



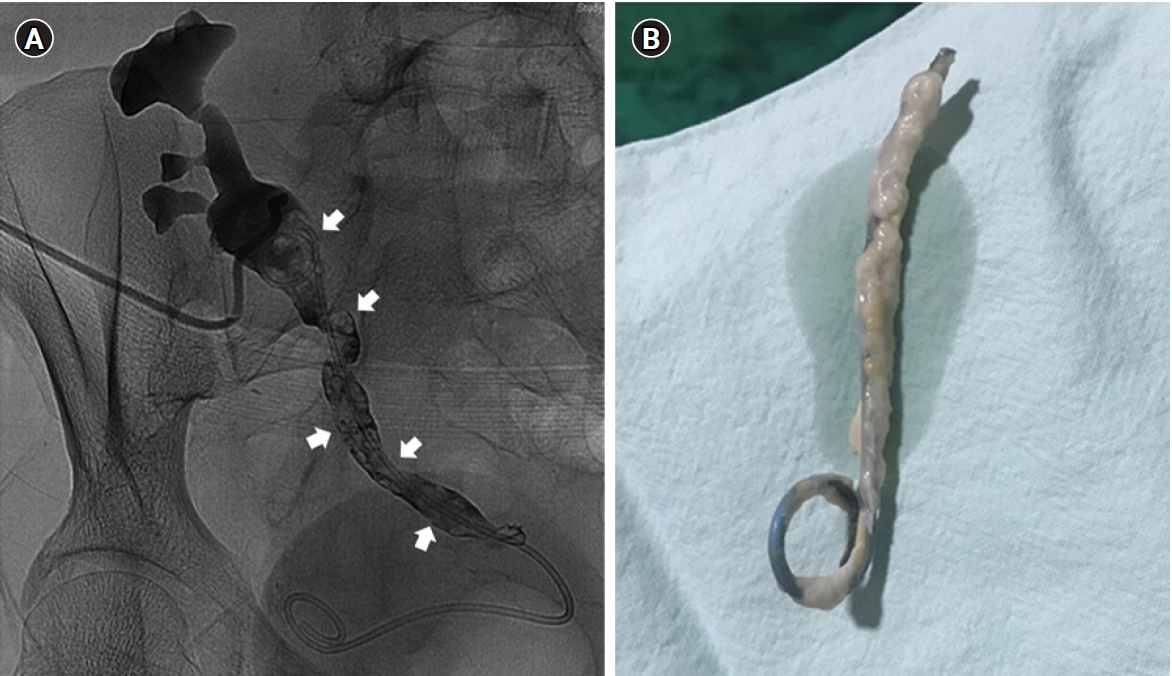
A 49-year-old female who underwent deceased donor kidney transplantation 1 month prior visited the outpatient clinic complaining of pitting edema. The patient’s end-stage kidney disease was caused by immunoglobulin A nephropathy, and hemodialysis had been performed for 7 years before the transplantation. Her serum creatinine level was 1.1 mg/dL one week previous at discharge. She received basiliximab as inductive immunosuppressive therapy and was maintained on triple immunosuppressive agents, including tacrolimus, mycophenolate mofetil, and prednisolone. The patient was given nystatin and sulfamethoxazole/trimethoprim as antifungal and antibacterial prophylaxis, respectively. Upon admission, the laboratory findings were as follows: serum creatinine, 2.6 mg/dL; C-reactive protein, 6.11 mg/dL; and pyuria. Ultrasonography revealed hydronephrosis of the graft kidney, suggesting ureteral stent obstruction. Percutaneous nephrostomy was inserted to relieve the obstruction and infection, and antegrade pyelography showed several radiolucent filling defects in the transplant ureter (Fig. 1A). Piperacillin-tazobactam empirical antibiotic therapy was initiated. Blood and urine cultures grew Candida albicans, so the initial antibiotics therapy was transitioned to intravenous fluconazole. The ureter stent was exchanged to allow complete infection treatment several days later. The removed ureter stent along with its surrounding white sheath were streaked on blood agar, MacConkey’s agar plates, and thioglycollate broth, in which Candida albicans was identified by the Vitek 2 system (bioMerieux, Marcy-l'Étoile, France) (Fig. 1B). Although the ureter stent infection was treated with antifungal therapy, a change in ureteral stent, and antegrade balloon dilatation, the patient required the ureteral stent continuously due to transplant-related ureter stricture. Therefore, the patient eventually underwent robot-assisted laparoscopic repair to reconstruct the transplant ureter stricture.
This study was approved by the Institutional Review Board of the Presbyterian Medical Center, Jeonju, Republic of Korea (No. E2022-055).
The routine use of ureter stents in kidney transplantation reduces the incidence of urological complications while increasing the risk of concurrent urinary tract infections. Urinary tract infection is the most common infectious complication after kidney transplantation. Particularly in the early posttransplant period, fungal infection of the urinary tract is typically encountered following prolonged antibiotic use, instrumentation, and indwelling urinary catheters. The most common fungal pathogens include Candida and Aspergillus species in transplant recipients. Apart from fungus balls, the radiographic differential diagnosis of filling defects on a renal allograft pyelogram should include ureteral stones, blood clots, malignancy, sloughed papilla, and organ rejection. The gold standard for diagnosing invasive Candida infection is culture of sterile body fluid. We did not assume a Candida infection until the culture results were available in the present case. Therefore, the possibility of Candida infection should be considered in cases of allograft hydronephrosis that show radiolucent filling defects in the transplant ureter, especially when accompanied by urinary tract infection.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









