



Introduction
Acute kidney injury (AKI) is a common complication among critically ill patients worldwide and is associated with substantial morbidity and mortality rates of 50% to 90% [1]. Approximately 5% to 10% of AKI patients require acute renal replacement therapy (RRT) during intensive care unit (ICU) admission [2ŌĆō4]. AKI patients requiring RRT are reported to have very high mortality rates, as much as 50% to 80% [5]. Risk factors for mortality include advanced age, sepsis, disease severity and number of failing organs, need for mechanical ventilation, presence of circulatory shock, and oliguria [6]. Several studies have also established the relationship between fluid overload (FO) and mortality [7ŌĆō10].
Continuous RRT (CRRT) is the preferred renal replacement modality in the management of critically ill patients with hemodynamic instability and AKI [5]. The Kidney Disease: Improving Global Outcome (KDIGO) Clinical Practice Guideline for AKI suggests that CRRT be used for hemodynamically unstable patients and patients with acute brain injury or other causes of increased intracranial pressure [11]. Many studies show that CRRT offers superior hemodynamic stability, metabolic clearance, and volume control. Other advantages of CRRT include enhanced clearance of inflammatory mediators and better preservation of cerebral perfusion among patients with acute brain injury or fulminant hepatic failure [12].
The limited availability in some areas and the high cost of CRRT, in addition to the high mortality rate among critically ill patients with severe AKI, warrant careful selection of patients who will benefit from it. Identifying patients who are most likely to have positive outcomes with CRRT is challenging. More studies are needed to identify such patients to guide therapeutic decisions, optimize limited resources, and provide realistic prognostic information to patients and their families. This study aims to determine mortality rates and identify factors associated with mortality among critically ill patients in the ICU with AKI who received CRRT.
Methods
Research design
This is multicenter observational study comprising all AKI patients who were admitted and received CRRT in the ICUs of Seoul National University Bundang Hospital, Seoul National University Hospital, Seoul National University Boramae Medical Center, and Ehwa Womans University Mokdong Hospital, from June 2017 to September 2018.
This study was approved by the Institutional Review Boards of Seoul National University Bundang Hospital (No. 1801-44-106), Seoul National University Hospital (No. 1801-036-913), Seoul National University Boramae Hospital (No. 10-2018-05), and Ehwa Womans University Mokdong Hospital (No. 2018-01-071). This study was performed in accordance with the Declaration of Helsinki. Informed consent was waived because the study is retrospective and noninterventional in nature.
Inclusion and exclusion criteria
All patients with AKI who received CRRT in the ICUs of Seoul National University Bundang Hospital, Seoul National University Hospital, Seoul National University Boramae Hospital, and Ehwa Womans University Mokdong Hospital from June 2017 to September 2018 were eligible. Patients already on chronic dialysis before the study period were excluded.
Data collection
Records of ICU patients with AKI who received CRRT over the study period were retrieved. Baseline demographics such as age and sex, preexisting comorbid conditions, and etiology of AKI were collected. Although AKI is often multifactorial, we classified patients into one of four etiologic groups: (1) septic, (2) cardiogenic, (3) postoperative, and (4) others. Use of mechanical ventilation and vasopressor(s), urine output 24 hours prior to CRRT, length of stay in the ICU and in the hospital, and time on CRRT were also noted. Disease severity was assessed using the Sequential Organ Failure Assessment (SOFA) score. Laboratory findings were also recorded.
Definitions
The AKI diagnostic criteria utilized in this study were in accordance with the 2012 KDIGO Clinical Practice Guideline for AKI: increase in serum creatinine (SCr) Ōēź 0.3 mg/dL within 48 hours, increase in SCr Ōēź 1.5 times the baseline, or urine volume < 0.5 mL/kg/hour for 6 hours [11]. The degree of FO was expressed as percent FO, which was calculated as follows: [(weight at start of CRRT ŌĆō baseline body weight)/baseline body weight] ├Ś 100.
Groups
Patients were grouped according to presence and degree of FO: group 1, no FO; group 2, FO Ōēż 10%; and group 3, FO > 10%. Patients were also classified according to SOFA score: A, low SOFA score (<10) and B, high SOFA score (Ōēź10), using the median SOFA score.
Outcomes
The primary outcomes were in-hospital mortality and 90-day mortality. We analyzed 90-day mortality to reduce bias related to short-term prognosis brought about by the acute illness.
Statistical analysis
Categorical data are expressed as the number of cases and percentages. Continuous data are expressed as the mean ┬▒ standard deviation (SD). Statistical comparisons were made between survivors and non-survivors using the independent t-test and the chi-square test, as appropriate. The Cox proportional hazards model was used to explore the effect of variables on mortality. The adjusted model included age, sex, hypertension, diabetes mellitus (DM), malignancy, and sepsis. Mortality data were analyzed using Kaplan-Meier survival curves. Statistical significance was defined as a p-value of <0.05. All statistical analyses were performed using IBM SPSS version 20 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
We identified 414 critically ill patients with AKI who received CRRT. When patients were divided into survivor and non-survivor groups, there was no difference in the age or sex distribution (p = 0.50 and p = 0.90, respectively). The mean age was 65.8 ┬▒ 15.3 years in the survivor group and 66.8 ┬▒ 14.4 years in the non-survivor group. A majority of the patients in both groups (67.8% and 68.4%, respectively) were male. The two most common comorbidities among all patients were hypertension and DM. The non-survivors had a higher mean SOFA score (10.3 ┬▒ 3.8 vs. 8.9 ┬▒ 3.2, p < 0.001), lower mean arterial pressure (77.8 ┬▒ 15.8 mmHg vs. 83.2 ┬▒ 17.6 mmHg, p = 0.001), and required at least one vasopressor (78.1% vs. 62.1%, p < 0.001). A majority of the patients in both groups required mechanical ventilation (56.5% among survivors vs. 74.3% among non-survivors, p < 0.001). Sepsis was the most common cause of AKI in either group. The mean SCr was lower in the non-survivor group (2.9 ┬▒ 1.7 mg/dL vs. 4.3 ┬▒ 3.1 mg/dL in the survivor group, p < 0.001). A higher proportion of patients in the non-survivor group had FO at the time of CRRT initiation (51.1% vs. 34.5%, p = 0.001). Table 1 shows the baseline clinical characteristics of the patients, stratified by in-hospital mortality.
Outcomes
The in-hospital mortality rate was 57.2% (237 of 414). Of the 177 patients who survived to hospital discharge, five patients expired in the 90 days following the start of CRRT. The 90-day mortality rate was 58.5%.
Factors associated with in-hospital and 90-day mortality
In our study, age was not found to significantly affect in-hospital or 90-day mortality (p = 0.45, respectively). Sex was also not significantly associated with mortality (in-hospital, p = 0.876; 90-day, p = 0.816).
Analysis showed that a lower SCr and blood pH and a higher SOFA score were independently associated with increased risk for in-hospital and 90-day mortality. A 1-SD increase in SCr and blood pH was associated with a decreased risk of in-hospital mortality (SCr: HR, 0.87; 95% confidence interval [CI], 0.81ŌĆō0.93; p < 0.001 / blood pH: HR, 0.15; 95% CI, 0.06ŌĆō0.36; p < 0.001) and 90-day mortality (SCr: HR, 0.84; 95% CI, 0.79ŌĆō0.90; p < 0.001 / blood pH: HR, 0.17; 95% CI, 0.07ŌĆō0.42; p < 0.001). On the other hand, a 1-unit increase in SOFA score was significantly associated with increased risk of in-hospital mortality (HR, 1.06; 95% CI, 1.02ŌĆō1.09; p < 0.001) and 90-day mortality (HR, 1.07; 95% CI, 1.04ŌĆō1.10; p < 0.001). More importantly, after adjustment for demographic factors and the other variables, SCr, blood pH, and SOFA score each remained significantly associated with in-hospital mortality (SCr: HR, 0.87; 95% CI, 0.81ŌĆō0.93; p < 0.001 / blood pH: HR, 0.11; 95% CI, 0.04ŌĆō0.28; p < 0.001 / SOFA score: HR, 1.05; 95% CI, 1.01ŌĆō1.08; p = 0.008). By multivariate Cox regression analysis, SCr (HR, 0.86; 95% CI, 0.80ŌĆō0.93; p < 0.001), blood pH (HR, 0.16; 95% CI, 0.06ŌĆō0.43); p < 0.001), and SOFA score (HR, 1.06; 95% CI, 1.02ŌĆō1.09; p = 0.001) were associated with 90-day mortality, independent of age, sex, comorbidities, and sepsis (Table 2).
FO was likewise significantly associated with an increased risk of in-hospital (HR, 1.54; 95% CI, 1.19ŌĆō1.98; p = 0.001) and 90-day mortality (HR, 1.57; 95% CI, 1.22ŌĆō2.02; p < 0.001). Patients with FO were 1.39 times (95% CI, 1.07ŌĆō1.81; p = 0.02) more likely to die within 90 days following CRRT initiation after adjustment for age, sex, SCr, blood pH, SOFA score, DM, hypertension, malignancy, and sepsis (Table 2).
Subgroup analyses
We also classified the patients according to degree of FO. One hundred fifteen patients (27.8%) had FO of Ōēż10%, while 67 patients (16.2%) had more severe FO of >10%. Two hundred thirty-one patients (55.8%) did not present with FO on CRRT initiation. Our results showed that mortality rates increased as the degree of FO increased. The highest mortality rates were recorded in patients with FO > 10% (in-hospital mortality: 82.1% vs. 57.4% in FO Ōēż 10%, p < 0.001; 90-day mortality: 85.1% vs. 59.1% in FO Ōēż 10%, p < 0.001).
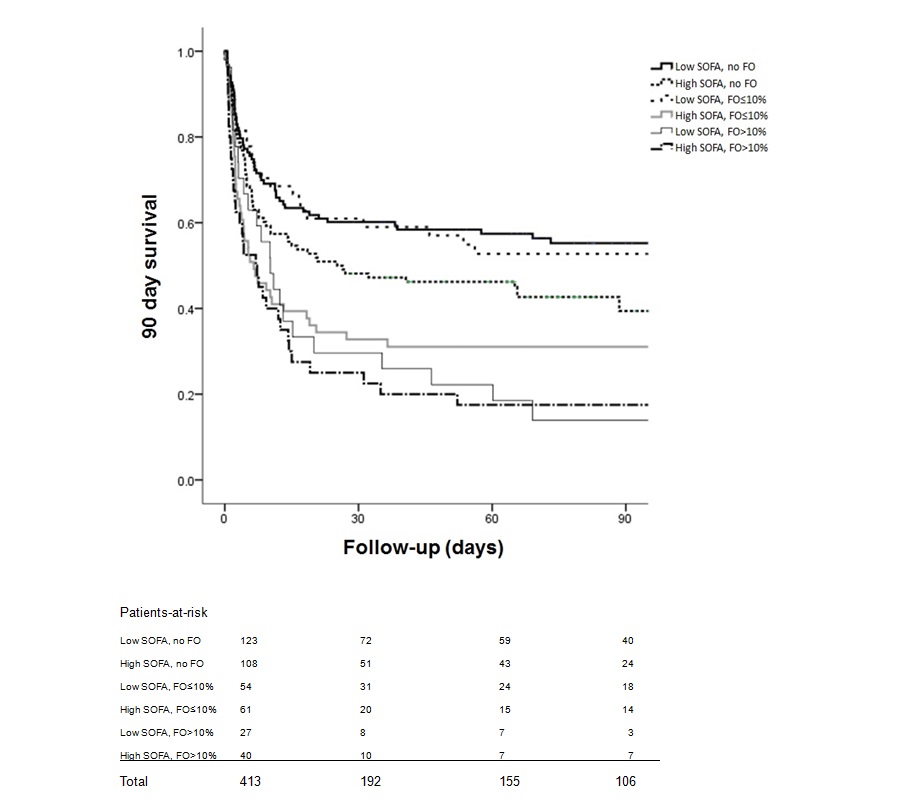
We further subdivided the patients into the following six groups to examine whether the increased mortality risk observed in patients with FO was adversely affected by SOFA score: group 1A, no FO and low SOFA score; group 1B, no FO and high SOFA score; group 2A, FO Ōēż 10% and low SOFA score; group 2B, FO Ōēż 10% and high SOFA score; group 3A, FO > 10% and low SOFA score; and group 3B, FO > 10% and high SOFA score (Table 3, 4).
In patients without FO (group 1), higher mortality was observed in the high SOFA subgroup (in-hospital: group 1B, 58.3% vs. group 1A, 43.1%; 90-day: group 1B, 58.3% vs. group 1A, 43.9%). Hazard ratios were 1.85 (95% CI, 1.10ŌĆō3.12; p = 0.02) for in-hospital mortality (Table 3) and 1.79 (95% CI, 1.06ŌĆō3.02; p = 0.03) for 90-day mortality in group 1B (Table 4).
Among patients with FO Ōēż 10%, a high SOFA score (group 2B) was also associated with increased hazard ratios for both in-hospital mortality (2.92; 95% CI, 1.53ŌĆō5.59; p = 0.001) and 90-day mortality (3.05; 95% CI, 1.59ŌĆō5.88; p = 0.001).
Among patients with a low SOFA score, it is noteworthy that the mortality risk of patients with FO Ōēż 10% (group 2A) was not statistically different from that of patients without FO (group 1A) (in-hospital: HR, 1.06; 95% CI, 0.56ŌĆō2.01; p = 0.87 / 90-day: HR, 1.10; 95% CI, 0.58ŌĆō2.09; p = 0.77).
Patients with FO > 10% had the highest risk of in-hospital mortality (group 3A: HR, 5.81; 95% CI, 2.07ŌĆō16.35; p = 0.001 / group 3B: HR, 6.23; 95% CI, 2.56ŌĆō15.17; p < 0.001) and 90-day mortality (group 3A: HR, 10.22; 95% CI, 2.92ŌĆō35.75; p < 0.001 / group 3B: HR, 6.02; 95% CI, 2.47ŌĆō14.67; p < 0.001) among the entire study population (Table 3, 4, respectively). The Kaplan-Meier survival curves also showed that survival was lowest in group 3 (Fig. 1, 2).
Discussion
We studied a multicenter population of 414 ICU patients with AKI who subsequently underwent CRRT. This study showed that the mortality rate was high among critically ill patients who received CRRT (in-hospital, 57.2% and 90-day, 58.5%). Our result is comparable to mortality rates in previously published data [3,13ŌĆō15] but better than those reported by Prasad et al. [16] (64%), Kao et al. [17] (66.5%), and Gonzalez et al. [18] (68.4%). Some studies have even reported in-hospital mortality as high as 70%ŌĆō80% [19,20].
Several articles have previously cited male sex, older age, and sepsis as risk factors for severe AKI requiring RRT [3,8]. Similar to previous studies, a majority of the patients in this study were male (282, 68.1%) [17,21]. The mean age was 66.4 ┬▒ 14.8 years, and most of the patients were Ōēź65 years (250, 60.4%). The most common etiology of AKI was sepsis, as was the case in the studies conducted by Kao et al. [17], Gonzalez et al. [18], and Soni et al. [19].
The association between advanced age and mortality among AKI patients has been extensively studied [17ŌĆō19]. In a study by Allegretti et al. [14] of 725 AKI patients who received CRRT, age over 60 years was an independent risk factor of in-hospital mortality (odds ratio [OR], 1.9; 95% CI, 1.3ŌĆō2.7; p = 0.001) and mortality following hospital discharge (HR, 1.9; 95% CI, 1.2ŌĆō3.0). Another study by Conroy et al. [22] reported that patients 75 years and older had higher hospital mortality (54.2% vs. 44%, p = 0.02) and 1-year mortality (63.6% vs. 50.6%, p = 0.005) than younger patients. Although poor outcomes have been observed in elderly AKI patients, this has not been consistent across all studies [23]. A retrospective study done in Germany of 424 patients found that the course and prognosis of AKI do not differ greatly in the elderly population [24]. Our study also did not identify age as a predictor of mortality in patients with CRRT-requiring AKI.
A lower SCr and blood pH and a higher SOFA score were independently associated with an increased risk of death. Several studies have identified high SCr as an independent factor for better outcomes [20,25]. Soubrier et al. [26], in a study of 197 patients treated with CRRT, found that SCr > 3.4 mg/dL predicted a favorable outcome. In our study, the non-survivors had a lower mean SCr at CRRT initiation. A 1-SD increase was associated with a decreased risk of in-hospital and 90-day mortality (HR, 0.87 and 0.84, respectively; p < 0.001). Possible explanations for this occurrence are decreased protein production and reduced muscle mass among the more critically ill patients. SOFA represents a severity parameter and is widely accepted as a prognostic factor for critically ill patients. In a study of 240 patients with AKI who received CRRT, Kee et al. [27] found that blood pH < 7.35 (OR, 4.33; 95% CI, 2.41ŌĆō7.77; p < 0.001) and a 1-SD increase in SOFA score (OR, 1.99; 95% CI, 1.49ŌĆō2.69; p < 0.001) were significantly associated with mortality within 7 days of CRRT initiation. Another single-center, retrospective cohort study of 562 patients also reported that acidemia and a higher SOFA score at the time of CRRT initiation were independently associated with a higher short-term mortality rate (death in-hospital or within one week of discharge) [28].
FO is known to be associated with mortality in critically ill patients with AKI [4,25,29]. Similar to other studies, and not surprisingly, FO was associated with increased mortality in our study. Although most studies have defined FO as more than a 10% increase in body weight relative to baseline, we included patients with less than 10% increase in body weight from baseline in our analysis since a study by Bagshaw et al. [30] found that a lower threshold of fluid accumulation (>5%) was associated with hospital mortality (OR, 2.31). This negative effect of FO Ōēż 10% on survival was more clearly seen in patients presenting with more severe illness (group 2B). Patients with a lesser degree of FO (<10%) should be given more attention since they are also at an increased risk for adverse outcomes. Timely recognition and subsequent management of FO in its earlier stages could positively impact patientsŌĆÖ hospital course and long-term prognosis.
Moreover, our results showed that a higher degree of FO was associated with higher risk of mortality. We observed a relationship between increasing degree of FO, increasing SOFA score, and mortality. In a study of 341 AKI patients who underwent CRRT, Kim et al. [31] observed that the adverse effect of FO on survival was more evident in patients with sepsis or more severe illness. In contrast, our results revealed that the increased risk of mortality associated with FO was also observed in patients with a low SOFA score. Patients with FO > 10% and low SOFA score (group 3A) were 5.8 times more likely to die in-hospital than patients with no FO and low SOFA score (group 1A). This risk increased to 6.3 when patients had high SOFA score and FO > 10% (group 3B). This highlights the importance of proper fluid management among critically ill patients with AKI regardless of disease severity.
This study showed that mortality following CRRT initiation for AKI was high. Our study demonstrated that SCr, blood pH, SOFA score, and FO are significant independent risk factors for in-hospital and 90-day mortality after adjustment for age, sex, sepsis, and comorbidities. In patients without FO and with FO Ōēż 10%, a lower SOFA score corresponded to a lower risk of in-hospital and 90-day mortality. Patients with FO > 10% had worse outcomes regardless of SOFA score.
In conclusion, the presence of FO signifies an increased risk of mortality independent of other factors, including severity of acute illness. Prevention of FO should be a priority, especially when managing the critically ill. Measures to ensure this include correctly identifying patients who are fluid-responsive, choosing the appropriate type and quantity of fluids to be given, and frequent clinical assessment of fluid status. Benefits and risks should always be weighed prior to starting or deciding to continue fluid therapy. A judicious fluid therapy is indispensable in the management of critically ill patients.
Although the predictors we identified in this study were identified separately in previous studies, our findings reaffirm the clinical importance of these factors in the management and prognosis of critically ill patients with AKI. This study has several strengths. It is a multicenter study and also included a larger number of patients compared to previous studies. Our findings can be extended to other ICU patients. This is an observational study. Interventions were not standardized. The decision to start CRRT, choice of CRRT modality, and CRRT prescription were made by the attending nephrologist. Our results can only predict the associations between factors and outcomes but do not determine causal relationship.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









