



Introduction
The number of kidney transplant (KT) procedures in older patients has been increasing [1]. Older recipients are characterized by attenuated immune function, which contributes to a less frequent rejection and a higher rate of infectious complications after KT [2]. Recent guidelines recommend age-adopted immunosuppression for KT recipients [3]; however, convincing evidence of the optimal immunosuppression in the older population is still lacking.
Induction treatment is one of the most important parts of immunosuppression. Basiliximab (BSX), which is a monoclonal interleukin-2 receptor (IL-2R) antibody, and antithymocyte globulin (ATG), which is a polyclonal antibody that mainly depletes T cells, are the two most commonly used induction agents currently [4]. The superiority of ATG over BSX with respect to reducing rejection events in immunologically high-risk kidney recipients has been proven [5,6]. However, it is not clear whether ATG has advantageous effects in low-risk recipients. Several studies showed that ATG could lower the biopsy-proven rejection (BPR) or even result in better graft survival in patients with low immunologic risk [7–9]. However, there has yet to be a randomized trial to evaluate these effects in KT recipients who underwent steroid withdrawal immunosuppression [10].
ATG warrants several adverse effects, such as cytokine release syndrome [5], infection [11,12], and posttransplant malignancy [13,14], of which all were more critical in the elderly population. However, ATG minimizes the use of calcineurin inhibitors and steroids [15,16], which could result in higher long-term graft function and better glucose control. A recent French observational study showed that ATG compared with BSX was related to neither better nor poorer graft survival as well as patient outcomes, except for lowering posttransplant diabetes mellitus (DM) in elderly KT recipients [17]. They included a relatively small sample size in both groups and only included deceased donor KT (DDKT); thus more evidence is still needed. Therefore, we compared ATG and BSX as induction therapies in older KT recipients (≥60 years) using matched analysis with Korean multicentric registry data.
Methods
Ethics approval
This study was performed under the tenets of the Declaration of Helsinki and the Declaration of Istanbul. The study protocol was approved by the Yonsei University Wonju College of Medicine (No. CR321365), which provided an exemption for informed consent because of the retrospective nature of the study.
Study population
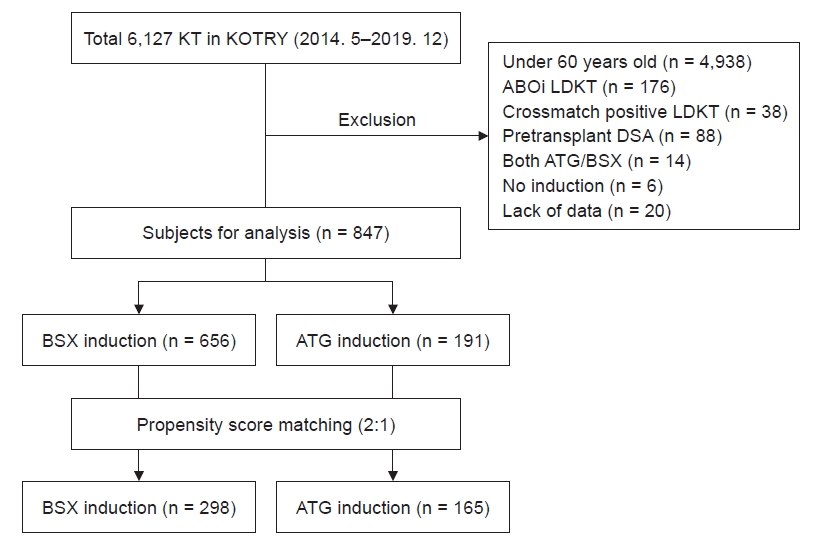
A retrospective analysis was performed on 6,127 patients who received KT between May 2014 and December 2019 as registered in the Korean Organ Transplantation Registry (KOTRY). We excluded patients who were under the age of 60 years (n = 4,938), ABO-incompatible (ABOi) living donor KT (LDKT) (n = 176), crossmatch-positive LDKT (n = 38), pretransplant donor-specific antibody (DSA) (n = 88), received both ATG and BSX induction therapy (n = 14), no induction therapy (n = 6), and insufficient data (n = 20). Finally, 847 low immunologic risk (crossmatch-negative, ABO-compatible, and no pretransplant DSA) elderly KT recipients were included in the study (Fig. 1).
Data collection
The demographics of the recipients and donors were sourced from the KOTRY database. The number of mismatches for human leukocyte antigen regarding A, B, and DR were collected. Pretransplant peak panel-reactive antibody (PRA) was categorized as 0% to 20%, 21% to 80%, and 81% to 100%. As PRA is a critical factor for posttransplant BPR, those with missing PRA were placed in a separate category, which accounted for approximately 30% of the study population. We separately collected donor factors, such as donor age, sex, body mass index (BMI), history of hypertension (HTN), history of DM, and serum creatinine, at donation. The cause of death for deceased donors and cold ischemic time (CIT) for all donors were also collected, as well as for deceased donors apart.
According to the data collection interval of the KOTRY, serum creatinine, immunosuppressant regimens, steroid use, and mycophenolate mofetil (MMF) or its equivalent (360 mg of enteric-coated mycophenolate being equivalent to 500 mg of MMF) were collected at discharge, 6 months, 12 months, and annually thereafter.
Tacrolimus (TAC) trough level was collected from 6 months onward, as the KOTRY collected it from a later period of this study. Graft function was evaluated by estimated glomerular filtration rate (eGFR) calculated by The Modification of Diet in Renal Disease equation [18].
Outcomes
Primary outcomes include BPR, death-censored graft failure, and patient death. BPR except borderline findings was separately analyzed from the entire BPR. Secondary outcomes include graft function, BK virus nephropathy (BKVN), infection, cancer, new-onset DM after transplantation (NODAT), and delayed graft function (DGF). BKVN was checked only when confirmed in renal biopsies. Infection was counted when the patient was admitted with confirmed pathogens. The most common types of infection were urinary tract infection, bacterial pneumonia, bacteremia, viral infection, viral pneumonia, fungal infection, and Pneumocystis jiroveci pneumonia. Each transplant institution reported DM to the KOTRY registry. Regarding early hyperglycemia, we excluded patients who were diagnosed with DM only during the early posttransplant period and reported with no DM after the follow-up period. NODAT was compared only in patients without pretransplant DM. DGF was defined as a need for dialysis within 7 days after KT.
Statistical analysis
A 2:1 propensity score-matching was performed between BSX and ATG groups with the nearest neighbor method. A caliper was set at 0.2 standard deviations (SDs). All available baseline factors were included as matching covariates, except the cause of death for donors and CIT, because our study contained a considerable LDKT population. The balance of the covariates was considered appropriate when the standard mean differences were between 0.1 of one another [19]. Cases outside of balance were discarded from both groups during matching; hence complete matching between the two groups was not achieved.
Regarding the comparison of numerical variables, the Student t test or Mann-Whitney U test was used, and the paired t test or McNemar test was used for the comparison of variables between matched groups. The results were presented as mean ± SD or median (interquartile range [IQR]) according to their normality. The chi-square test was used for categorical variables. Kaplan-Meier analysis was used to compare the cumulative probability of posttransplant events, and statistical significance was confirmed by the log-rank test. All analyses were performed using standard software (IBM SPSS version 25.0; IBM Corp., Armonk, NY, USA and R freeware version 3.6.3; R Foundation for Statistical Computing, Vienna, Austria). The p-values of <0.05 were considered statistically significant.
Results
Baseline characteristics
Table 1 shows the baseline characteristics of the BSX and ATG groups before and after matching. Before matching, 656 older recipients (≥60 years, 77.4%) received BSX as induction therapy, whereas 191 (22.6%) received ATG as induction therapy. Age, sex, BMI, and the cause of end-stage renal disease were similar between the groups. However, the ATG group showed more frequent retransplantation (2.9% vs. 9.9% in the BSX and ATG groups, respectively; p < 0.001) and longer pretransplant dialysis duration (43.5 ± 51.0 months vs. 61.4 ± 52.4 months, respectively; p < 0.001). PRA was significantly different between both groups (p = 0.003), especially the 81st to 100th percentile of PRA values was higher in the ATG group than in the BSX group (1.4% vs. 5.2%). The proportion of DDKT was higher in the ATG group than in the BSX group (50.6% vs. 82.7%, p < 0.001). Several donor risk factors, such as male sex (54.0% vs. 68.1%, p = 0.001), creatine at donation (1.0 ± 0.8 vs. 2.0 ± 1.7, p < 0.001), HTN (22.9% vs. 30.4%, p = 0.034), and DM (9.1% vs. 16.2%, p = 0.005) were higher in the ATG group than in the BSX group, so was expanded criteria donor (ECD), accordingly (25.5% vs. 41.9%, p < 0.001). CIT, which was available only in 78.5% of the study population, was longer in the ATG group than the BSX group. However, it became similar when compared considering DDKT only (298.5 ± 145.5 minutes vs. 296.9 ± 148.6 minutes, p = 0.93).
By propensity score matching, 165 patients in the ATG group were matched to 298 patients in the BSX group with adequate balance (Supplementary Fig. 1, available online). The similarity in all baseline covariates was achieved between the BSX and ATG groups after matching, as shown in Table 1. Some factors were excluded from the matching, including ECD, vascular cause of death, and CIT. The mean total dose of ATG was 4.7 ± 1.6 mg/kg in the ATG group. All patients in the BSX group received two doses of 20 mg BSX on postoperative days 0 and 4.
Maintenance immunosuppression
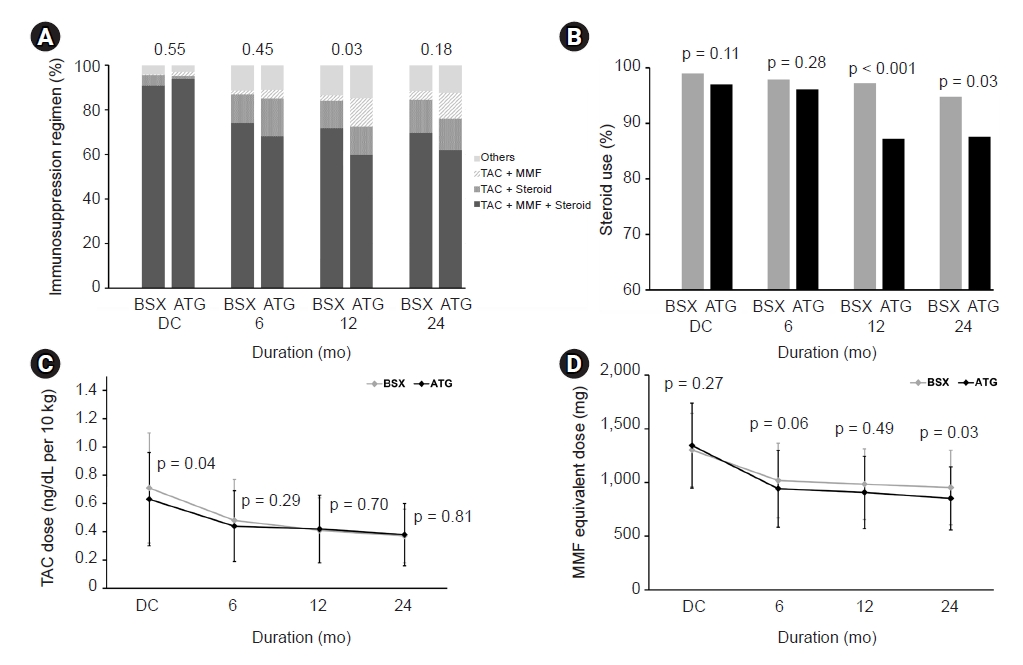
Fig. 2 shows the comparison of maintenance immunosuppressants between the BSX and ATG groups. Most patients of both groups used a combination of TAC, MMF, and steroids at discharge, and no differences were found among the regimen types. At 6 months, the proportion of the triple regimen declined, whereas TAC plus steroid regimen became more common (12.8% vs. 16.9% for BSX and ATG, respectively) in both groups. One year after KT, the type of immunosuppression was significantly different between groups (p = 0.03) (Fig. 2A), and the proportion of TAC plus MMF was especially higher in the ATG group than in the BSX group (2.4% vs. 12.8%, p < 0.001). The proportion of steroid use was significantly lower in the ATG group than in the BSX group from both 1 and 2 years after KT (97.2% vs. 87.2%, p < 0.001 at 1 year; 94.8% vs. 87.6%, p = 0.03 at 2 years) (Fig. 2B), although the daily steroid dose in the patients on maintenance steroid treatment was similar from discharge to 2 years after KT in both groups (Supplementary Fig. 2, available online). The cumulative incidence of pulse steroid therapy within 6 months was significantly lower in the ATG group (7.3%; one patient received pulse steroid therapy twice, and 11 patients received pulse steroid therapy once) than in the BSX group (15.4%; five patients received pulse steroid therapy twice, and 41 patients received pulse steroid therapy once) (p=0.01). The median TAC trough level was significantly lower at 6 months after KT in the ATG group than in the BSX group (6.4 [IQR, 5.1–8.1] vs. 5.7 [IQR, 4.5–7.1], p = 0.001), but they then became similar from 1 year onwards (Supplementary Fig. 3, available online). At the discharge date, the TAC dose in the ATG group was significantly lower than in the BSX group (0.63 ng/dL per 10 kg vs. 0.71 ng/dL per 10 kg, p = 0.004) (Fig. 2C). The mean equivalent maintenance dose of MMF was not different at discharge and 6 months. However, it was lower in the ATG group than in the BSX group after 1 year postoperation (984 ± 329 mg vs. 907 ± 338 mg, p = 0.049) (Fig. 2D).
Primary outcomes
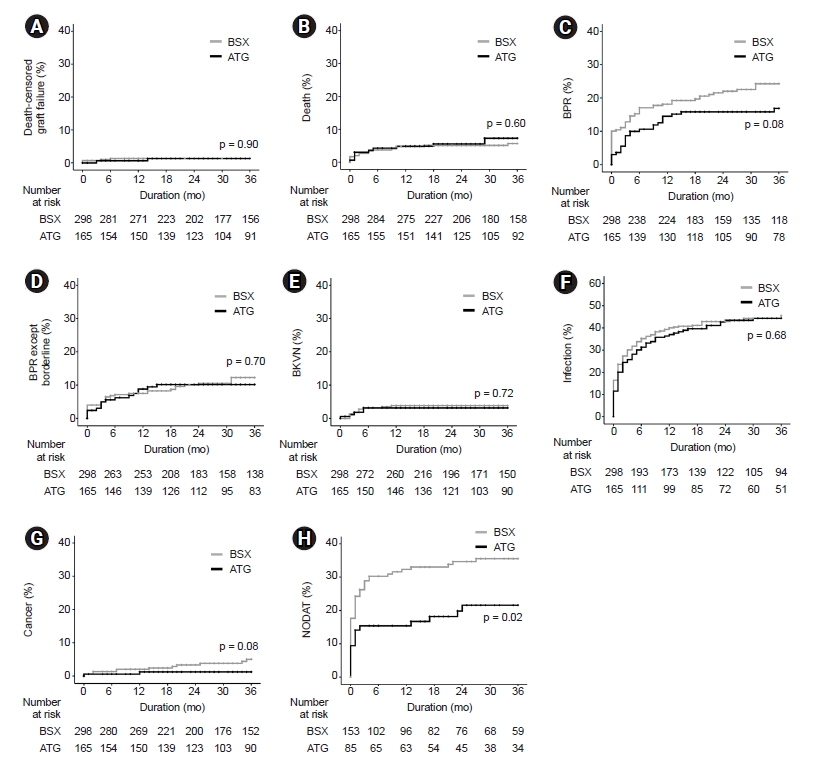
During 28.5 ± 10.4 months of mean follow-up, six patients (1.3%) experienced death-censored graft failure, and 27 patients (5.8%) died with a functioning graft. The cumulative probability of death-censored graft failure was 1.4% at both years 1 and 3 of follow-up in the BSX group, and the corresponding probabilities were 0.6% and 1.3% in the ATG group (p = 0.90) (Fig. 3A). The cumulative probability of patient death was 4.7% at year 1 and 5.7% at year 3 of follow-up in the BSX group vs. 4.9% at year 1 and 7.3% at year 3 of follow-up in the ATG group (p = 0.60) (Fig. 3B). The cumulative probability of BPR was 18.1% at 1 year and 24.3% at 3 years postoperation in the BSX group, whereas the cumulative probability of BPR was 14.5% at 1 year and 16.9% at 3 years postoperation in the ATG group. BPR was numerically lower in the ATG group than in the BSX group, though without statistical significance (p = 0.08) (Fig. 3C). Furthermore, BPR probability was similar between the ATG and BSX groups, except for pathologically borderline rejection (7.5% at 1 year and 12.3% at 3 years in the BSX group compared to 8.8% at 1 year and 10.2% at 3 years postoperation in the ATG group, p = 0.70) (Fig. 3D).
Secondary outcomes
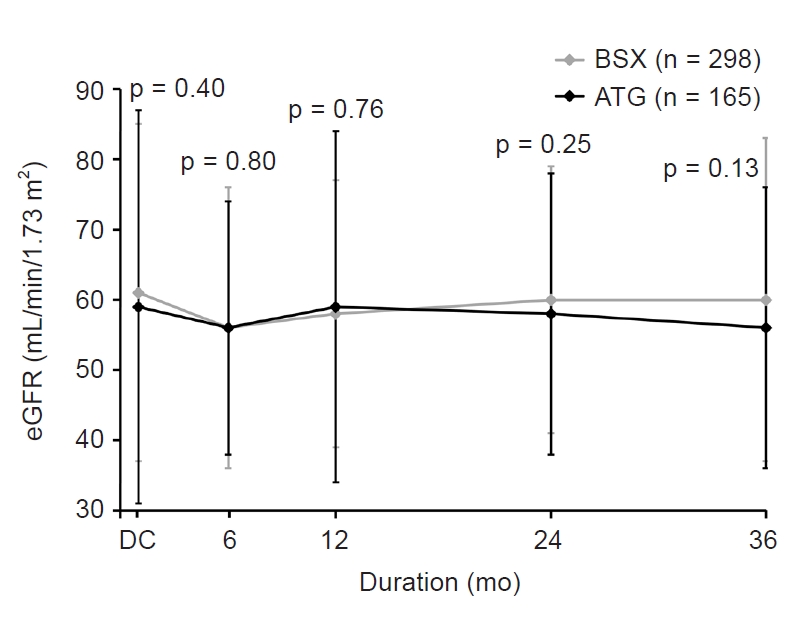
DGF occurred in 9.5% of the BSX group and 8.5% of the ATG group without a significant difference (p = 0.83). The cumulative probability of BKVN was similar between the two groups (3.9% at both years 1 and 3 in the BSX group and 3.1% at both years 1 and 3 in the ATG group, p = 0.72) (Fig. 3E). The cumulative probability of infection was 39.3% at 1 year and 44.3% at 3 years postoperation in the BSX group, whereas the corresponding values were 37.0% and 44.3% in the ATG group (p = 0.68) (Fig. 3F). Not only was the cumulative probability of infection similar between the two groups but so were the cumulative probabilities of urinary tract infection, bacterial pneumonia, bacteremia, viral infection, viral pneumonia, fungal infection, and Pneumocystis jiroveci pneumonia (Table 2). The cumulative probability of cancer after KT was numerically lower in the ATG group (1.3% at both 1 year and 3 years postoperation) vs. the BSX group (2.1% and 5.0% at 1 year and 3 years postoperation) without any significance (p = 0.08) (Fig. 3G). Among patients without pretransplant DM, the cumulative probability of NODAT was significantly lower in the ATG group than in the BSX group (32.3% at 1 year and 35.6% at 3 years postoperation in the BSX group compared to 15.4% at 1 year and 21.6% at 3 years postoperation in the ATG group, p = 0.02) (Fig. 3H). Graft function was similar throughout the study period between the BSX and ATG groups, at approximately 60 mL/min/1.73 m2 eGFR (Fig. 4). Besides, ATG dose did not affect the rate of death-censored graft failure, death, BPR, antibody-mediated rejection, BKVN, infection, cancer, or NODAT (Supplementary Table 1, 2, available online).
Discussion
From matched analysis with the Korean multicentric registry, this study comprehensively compared the outcomes between two induction therapies, BSX and ATG, in older KT recipients. ATG did not have superiority over BSX for DGF development or graft function throughout the study period. The ATG group not only showed a lower TAC trough level and cumulative proportion of pulse steroid therapy at 6 months but also lower steroid use than the BSX group from 1 year after transplantation onwards. The type of induction regimen did not affect death-censored graft failure or patient survival. BPR, BKVN, infection, and cancer were not significantly different in patients who received BSX or ATG. However, the probability of NODAT was significantly lower in the ATG group than in the BSX group among the patients without pretransplant DM.
Different from the United States’ report [20], ATG is less used in the entire KT population than BSX. Especially, the proportion of patients who received BSX induction was much higher in the elderly KT population, as shown in our supplementary data (Supplementary Fig. 4, available online). This can be attributed to LDKT predominance and the relatively short CIT for DDKT due to the geographical features of Korea, which then leads to less preference for ATG as induction therapy.
IL-2R antibody induction therapy has no significant effect on the rate of rejection or patient or graft survival in TAC-based maintenance immunotherapy in standard-risk KT recipients [21]. Perioperative antibody induction is associated with a lower risk of mortality in DDKT recipients with low immunologic risk [22]. However, several studies, including meta-analyses, have demonstrated that antibody induction is not associated with an increased risk of all-cause mortality or graft loss [23–26].
Before matching for baseline features, the ATG group had more frequent retransplantation, higher PRA and DDKT, and more marginal donors than the BSX group. Those features of the BSX group were similarly matched to the ATG group by matching that ended up with population. However, there was no difference in DGF development between the two groups. With an in vivo mechanism of reducing leukocyte adherence to antigen-presenting endothelial cells [27], ATG has shown a protective effect on DGF in several studies [28,29]. The discrepancy in our results could be attributed to the relatively good donor condition, including approximately 20% LDKTs and less than 6 hours of mean CIT for the DDKT population. The mean donor creatinine at donation was 1.6 to 1.7 mg/dL, and the incidence of DGF was under 10% in our matched population, which resulted in no difference in DGF development between the ATG and BSX groups.
ATG was reported to be superior to BSX in preventing rejection in not only high-risk patients but low-risk KT patients as well [5–8]. The current study revealed that the incidence of BPR may have been lower in the ATG group than in the BSX group without statistical significance. Excluding borderline BPR, the incidence of BPR, which is clinically important, is similar between the two groups. This result is consistent with prior research in France, which revealed no difference in rejection rates between the two groups, unlike preexisting large database studies [17].
The rejection prevention effect of ATG is not sufficient due to the attenuated immunity of older patients with a low risk of rejection [29]. Additionally, past studies only considered zero mismatch before transplantation, so there is a possibility that high-risk patients with acute preoperation existing DSA were included. The French study and our study excluded patients with detectable DSA as the Luminex assay base. Compared to BSX, ATG was not effective in preventing rejection since it was mainly used for low-risk patients.
Compared to BSX treatment, the incidence of leukopenia is higher following ATG treatment due to the effect of global T cell depletion; therefore, careful infection monitoring is necessary [30]. These infections could become more serious, especially in elderly patients [11]. Similarly, the previous French study revealed no increased incidence of infection in the ATG group, as in our study. A previous study of ABOi LDKT in elderly patients revealed that infection-related death in DDKT recipients is higher than that of ABOi KT recipients due to the use of ATG; thus, ATG induction therapy should be carefully monitored in the elderly [31]. According to some studies, KT recipients who received ATG are at a higher risk of infection [26,32].
In contrast to the French study and ours, the majority of study participants use steroids as maintenance therapy. Furthermore, some studies describe the use of cyclosporin-based immunosuppressive therapy rather than TAC-based immunosuppressive therapy. As a result, in addition to ATG, several other factors may have played a role in the infection-related complications described herein. Similar to the French study, this matched analysis showed that ATG induction itself did not increase the risk of infection in elderly KT recipients. This result could be important evidence to determine the induction regimen for elderly patients.
Similar to the French study [17], our study revealed that the only difference between the ATG and BSX groups was NODAT. Our study also revealed that the TAC requirement in the first 6 months of transplantation was lower in the ATG group than in the BSX group. Different from the French study, our results showed that the proportion of patients using steroids from 1 year after transplantation was significantly lower in the ATG group. No difference was found in the number of patients who required continued steroid use. No evidence suggests that ATG could be used for more effective rejection prevention in early steroid withdrawal, as shown in other randomized controlled trials [10]. Although the difference in the prevalence of BPR is not statistically significant between groups, the lower prevalence of rejection, including borderline rejection, in the ATG group affected the low incidence of pulse steroid therapy. As shown in Supplementary Fig. 2, steroid dosage (maintenance dose) did not differ between the two groups. However, the cumulative probability of pulse steroid therapy at 6 months after operation was significantly lower in the ATG group than in the BSX group. From 1 year after transplantation, a higher proportion of patients treated with steroids experienced withdrawal in the ATG group. It can be inferred that the frequency of steroid dose reduction and withdrawal was high from around 6 months after transplantation for both groups. The relationship between steroid use and NODAT has already been reported [10]. Low doses of TAC and steroids might be associated with a lower incidence of NODAT in the ATG group. In our study, the ATG group required a lower dose of steroids and TAC to maintain immunological safety, which led to a significantly decreased NODAT. The reduction of NODAT in the ATG group is thought to be greater in elderly patients with an already higher propensity for NODAT [33].
This study has several limitations. This is a retrospective study with relatively small sample size and unmeasured confounders. A discrepancy was found in the immunosuppressive treatment strategies among institutions contributing to the KOTRY. The comparison of immunosuppressive regimens and dosages relies not on consecutive data but on spot measurements due to the data collection policy of the KOTRY. We could not compare induction regimens across institutions or obtain TAC trough levels at discharge due to internal KOTRY registry regulations. There is no information provided about the institution where a specific patient may have worked. Despite these limitations, this study used a large multicenter database with matched analysis and compared ATG and BSX induction therapies among elderly low-risk patients. No difference was found in graft survival, all-cause mortality, rejection, or infection between the ATG and BSX groups. However, ATG reduced maintenance TAC and steroid requirements and NODAT incidence compared to BSX.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









