



Introduction
Between 2015 and 2050, the proportion of the elderly population is estimated to double from 12% to 22% worldwide [1]. At the same time, the prevalence of mental health disorders among elderly people is growing rapidly. More than 20% of adults aged 60 and older suffer from mental health disorders [2]. The most common mental health disorders in this age group are dementia and depressive disorder (DD), which are reported to affect approximately 5% and 17% of the elderly population, respectively [3,4].
Mental health has been found to be closely related to the prevalence of kidney disease. Cognitive impairment is found in 30% to 60% of patients undergoing hemodialysis, which is at least twice the value observed in age-matched controls [5]. In addition, in a cohort of 3,349 participants, those with moderate kidney failure were associated with a 37% increased risk of dementia, showing that the link between cognitive impairment and kidney disease is not limited to patients with advanced kidney failure [6]. Similarly, DD was found in about 20% of patients with severe chronic kidney disease (CKD) and 40% of patients on dialysis [7].
The pathophysiology underlying the relationship between mental health disorders and kidney disease is not fully understood. However, the concept of brain–kidney crosstalk has been raised recently, suggesting that diseases in the kidney can affect brain function, and vice versa [8]. Retention of uremic toxins that results from reduced kidney function has been proposed as a factor that affects the central nervous system (CNS) and could initiate mental health disorders [9]. Observational studies showing an increased risk of incident dementia and DD among CKD patients suggest the presence of such kidney to brain crosstalk [5,7]. On the other hand, CNS dysfunction can induce neurohumoral changes, hormonal disturbances, and immunologic responses that could affect kidney function [10]. Nonetheless, clinical findings supporting brain to kidney crosstalk are lacking.
To assess whether mental health disorders affect kidney function, the risk of incident end-stage kidney disease (ESKD) development was compared in patients with or without Alzheimer disease (AD) or DD by evaluating claims information from a nationwide health insurance database in Republic of Korea.
Methods
Data source
Data were retrieved from the National Health Insurance Service (NHIS)-Senior cohort database. More than 98% of the Korean population is enrolled in the mandatory NHIS program, and the remaining people, who are in the lowest income bracket, receive government benefits. The NHIS-Senior cohort, composed of 558,147 people, is constructed as a 10% representative sample of 5.5 million beneficiaries aged >60 years in 2002. The cohort was followed from January 1, 2002, through December 31, 2015, or until eligibility disqualification due to death or emigration. Further details regarding the cohort have been published previously [11]. The data can be accessed on the National Health Insurance Data Sharing Service homepage of the NHIS (http://nhiss.nhis.or.kr) after approval by the National Health Information data request review committee. The NHIS-Senior cohort provides medical claims data that have been deidentified at the individual level.
This study was conducted in accordance with the principles of the Declaration of Helsinki and the protocol was approved by the Institutional Review Board of Yonsei University Health System Clinical Trial Center (No. 4-2020-1382). The informed consent requirement was waived because this was a retrospective analysis.
Study population
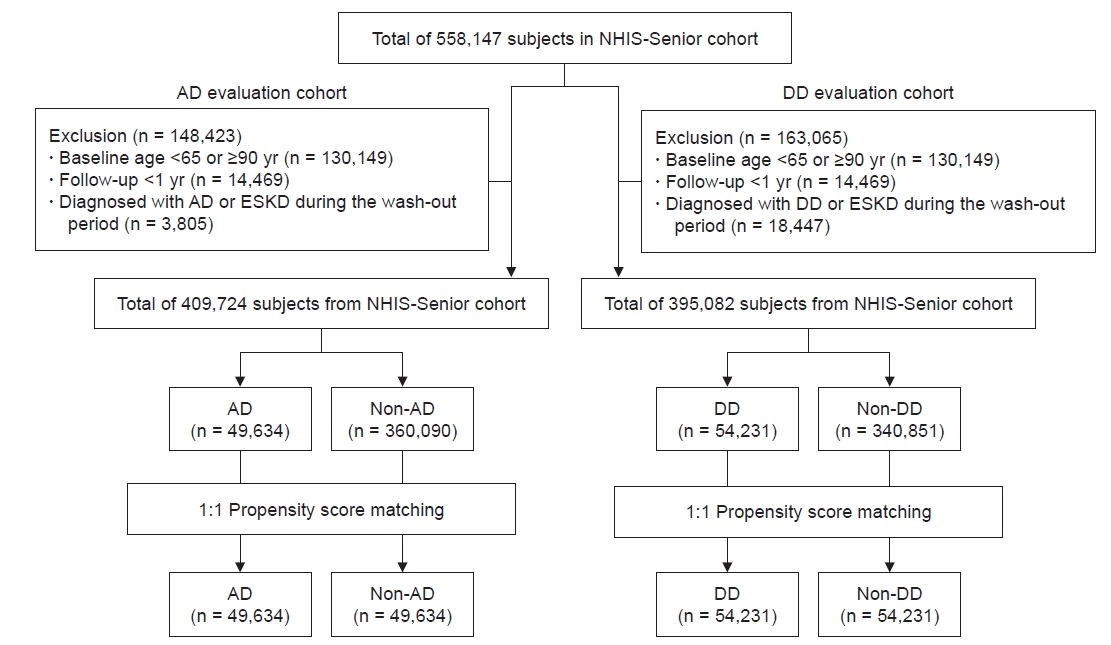
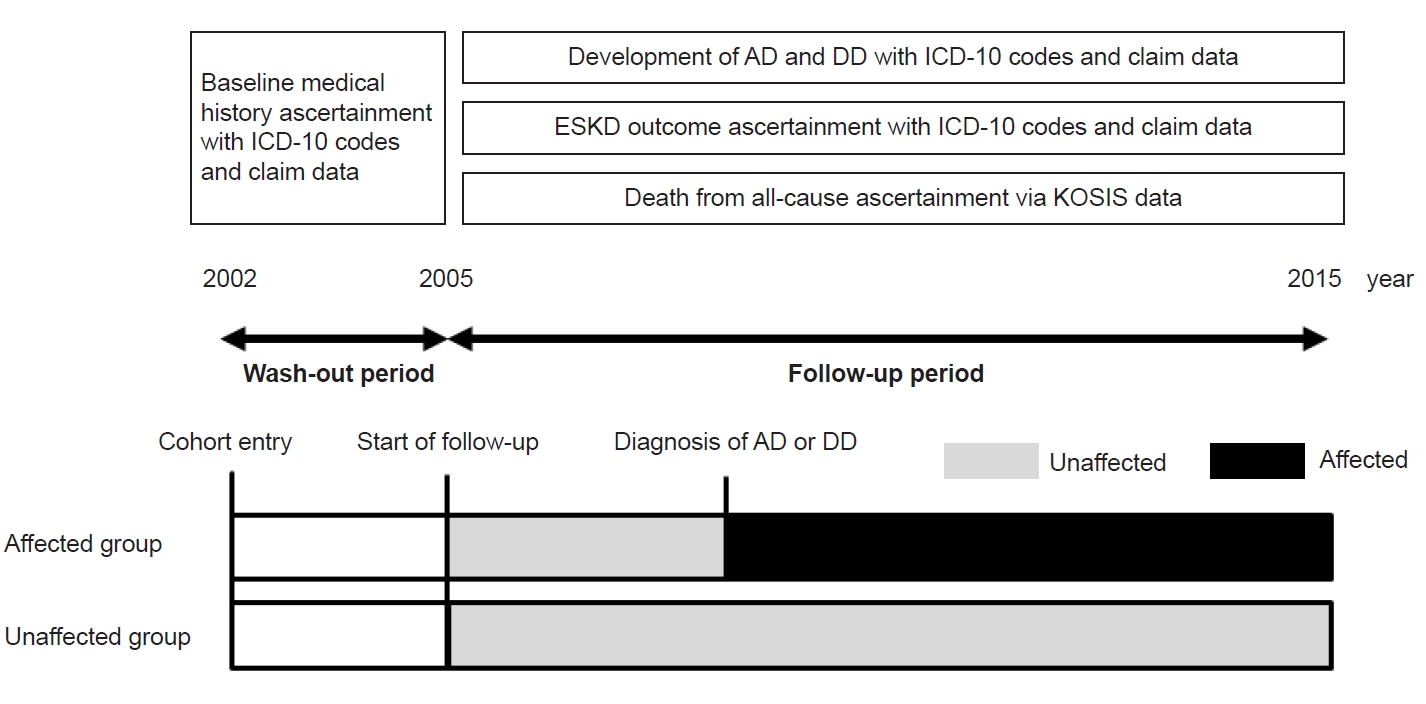
Of the 558,147 subjects in NHIS-Senior cohort, those who were younger than 65 years or older than 90 years at baseline (n = 130,149) and those who were followed for less than 1 year (n = 14,469) were excluded. A 3-year washout period was applied from January 1, 2002, to December 31, 2004. The participants were divided into AD and DD evaluation cohorts. Those diagnosed with AD or ESKD during the washout period (n = 3,805) were excluded from the AD evaluation cohort. Those diagnosed with DD or ESKD during the washout period (n = 18,447) were excluded from the DD evaluation cohort (Fig. 1). The index date for all participants was January 1, 2005 (Fig. 2).
Data collection
Baseline medical histories, including comorbidities and medications, were acquired for the washout period. Baseline demographic data of age, sex, urban residence, and income were acquired as of 2005. Diagnoses and medical services were defined based on International Classification of Diseases, 10th revision (ICD-10) codes and claim records. Diagnoses of AD and DD were defined using ICD-10 codes (F00 or G30 for AD; F32, F33, F34, or F38 for DD) and a concurrent prescription record for dementia- or DD-related treatment for at least 30 days during the follow-up period. Donepezil, rivastigmine, galantamine, and memantine were considered to be dementia-related treatments, and tricyclic antidepressants, selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and atypical antidepressants were DD-related treatments. Further details regarding the ICD-10 codes and medications used to define the covariates are presented in Supplementary Table 1 (available online). Subjects were considered to have comorbidities when the condition was a discharge diagnosis after hospitalization or was documented as a diagnosis more than once in an outpatient setting. Residential area was defined using 17 district codes, and income was determined according to participant health insurance premium in 2005.
Exposure and outcomes
Diagnoses of AD or DD were analyzed as time-varying exposures. Those newly diagnosed with AD or DD during the follow-up period were assigned to the AD or DD group, respectively (Fig. 2). Subjects diagnosed with AD or DD after development of ESKD were treated as exposure unaffected. The study outcome was development of ESKD, defined using ICD-10 codes (Z49.1, Z49.2, Z94.0, Z99.2, or T86.1) or dialysis treatment-related claim codes that were repeated for at least 90 days during follow-up.
Statistical analysis
The normality of the parameter distribution was tested graphically using histograms. All continuous variables are expressed as median and interquartile range (IQR). To account for possible differences in baseline characteristics between the affected and non-affected groups, 1:1 propensity score matching was performed using the greedy (nearest neighbor) method. The propensity score was estimated as the probability of being diagnosed with AD or DD using a logistic regression based on demographic and medical data. Standardized mean differences were determined to confirm the balance between the groups. Variables were considered well balanced when the standardized mean difference was less than 0.10. All of the covariates used for estimating the propensity score were included in the adjusted models [12]. The subdistribution hazard ratio (sHR) was assessed with all-cause death as a competing risk to evaluate the association between AD or DD and ESKD incidence using the Fine and Gray method [13]. The index date of the subdistribution hazard model was January 1, 2005, and the subjects were followed to the censoring point, defined as development of ESKD or eligibility disqualification (Fig. 2). The proportional hazard assumption was tested based on Schoenfeld residuals [14]. Sensitivity analyses were performed to confirm the main findings. First, considering the possibility of selection bias inherent in the matching procedure, evaluations were performed using the propensity scores as weights to account for selection assignment differences [15]. The top and bottom one percentiles of the weight were eliminated to reduce the effect of extremely small or large weights. Second, subgroup analyses were performed according to sex, residential area, and disease onset. Median age at AD or DD diagnosis was determined from the entire cohort, and early onset was defined as a diagnosis before the median age for that disease. Third, to consider the possibility that CKD could have a causal effect on AD or DD development, analyses were conducted after excluding participants diagnosed with CKD of <180 days prior to AD or DD diagnosis. For all analyses, a p-value less than 0.05 was considered statistically significant. All statistical analyses were performed using Stata for Windows version 15.0 (StataCorp LLC, College Station, TX, USA) and SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline characteristics
The baseline characteristics of the participants before propensity score matching are shown in Supplementary Table 2 (available online). In the AD evaluation cohort, 360,090 and 49,634 participants were allocated to the non-AD and AD groups, respectively. The median age of the patients in the AD group was 74 years (69–78 years), and 30.1% were male. Compared with the non-AD group, those in the AD group were older, more likely to be female, and had lower prevalence of hypertension (HTN) and peripheral arterial disease. In the DD evaluation cohort, the non-DD and DD groups contained 340,851 and 54,231 people, respectively. In the DD group, the median age of patients was 70 years (67–75 years), and 34.8% were male. Those in the DD group were younger and more likely to be female than subjects in the non-DD group. Patients in the AD and DD groups were subjected to 1:1 propensity score matching within the AD evaluation cohort and DD evaluation cohort, respectively. After propensity score matching, baseline characteristics were well balanced (Table 1).
Incidence of end-stage kidney disease
In the AD evaluation cohort, during a median (IQR) follow-up of 10 years (9–10 years), 297 and 168 cases of incident ESKD occurred in the non-AD and AD groups, respectively. Per 1,000 person-years, the incidence rate of ESKD was 0.36 in the non-AD group and 1.17 in the AD group (Table 2). During a median (IQR) follow-up duration of 10 years (10–10 years) in the DD evaluation cohort, 309 and 216 cases of incident ESKD occurred in the non-DD and DD groups, respectively. The corresponding incidence rates per 1,000 person-years were 0.36 in the non-DD group and 0.91 in the DD group (Table 2).
Effect of Alzheimer disease or depressive disorder on end-stage kidney disease development
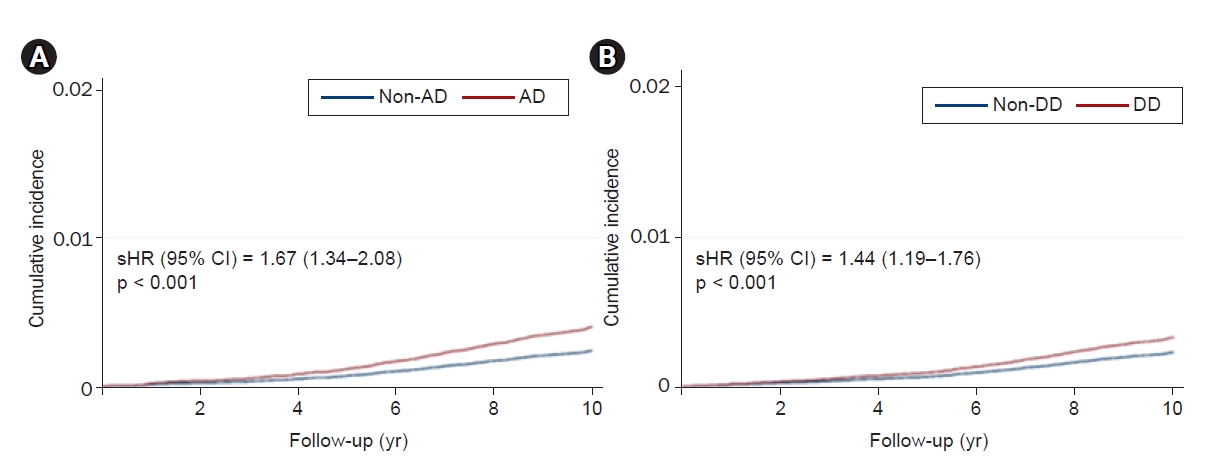
When subdistribution hazard models were constructed with death as a competing risk for incident ESKD, the risk of ESKD development was significantly higher in the AD group than the non-AD group (sHR, 1.86; 95% CI, 1.50–2.30) in the AD evaluation cohort. This risk was attenuated but still statistically significant after adjusting for additional confounding variables (sHR, 1.67; 95% CI, 1.34–2.08). In the DD evaluation cohort, the risk of ESKD was higher in the DD group than the non-DD group (sHR, 1.75; 95% CI, 1.43–2.13), and that relationship was maintained after adjusting for additional confounding demographic and clinical variables (sHR, 1.44; 95% CI, 1.19–1.76) (Table 2). The cumulative incidence curves constructed for participants in the AD evaluation cohort show that the time to development of incident ESKD was significantly longer in the non-AD group than the AD group (p < 0.001) (Fig. 3A). Similarly, the time to incident ESKD development in the DD evaluation cohort was significantly longer in the non-DD group than the DD group (p < 0.001) (Fig. 3B).
When subgroup analyses were performed according to sex, residential area, and AD or DD onset, no significant interactions were found between the subgroups, suggesting that the associations found in the main analysis would be significant regardless of subgroup (Table 3).
Sensitivity analyses
To further account for possible selection bias, evaluations were made after propensity score weighting. In the AD evaluation cohort, the risk for ESKD development was higher in the AD group than in the non-AD group (adjusted sHR, 1.51; 95% CI, 1.27–1.79). In the DD evaluation cohort, ESKD development risk was higher in the DD group than the non-DD group (adjusted sHR, 1.18; 95% CI, 1.02–1.37) after adjusting for confounding factors (Supplementary Table 3, available online). To minimize possible causal effects of CKD on development of AD or DD, evaluations were conducted after excluding those diagnosed with CKD prior to diagnosis of AD or DD. The baseline characteristics of those participants are shown in Supplementary Tables 4 and 5 (available online). Evaluations of those participants revealed that the incident ESKD risk was still higher in the AD group than the non-AD group (adjusted sHR, 1.37; 95% CI, 1.06–1.77) and higher in the DD group than the non-DD group (adjusted sHR, 1.33; 95% CI, 1.07–1.60) after adjusting for confounding factors (Supplementary Table 6, available online).
Discussion
This study evaluated the risk of ESKD development among patients diagnosed with AD or DD using data from a nationwide representative elderly population cohort in Republic of Korea. The incidence rate of ESKD was higher among those with AD or DD than in people without AD or DD, respectively. In addition, those with AD or DD were at a higher risk for developing ESKD. This association was significant even after adjusting for confounding factors, including underlying CKD. Moreover, the significance of the relationship was maintained in sensitivity analyses using propensity score weighting. These findings suggest that preceding mental health conditions such as AD and DD affect kidney function, increasing the risk of ESKD.
Connectivity between the kidney and the CNS is suggested as one cause of the high prevalence of CNS disorders in patients with kidney disease. The possibility that underlying kidney disease could give rise to neurologic complications through cytokine-induced damage, oxidative stress, and accumulation of neurotoxic metabolites has been demonstrated in clinical and animal studies [8,16,17]. Recently, in addition to that kidney to brain crosstalk, the possibility of brain to kidney crosstalk has been proposed on the basis of several clinical phenomena. Acute kidney injury is a common accompaniment of traumatic brain injury and ischemic stroke, with reports that up to 23% of traumatic brain injury patients develop acute kidney injury [18–20]. In addition, hemodynamic and neurohormonal changes and induction of inflammatory responses upon brain death are implicated as key factors that cause acute rejection after kidney allograft transplantation [10]. However, those findings mainly involve acute disease states, and whether CNS disorders chronically affect kidney function is not well known. The results of this study, which show that the risk of ESKD is significantly higher in AD or DD patients than in people without those underlying mental health problems, suggest that brain to kidney crosstalk could chronically affect kidney function. These results are supported by a recent study conducted in China that showed that severity of depressive symptoms correlated with rapid kidney function decline [21].
Several steps of this study aimed to increase the likelihood that the assessed risk would be determined by AD or DD and not by other confounding factors. HTN and diabetes mellitus (DM) are underlying conditions well known to affect kidney function. The prevalence of patients with DM did not differ between those with or without AD or DD even before propensity score matching. Although patients with HTN were more prevalent in the non-AD group than the AD group, the difference was not large and was well balanced after propensity score matching, lowering the chances that underlying comorbidities played a role in the elevated ESKD risk reported here. In addition, the association between incident ESKD and AD or DD was maintained following additional confounding factor adjustments and propensity score matching. Moreover, when propensity score weighting was used to balance the baseline characteristics between groups with or without AD or DD, the significance of risk increase was maintained, which further reduced the possibility that confounding factors affected the reported risk of ESKD development.
Underlying CKD is another potential factor that can affect ESKD risk, with the rate of kidney function decline being aggravated in patients with CKD [22]. However, the prevalence of CKD at baseline did not differ between the groups with or without AD or DD. In addition, further adjustments for prevalent CKD after propensity score matching did not compromise the association between incident ESKD risk and AD or DD. Moreover, in the sensitivity analysis that excluded patients diagnosed with CKD before AD or DD diagnosis, the incident ESKD risk increase in patients with AD or DD was maintained, suggesting that this association is independent of underlying CKD. Nonetheless, the possibility that other factors not included in the analyses affect the risk of ESKD development cannot be ignored, and evaluations that include more variables are required to confirm the findings of this study.
Several mechanisms could explain the increased risk of ESKD in patients with AD or DD. An increase in sympathetic nervous system activity can alter kidney blood flow and glomerular filtration, leading to accelerated kidney function decline [10]. The dysregulation in sympathetic tone that results from an acute brain injury is suspected to be one reason that traumatic brain injury patients often develop acute kidney injury [23]. Reports showing that sympathetic nervous system activity is elevated in patients with AD or DD further support that possibility [24,25]. Alterations in the cerebral renin-angiotensin system (RAS) might also contribute to the brain to kidney crosstalk observed in this study [26]. An animal study in rats revealed that the cerebral RAS affects kidney function in DM [27]. Changes in cerebral RAS have also been implicated in patients with DD [28,29]. In addition, upregulation of the brain RAS has been closely linked to the pathogenesis of AD [29,30]. Systemic inflammation caused by CNS disorders might also affect kidney function. Microglial cells in AD have been reported to release inflammatory cytokines, including interferon-γ and interleukin (IL)-1β [31–33]. In DD patients, serum levels of IL-6 and tumor necrosis factors have been found to be increased [34]. Considering that chronic systemic inflammation is a well-known risk factor for kidney disease, the inflammatory milieu accompanying AD and DD could increase the risk of ESKD in such patients [35].
Kidney function is a known risk factor for mental health disorders [7,36,37]. Although kidney function could not be accurately determined because of the inevitable limitations of analyzing a large health insurance claims database, several actions were taken to reduce the chances of underlying kidney disease affecting the onset of ESKD. First, propensity score matching was conducted between the groups with or without AD or DD for underlying CKD. In addition, matching was performed for major CKD risk factors such as HTN, DM, and heart failure. Second, to further reduce the possibility of bias, additional adjustments were made in assessing the sHR, including CKD and CKD risk factors as covariates. Third, a sensitivity analysis excluding those diagnosed with CKD at baseline was performed to lower the chances that underlying CKD played a role. Nonetheless, completely eliminating the probability that undetermined underlying CKD had an effect on the outcome was not possible with this dataset. Therefore, the suggestive findings of this study need to be evaluated in further investigations that include data on kidney function.
This study has several limitations. First, the limitations related to the observational nature of this study should be addressed. Although actions to evaluate the risk of ESKD after onset of AD or DD have been applied, no causal relationship can be ascertained due to the retrospective design of this study. Further prospective investigations are needed to confirm the findings of this study. Second, because the evaluation used information from a NHIS claims database, the possibility of misclassified comorbidities should be considered. In addition, diagnosis codes for a particular comorbid condition might have been omitted if the patient was not being actively treated for that comorbidity. Nonetheless, the accuracy of AD classification through ICD-10 codes has been validated for the NHIS database [38]. In addition, concurrent use of AD- and DD-related medications was considered to improve diagnostic precision. Because all dialysis patients in the Republic of Korea are supported by a copayment assistance policy through the NHIS, ESKD outcomes are accurately identifiable. Third, laboratory data and detailed demographic data were not available. Although CKD was considered as a comorbidity based on diagnosis codes, it was not possible to account for relative kidney function. In addition, factors that could have affected DD, such as family history or occupational status, could not be included in the analyses.
In conclusion, the risk of ESKD development was higher in elderly patients diagnosed with AD or DD than in those who did not have those disorders. These results suggest that preceding mental health disorders could play a role in subsequent development of kidney disease. However, further detailed prospective investigations are needed for confirmation.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









