower eGFR, a GLP-1 RA with proven kidney and CV benefits should be prioritized, especially in patients at high risk for atherosclerotic CVD. There is robust data on the CV and kidney protective effects of several SGLT2i and GLP-1 RA, independent of their glucose-lowering effect. These agents should be considered the primary choice over other antihyperglycemic therapeutics such as DPP4i or sulfonylureas, especially in patients with T2D with increased risk for CVD or kidney disease. Additional detailed discussions on metformin, SGLT2i, and GLP-1 RA are presented below.
Metformin
Metformin remains the preferred initial antihyperglycemic therapy for most patients with T2D due to its low cost, high efficacy, and low risk of hypoglycemia. Additionally, it has weight- and lipid-lowering properties as well as beneficial effects on CV mortality [13]. Metformin is eliminated primarily by the kidney. Despite limited data, the potential for elevated risk of lactic acidosis in patients with lower eGFR has restricted its use to patients with an eGFR of >30 mL/min/1.73 m2.
Sodium-glucose cotransporter-2 inhibitors
SGLT2i are now widely used antihyperglycemic therapies for T2D. Multiple CV outcome trials, including the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event) trial and the CANVAS (Canagliflozin Cardiovascular Assessment Study), have demonstrated that SGLT2i provide significant kidney benefits in addition to CV benefits. For instance, secondary outcome analysis of the EMPA-REG demonstrated an impressive 39% reduction in incident or worsening kidney disease in the empagliflozin group [14]. The CANVAS-Renal trial similarly reported a 40% reduction in the composite kidney outcome (sustained reduction in the rate of eGFR decline, need for kidney replacement therapy, or death from renal causes) [15]. In contrast to these CV outcome trials, the CREDENCE (Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation) trial was designed to assess SGLT2i canagliflozin primary on kidney outcomes in T2D with albuminuric CKD. Results showed that there was a 34% reduction in kidney-specific composite outcome (ESKD, doubling of creatinine, or kidney-related death) in the canagliflozin group [16]. More recently, in the DAPA-CKD (Dapagliflozin in Patients with Chronic Kidney Disease) study, the kidney and CV benefits of the SGLT2i dapagliflozin was found to extend to patients with CKD (eGFR of 25–75 mL/min/1.73 m2) with or without T2D, thus making an argument for the use of SGLT2i in patients with CKD independent of diabetes status [17].
SGLT2i reduces renal glucose reabsorption, resulting in osmotic diuresis and plasma volume contraction. A reversible reduction in eGFR of more than 10% occurs in about a third of patients treated with SGLT2i. Although they are relatively weak glucose-lowering agents, they have the additional benefit of lowering BP and weight and do not cause hypoglycemia. Potential adverse effects include an increased risk for volume depletion, genital and urinary tract infections, perineal necrotizing fasciitis, and euglycemic ketoacidosis. The risk of lower-limb amputation was only seen in one trial with canagliflozin. Nevertheless, patients who have foot ulcers or are at high risk for amputation should be educated on proper foot care and amputation prevention. Importantly, all SGLT2i exhibit a substantial degree of renal excretion and are associated with increased accumulation and toxicity in patients with renal impairment. Specifics vary according to individual medication, but they generally should not be initiated for patients with eGFR of <25–30 mL/min/1.73 m2 (Table 1). However, once started, as long as they are tolerated well, they may be continued until the start of dialysis.
Glucagon-like peptide-1 receptor agonists
For T2D, the GLP-1 RA represent a newer family of injectable antihyperglycemic therapeutics. Liraglutide, semaglutide, and dulaglutide, in particular, have demonstrated in large CV outcome trials to have significant CV and kidney benefits, particularly in patients with established CVD or those who are at high risk. In the LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial, there was a 22% reduction in CV death and 15% reduction in death from any cause with liraglutide compared with a placebo [18]. Long-term follow-up data in patients with DKD also demonstrated a 22% reduction in the composite renal outcome, primarily due to a lower rate of severely increased albuminuria. Data on semaglutide (SUSTAIN-6 and PIONEER-6 studies) and dulaglutide (REWIND study) similarly showed CV benefits and reduced risk of albuminuria onset and kidney disease progression [19,20]. There is not yet a trial with a primary endpoint of kidney outcomes for any GLP-1 RA. The ongoing FLOW (Effect of Semaglutide Versus Placebo on the Progression of Renal Impairment in Subjects With Type 2 Diabetes and Chronic Kidney Disease) trial should address whether GLP-1 RA can slow the progression of DKD.
A number of GLP-1 RA, including liraglutide, semaglutide, and dulaglutide, have little renal clearance and are safe to use even in patients with advanced-stage DKD (Table 1) [12]. Major guidelines, including the American Diabetes Association (ADA) and the European Association for the Study of Diabetes, now recommend using GLP-1 RA to reduce CVD risk in T2D, independent of glycemic control [21]. In clinical practice, the most common adverse effects of GLP-1 RA include gastrointestinal symptoms, injection site reactions, and an increase in heart rate. GLP-1 RA should also be avoided in patients at risk for medullary thyroid tumors or a history of acute pancreatitis.
Blood pressure control
In patients with DKD, hypertension is very prevalent and is associated with renal parenchymal disease, volume expansion, and salt sensitivity. Several studies as well as real-life observations have pointed out that hypertension plays a central role in the pathogenesis and progression of kidney and CV damage. Higher BP is associated with increased albuminuria, more rapid progression, and increased risk of kidney failure [22]. Therefore, adequate BP control, irrespective of the agent(s) used, is an important strategy in the treatment of DKD.
Importantly, the issue of target BP in patients with DKD has not been clearly resolved. Many guidelines published before 2021, including the ADA (2020) and the American College of Cardiology/American Heart Association (ACC/AHA, 2020), recommended a BP target of <130/80 mmHg. Moreover, the National Institute for Health and Care Excellence (NICE, 2019) as well as the European Society of Cardiology/European Society of Hypertension (ESC/ESH, 2018) recommended a clinic BP target of <140/90 mmHg in all patients regardless of diabetes status or renal disease. Individualized consideration with a less stringent goal of <150/90 mmHg in patients aged >80 years old was also suggested. In contrast, the KDIGO 2021 clinical practice guideline for BP management in patients with CKD recommends a systolic BP target of <120 mmHg for individuals with CKD, with or without diabetes. This recommendation is based on standardized office BP measurements and referenced the large SPRINT (Systolic Blood Pressure Intervention Trial), which included mostly nondiabetic patients. Unfortunately, the balance of benefits and harms from intensive BP control remains uncertain in patients with diabetes and advanced-stage CKD. In the ACCORD-BP (Action to Control Cardiovascular Risk in Diabetes-Blood Pressure) trial, which tested a systolic BP less than 120 mmHg vs. less than 140 mmHg in patients with T2D and high CV risk, there was no significant difference between the two BP groups in the primary composite major CV outcomes. Benefits in the secondary outcome of stroke prevention were counterbalanced by an increased risk for hyperkalemia and kidney dysfunction in the intensive BP control group [23].
Consequently, similar to the glycemic target, the optimal BP target in patients with DKD is a shared decision-making process between the patient and the clinician, taking into consideration the patient’s age, CVD and stroke risk, and eGFR. In clinical practice, proper procedures used to measure BP is critical. Increased emphasis is now placed on implementing standardized BP measurements in the office and encouraging home BP monitoring. BP measurement in the office involves preparing the patient and repeated measurements separated by 1 to 2 minutes and using the average of at least two readings obtained on at least two occasions to estimate BP. Patients with DKD often have autonomic neuropathy and orthostasis, and BP measured in the upright position should be taken after a period of rest. Ambulatory BP measurements may be particularly helpful to assess BP control in patients suspected of having “white-coat hypertension” or wide variations in BP throughout the day.
Renin-angiotensin-aldosterone system blockade
Renin-angiotensin system inhibitors
Until a decade ago, the only drug class specific to the treatment of DKD were the RASi, including angiotensin-converting enzyme inhibitors (ACEi) and angiotensin II receptor blockers (ARB). Many historical studies have shown that RAS inhibition with ACEi or ARB reduces proteinuria and provides preferential kidney protection that is independent of BP reduction [24]. For T1D, there is robust data on the kidney protective effects of ACEi but insufficient data is available for ARBs. For T2D, however, several large clinical trials have demonstrated the efficacy of ARB in reducing albuminuria and the progression of nephropathy, including the RENAAL (Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan), IDNT (Irbesartan Diabetic Nephropathy Trial), IRMA 2 (Irbesartan in Type 2 Diabetes with Microalbuminuria 2), and MARVAL (Microalbuminuria Reduction With Valsartan) studies, though there are insufficient data for ACEi.
Based on the shared properties of ACEi and ARBs in inhibiting the RAS, both ACEi and ARB are believed to be effective in the treatment of T1D- and T2D-associated DKD. In a small randomized controlled trial of T2D and early nephropathy with 5 years of follow-up, the ARB telmisartan was not inferior to the ACEi enalapril in providing long-term kidney protection. The choice between these two classes of drugs usually depends on factors such as physician and patient preference, cost, availability of generic formulations, and side effect profiles of individual drugs.
Notably, several large trials have failed to show improved clinical outcomes when an ACEi was combined with an ARB, or when an ACEi or ARB was combined with the direct renin inhibitor aliskiren. Combining different RASi engenders hyperkalemia and/or acute kidney injury and should be avoided.
Aldosterone blockade
Studies of RAS inhibition do not differentiate between the relative contribution of the RAS vs. aldosterone system blockade. Plasma aldosterone levels are elevated in up to half of the patients on ACEi or ARB therapy after 12 months, known as aldosterone breakthrough. This may partly explain why RAS inhibition does not adequately regress albuminuria in a considerable proportion of patients with DKD. MRA block the effect of aldosterones on the CV and kidney systems. They have anti-inflammatory and antifibrotic effects. They have been shown to reduce proteinuria when they are used alone and have an additive effect on proteinuria when they are used in combination with an ACEi or ARB. However, the use of steroidal MRAs such as spironolactone and eplerenone is frequently limited by the presence of hyperkalemia, especially in patients with reduced eGFR.
Finerenone, which is now approved in the United States, is a nonsteroidal MRA that has greater aldosterone receptor selectivity and affinity compared to steroidal MRA, thus affording a higher potency and a lower risk of hyperkalemia. Two large randomized controlled studies have been published on finerenone in T2D on a background of maximal RAS inhibition therapy. In the FIDELIO-DKD (Finerenone in Reducing Kidney Failure and Disease progression in Diabetic Kidney Disease) study, finerenone reduced the relative risks of the primary composite outcome of CKD progression by 18%, and the secondary composite outcome of CV morbidity and mortality by 14%, in T2D with advanced CKD over a median follow-up of 2.6 years [25]. Insights into the effects of finerenone in patients with T2D and less advanced CKD was assessed by the FIGARO-DKD (Finerenone in Reducing Cardiovascular Mortality and Morbidity in Diabetic Kidney Disease) study. Results showed a 29% risk reduction in hospitalization for heart failure and a 23% risk reduction in the kidney composite outcome of kidney failure, sustained decrease from baseline GFR of >57%, or death from renal causes (2.9% vs. 3.8%) [26]. In both trials, adverse events were similar between the finerenone and placebo groups and hyperkalemia was uncommon.
Dyslipidemia control
Dyslipidemia in diabetic patients is believed to substantially contribute to the development of albuminuria and progression of DKD, although the complex pathophysiological link between the two has not been fully clarified [27]. Furthermore, in diabetic patients, the serum lipid profile changes as CKD progresses, with a shift from larger toward smaller low-density lipoprotein cholesterol (LDL-C) and an increase in triglycerides. There is evidence that both the level of proteinuria and kidney functional impairment are independently associated with altered lipid metabolism and accumulation and contribute to the development of atherosclerotic CVD [28]. Thus, dyslipidemia is believed to be partly responsible for the significant residual CV risk seen in patients with DKD, once glucose and BP control are achieved. Consequently, interventions aiming to improve lipid targets constitute an important aspect of DKD management.
Administration of lipid-lowering drugs, for the primary and secondary prevention of CVD, is an important element of DKD management. Hydroxymethylglutaryl-CoA reductase inhibitor (statin) therapy shows the strongest evidence for reducing atherosclerotic CVD and is generally considered the first choice of hypolipidemic agent. In general, lipid management guidelines emphasize the need to identify a patient’s risk for atherosclerotic CVD and the application of treatment to achieve an LDL-C level that is as low as possible for high-risk patients. Most guidelines of the United States (e.g., ACC/AHA, 2018; ADA, 2021) recommend an LDL-C reduction of ≥50% or an LDL-C goal of ≤70 mg/dL, while the European Society of Cardiology and European Atherosclerosis Society (ESC/EAS, 2019) recommend an even more stringent LDL-C goal of <55 mg/dL for those at very high risk. The addition of non-statin hypolipidemic agents (e.g., ezetimibe, fenofibrate, bempedoic acid, proprotein convertase subtilisin/kexin type 9 inhibitors [PCSK9i], or inclisiran, the newer small interfering RNA therapy) with or, in the case of PCSK9i, in place of maximally tolerated statin intensity, may be considered in high-risk patients who have not achieved lipid reduction goals. It remains unclear at this time whether any combination of dyslipidemia therapy would improve overall kidney or CV outcomes in patients with DKD.
Furthermore, there is controversy regarding the efficacy of lipid-lowering therapy once a patient reaches ESKD and is placed on dialysis. Several RCTs (4D, AURORA, and SHARP) have failed to demonstrate the benefit of statin therapy as a primary prevention of CVD in dialysis patients. In contrast, a recent observational study of 1596 incident dialysis patients in South Korea found that statin initiation was associated with a lower risk of all-cause mortality in statin-naïve ESKD patients [29]. It is unclear whether this represents an influence of race or ethnicity on the efficacy of statin therapy. Currently, there is insufficient data to recommend the use of statin therapy for primary or secondary prevention of CVD in patients on dialysis.
Nonpharmacological treatment for diabetic kidney disease
For all diabetic patients, nutritional counseling, including salt restriction and choice of carbohydrates and fats, constitutes an important component of the patient-directed self-management educational program. In particular, dietary protein restriction has been shown to improve proteinuria and slow the progression of kidney impairment [30]. In patients approaching ESKD, a low-protein diet (<0.8 g/kg/day) may also delay the onset of uremic symptoms. Protein-restricted diets should be supplemented with iron, calcium, and multiple vitamins, and should deliver ~35 kcal/kg per day.
A healthy lifestyle, including smoking cessation, exercise, and weight reduction, has also been shown to significantly reduce the risk of CV events and progression of DKD. Smoking, in particular, is an independent risk factor for CVD and DKD, and smoking cessation has been shown to improve kidney prognosis [31].
Exercise and weight reduction may also improve kidney outcomes. Secondary analysis of the Action for Health in Diabetes (look-AHEAD) randomized controlled trial found that a greater weight loss through intensive diet and exercise interventions (mean 1-year weight loss of 8.6% vs. 0.7%) was associated with a 31% reduced incidence of CKD in overweight or obese T2D patients [32]. Furthermore, there is increasing interest in the role of bariatric surgery in DKD. Results of prospective cohort studies and emerging evidence from RCT have demonstrated that bariatric surgery may prevent or slow the progression of DKD in obese patients with T2D [33].
Multidisciplinary team care
Initiating, optimizing, and sustaining evidence-based pharmacological therapy using combination therapeutics of RASi + SGLT2i/GLP1 RA + nonsteroidal MRA + statin may significantly improve outcomes for patients with DKD. In addition to pharmacological therapeutics, the prevention and treatment of DKD also necessitates dietary restrictions, lifestyle modifications such as smoking cessation and exercise, weight loss, and even bariatric surgery as necessary.
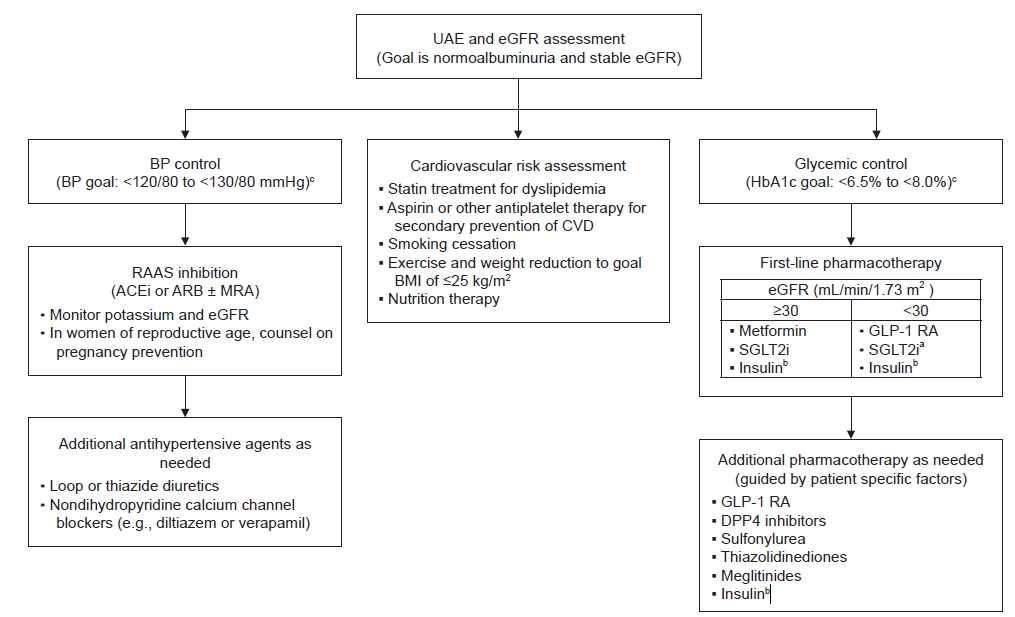
Providing early diagnosis and implementing a comprehensive treatment plan for patients with DKD is best achieved with a multidisciplinary approach, aiming at individualized blood glucose control, BP control, dyslipidemia treatment, and appropriate dietary restrictions and lifestyle modifications (Fig. 1). Even before the discovery of SGLT2i and GLP-1 RA, intensive multifactorial treatment including both behavioral and pharmacological approaches was demonstrated in the Steno 2 trial to significantly increase the lifespan of patients, lower the risk for CVD, and slow the progression of kidney disease [34].
DKD care teams should ideally consist of physicians (nephrologists and endocrinologists), pharmacists, dieticians, nurses, and ancillary medical staff. They should provide a structured self-management education program in the patient’s preferred language and engage the patients to participate in shared decision-making regarding their treatment plan. The complexity of medical regimens is a major obstacle to achieving adherence. Therefore, the patient’s preference and goals of care must be carefully considered against the anticipated benefits of each medical regimen. In accordance with KDIGO recommendations, such patient education programs should be structured, monitored, individualized, and evaluated regularly by the DKD care team to be most effective [5].
Future directions
Despite significant advances in pharmacological therapy for diabetic patients, available DKD treatments can only slow the decline in GFR, and there remains significant residual CV risk. Currently, research into potential novel therapeutic targets for DKD is particularly active and brings much anticipation and optimism to this field. New targets for therapeutic intervention include drugs that interfere with the formation and action of AGEs or receptors for AGEs, drugs that target oxidative stress, inflammatory cytokines, or fibrosis. The role of micro-RNAs in the pathogenesis of DKD is an emerging field and may also provide additional novel treatment approaches. Cell therapies targeting intrarenal vascular restitution are in early clinical trials. New insights into the molecular mechanisms that underlie the origin and progression of DKD are emerging from large-scale genetic and molecular studies in experimental models and humans.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









