



Introduction
Chronic kidney disease (CKD) is a major health problem worldwide [1,2]. Patients with CKD have increased risk of end-stage renal disease (ESRD), cardiovascular disease, and all-cause mortality [2-4]. Risk factors for development and progression of CKD are similar to those implicated in cardiovascular disease, including hypertension, diabetes, and dyslipidemia [5-7]. Among these factors, abnormal lipid metabolism is common in patients with kidney disease [8]. Previous experimental studies have shown that hyperlipidemia is associated with kidney injury [9,10]. Several epidemiologic studies demonstrated that dyslipidemia is significantly associated with increased risk of reduced kidney function or greater decline in estimated glomerular filtration rate (eGFR) in the general population without kidney disease [11,12]. However, the effects of statins on kidney disease progression in patients with CKD remain controversial [13].
High-intensity statin therapy can reduce the risk for cardiovascular events regardless of baseline risk [14,15]. The 2013 American College of Cardiology/American Heart Association (ACC/AHA) lipid guidelines recommend statin dosing in adults based on intensity, rather than targeting specific low-density lipoprotein cholesterol (LDL-C) concentration. The 2013 Kidney Disease: Improving Global Outcomes (KDIGO) lipid guidelines also recommend use of statins for most patients with CKD aged Ōēź 50 years and with eGFR < 60 mL/min/1.73 m2, in light of their high cardiovascular risk, based on previous randomized trial data on lipid-lowering therapy in CKD [16,17]. However, there have been conflicting results regarding the beneficial effect of statins on kidney function. Moreover, observational studies have reported an increased risk of acute kidney injury after initiation of high-intensity statin [18,19], raising concern for worsening kidney function in patients with CKD and long-term use of high-intensity statin. It is well-known that statin therapy in patients with CKD is not as effective as in people without CKD. The reason for this is not clear, but we hypothesized that statin intensity might modify the relationship between statin use and adverse clinical outcomes in patients with CKD.
Thus, we aimed to investigate whether higher-intensity statin therapy is associated with lower risk of CKD progression in Korean adults with CKD.
Methods
Study participants
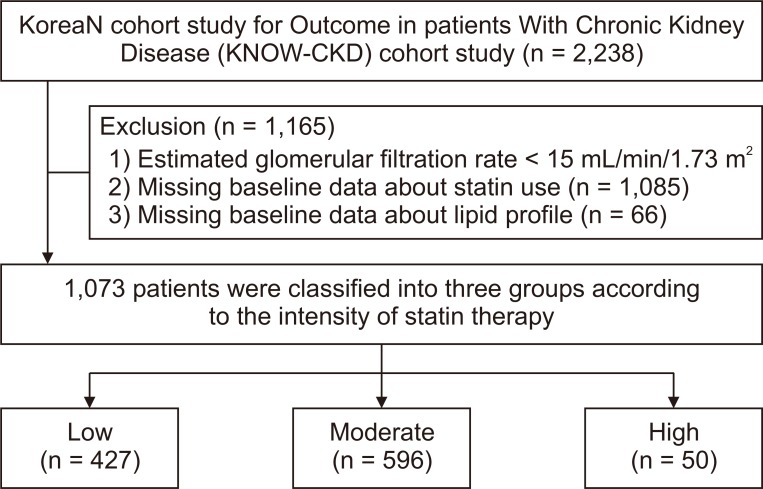
The Korean Cohort Study for Outcome in Patients With Chronic Kidney Disease (KNOW-CKD) is a prospective nationwide cohort study investigating various clinical courses and risk factors for CKD progression in Korean patients. Patients aged between 20 and 75 years with CKD stages from 1 to 5 before dialysis who voluntarily provided informed consent were enrolled from nine tertiary-care general hospitals throughout Korea between June 2011 and February 2016. The study rationale, design, methods, and protocol summary are provided in detail elsewhere (NCT01630486 at http://www.clinicaltrials.gov) [20]. Among 2,238 patients in the KNOW-CKD cohort, 1,085 with baseline eGFR < 15 mL/min/1.73 m2 and missing data regarding statin therapy or lipid profiles were excluded. Finally, 1,073 patients were included in the present analysis (Fig. 1). All included patients provided written informed consent, and the study was approved by the institutional review board of each participating center. All investigators conducted this study in accordance with the guidelines of the 2008 Declaration of Helsinki.
Data collection
Demographic data were collected from all patients, including age, sex, smoking status, social history, and medical history. Smoking status was classified as never, past, or current. Education level was categorized as low, less than middle school; middle, middle school; and high, more than middle school. Income level was divided into three groups: low, < $1,200 per month; middle, $1,200 to $3,800 per month; and high, Ōēź $3,800 per month. Anthropometric data including height and weight were collected upon enrollment. Body mass index (BMI) was calculated by dividing initial body weight by height in meters squared. After 5 minutes of seated rest, blood pressure (BP) was measured using an electronic sphygmomanometer. Hypertension was defined as history of physician-diagnosed hypertension, systolic BP (SBP) Ōēź 140 mmHg, diastolic BP Ōēź 90 mmHg, or use of antihypertensive drugs. Diabetes was defined as history of physician-diagnosed diabetes, fasting glucose Ōēź 126 mg/dL, post-load glucose level Ōēź 200 mg/dL, HbA1c Ōēź 6.5%, or use of insulin or oral antidiabetic drugs. Charlson Comorbidity Index was assessed using the method described previously [21]. The 10-year atherosclerotic cardiovascular disease (ASCVD) risk scores were calculated according to the risk assessment equation from the 2013 ACC/AHA guidelines [22]. After an overnight fast, venous samples were collected to determine hemoglobin, serum urea nitrogen, creatinine, fasting plasma glucose, albumin, calcium, phosphate, total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol, LDL-C, and high-sensitivity C-reactive protein levels. Serum creatinine was measured by an isotope dilution mass spectrometry-traceable method at the central laboratory (Lab Genomics, Seoul, Korea). The CKD Epidemiology Collaboration equation was used to determine eGFR [23]. The second voided or random urine was collected, and samples were immediately sent to the central laboratory. Proteinuria was determined by 24-hour urinary protein excretion test (g/24 hr).
Intensity of statin therapy
Intensity of statin therapy was defined based on the expected LDL-C reduction indicated in clinical trials, as summarized in the 2013 ACC/AHA guidelines (Supplementary Table 1; available online) [14].
Study outcomes
Study participants were followed-up until March 31, 2018. The study endpoint was a composite of doubling of serum creatinine, Ōēź 50% decline in eGFR, initiation of dialysis, or kidney transplantation.
Statistical analysis
All statistical analyses were performed using IBM SPSS software for Windows ver. 24.0 (IBM Corp., Armonk, NY, USA), SAS software ver. 9.2 (SAS Institute Inc., Cary, NC, USA), and R software ver. 3.3.1 (http://www.R-project.org). Continuous variables were expressed as mean ┬▒ standard deviation or median and interquartile range. Categorical variables were expressed as frequency with percentage. All continuous variables were tested for normality before statistical analysis. The Kolmogorov-Smirnov test was performed to determine the normality of parameter distribution. Comparisons between groups were performed using analysis of variance with a normal distribution and the chi-square test or FisherŌĆÖs exact test for categorical variables. Data that did not show a normal distribution were compared using the Kruskal-Wallis test. To evaluate the association between statin intensity and CKD progression, multivariable Cox regression analysis was performed. Variables that were significant in univariable analysis (P < 0.05) or clinically important were included for adjustment. The results were presented as hazard ratios (HRs) and 95% confidence intervals (CIs). Participants who were lost to follow-up were censored at the date of the last examination. For all analyses, P < 0.05 was considered significant.
Results
Baseline characteristics
The baseline characteristics of participants according to statin therapy intensity-based group are described in Table 1. Totals of 427 (39.8%), 596 (55.5%), and 50 (4.7%) participants were classified into low-, moderate-, and high-intensity statin groups, respectively. The mean age of participants was 56.0 ┬▒ 11.39 years, and 665 (62.0%) were male. The mean eGFR was 51.7 ┬▒ 26.7 mL/min/1.73 m2. Demographic data, including age, sex, smoking status, marital status, education status, income status, BMI, and BP, showed no significant differences among the groups. The most common cause of CKD in study participants was glomerulonephritis, followed by diabetes and hypertension. However, no differences were found in cause of CKD among the three groups. Regarding use of other lipid-lowering drugs, the high-intensity group was taking less ezetimibe and more fibrates than the low-intensity group. In the laboratory data, the high-intensity group showed higher level of proteinuria and lower level of serum albumin than the low-intensity group. There were no differences in lipid profiles among groups except in terms of triglyceride level; patients in the high-intensity group showed higher level of TG than those in the low-intensity group. The ASCVD risk score, Charlson Comorbidity Index, and prevalence of comorbidities such as diabetes, hypertension, coronary artery disease, congestive heart failure, and peripheral artery disease were similar among groups.
Risk of kidney disease progression according to intensity of statin therapy
During a median follow-up of 39.9 (25.4-61.6) months, 102 (23.9%), 138 (23.2%), and 15 (30.0%) renal outcome events occurred in low-, moderate-, and high-intensity groups (P for trend = 0.74), respectively. The crude incidence rate of doubling of serum creatinine, Ōēź 50% decline in eGFR, and initiation of dialysis or kidney transplantation was higher in the high-intensity group than in the low-intensity group without statistical significance (Fig. 2). However, Kaplan-Meier analysis showed no significant difference in time to first adverse kidney outcome among statin intensity groups (Fig. 3). In multivariable Cox analysis adjusted for demographic factors of age, sex, BMI, SBP, smoking status, income status, comorbidities (hypertension, diabetes, and CVDs), laboratory data (eGFR, proteinuria, and lipid profiles), and use of other lipid-lowering agents (ezetimibe or fibrates), use of high- or moderate-intensity statin was not associated with risk of CKD progression compared with use of low-intensity statin. The corresponding HRs (95% CIs) were 1.15 (0.60-2.20) and 0.97 (0.72-1.30), respectively (Table 2). In addition, the annual eGFR decline rate was not different among the three groups (-1.19 ┬▒ 0.24, -1.58 ┬▒ 0.16, and -0.16 ┬▒ 0.59 mL/min/1.73 m2/yr in low-, moderate-, and high-intensity statin groups, respectively; P = 0.06). When high- and moderate-intensity statins were grouped together, no significant association was observed between statin intensity and primary outcome (HR, 1.03; 95% CI, 0.77-1.38; Supplementary Table 2).
In addition, the association between statin intensity and change in proteinuria during follow-up was evaluated. Proteinuria level was not significantly different among statin intensity groups during the follow-up period (P = 0.64; Supplementary Fig. 1).
Subgroup analyses
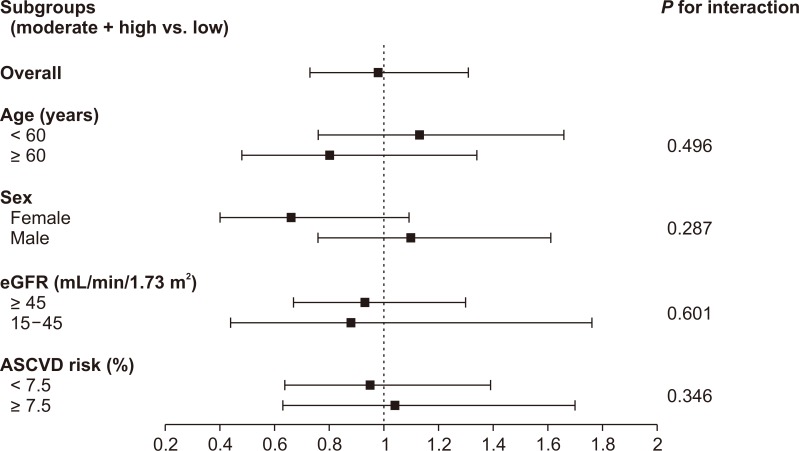
We further evaluated the association between statin therapy intensity and CKD progression in subgroups stratified by age (< 60 years vs. Ōēź 60 years), sex (female vs. male), eGFR category (15-45 vs. Ōēź 45 mL/min/1.73 m2), and ASCVD risk score (< 7.5% vs. Ōēź 7.5%). There were no significant interactions between stratified variables and statin therapy intensity group in terms of CKD progression. This result suggests that the association was consistent regardless of age, sex, eGFR, and ASCVD risk score (Fig. 4).
Discussion
In the present study, we investigated the association between statin therapy intensity and CKD progression in patients with CKD. Despite the crucial role of intensity-based statin therapy in preventing cardiovascular events, low-, moderate-, or high-intensity statin therapies were similarly associated with risk of adverse kidney outcome. This association was consistent regardless of age, sex, eGFR category, and ASCVD risk score.
Dyslipidemia is an important risk factor for adverse cardiovascular outcome in patients with and without CKD [24]. Previous meta-analyses have shown that statin therapies largely contribute to reduced atherosclerotic cardiovascular events and related mortality in patients with non-dialysis-dependent CKD [25,26]. In addition, dyslipidemia is associated with more rapid loss of kidney function in people without kidney disease. Patients with kidney disease are more likely to have hyperlipidemia, although not all patients with elevated lipid levels have kidney disease [27,28]. In experimental studies, hyperlipidemia may exacerbate preexisting kidney disease by causing direct injury to the glomerular basement membrane [29]. In contrast, statins may improve kidney function by improving endothelial function to increase renal perfusion [30]. Furthermore, statins reduce proteinuria by attenuating renal inflammation and fibrosis in the tubulointerstitium [31]. Although lipid accumulation and lipotoxicity may lead to kidney injury in experimental animal models, there is insufficient evidence supporting an effect of lipid profile abnormality on kidney function in humans [32]. Furthermore, epidemiologic studies have yielded conflicting results on the relationship between statins and kidney disease progression among patients with CKD. Several trials have suggested the beneficial effects of statins on kidney disease outcomes [33,34]. However, previous studies were based on post hoc analyses of cardiovascular benefits of statin therapy, and the effects on kidney function were modest. Moreover, studies suggesting the reno-protective effects of statins mainly included patients with prevalent CVD, and several other studies showed that statins have no effect on kidney function in CKD patients without CVD [35,36]. Therefore, statin therapy may decrease the rate of kidney function decline mainly in patients with prevalent CVD. However, the clinical significance of this effect remains unclear.
Recently, statin therapies of differing intensity are being recommended. The ACC/AHA guidelines emphasize different statin therapy intensities in patients with varying risks of ASCVD [14]. In this regard, the dose-dependent relationship between statin therapy intensity and renal outcome can be hypothesized [37]. Sanguankeo et al [12] reported that high-intensity statin therapy improved eGFR in patients with CKD compared to a control group, but moderate- to low-intensity statin therapies were not associated with improved eGFR. They also showed that LDL-C reduction had a significant association with changes in eGFR; the magnitude of eGFR increase was well correlated with decrease in LDL-C concentration. In line with our study, however, they showed no significant association between statin therapy intensity and hard study endpoints, such as 50% eGFR reduction or development of ESRD. Possible reasons for the nonsignificant association between statin therapy intensity and hard renal events in this study are suggested. First, most previous studies that reported the effects of statins on renal function were post-hoc analyses of original studies that aimed to examine the cardiovascular benefits of statin therapy. Thus, almost all study subjects had preexisting CVD. However, in the present study, only 10% of study participants had previous CVD at baseline. It is possible that the protective effect of statins might not have been pronounced in our study cohort. Hence, subgroup analysis stratified by low vs. high ASCVD risk scores was performed; however, there was still no significant relationship between statin therapy intensity and renal event. Second, the positive effect of statins on declining kidney function may be attenuated in the presence of other risk factors for CKD progression, such as high BP. Hypertension is one of the strongest risk factors for kidney function decline. A previous study showed that the beneficial effect of statins on preservation of kidney function was weaker in people with higher SBP [38]. This result suggests that other risk factors can modify the effect of statins on kidney function. Third, previous studies indicated that statin therapy may lead to unintended acute kidney injury. In particular, use of high-intensity statin therapy was associated with an increased rate of acute kidney injury diagnosis during hospital admissions [18]. Therefore, the possible harmful effect of statin therapy might have hindered the reno-protective effect of statins. Nevertheless, statins also may have pleiotropic effects favorable for reducing CKD progression, such as lowering oxidative stress, reducing inflammation, and stabilizing atherosclerotic plaques [39]. Thus, further studies are warranted to validate the effect of statins on renal outcomes.
Although we did not observe significant association between statin intensity and adverse kidney outcome, our findings remain valuable. First, it is well-known that statin therapy in patients with CKD is not as effective as in people without CKD. The reason for this is unclear, but we thought that statin intensity might modify the relationship between statin use and adverse clinical outcome in patients with CKD. This prompted us to analyze this association in depth using a cohort database involving only patients with CKD. Although we could not assert a causal relationship, our findings suggest that the lower effectiveness of statin therapy in patients with CKD may not be related to statin intensity. Second, there is concern regarding the possible harmful association of high-intensity statins with acute kidney injury [40]. However, our study showed that high- or low-intensity statin use was similarly associated with risk of CKD progression. This indicates that long-term kidney outcomes may not be affected by statin intensity.
This study has several limitations. First, due to its observational design, the causal relationship between statin therapy intensity and kidney function could not be determined. Second, patients with ESRD requiring dialysis or those who had received kidney transplantation were not included. Thus, the study results cannot be generalized to these patients. Third, only baseline statin therapy was used in the analysis; thus, the study results cannot reflect changes in statin use over time. Furthermore, changes in LDL-C level according to statin intensity could not be evaluated because patients had been treated with statin therapy before study enrollment. The beneficial effects of high-intensity statin therapy were linked to higher reduction in LDL-C level [17]. Thus, it could not be determined whether high-intensity statin therapy with a large reduction in LDL-C level has a reno-protective effect. Fourth, the proportion of participants in the high-intensity statin therapy group was relatively small. The 2013 KDIGO lipid guidelines recommend statins for patients aged Ōēź 50 years with CKD and with eGFR < 60 mL/min/1.73 m2, but it does not specify statin intensity dosing recommendations [41]. Thus, most patients with CKD take statins irrespective of dose based on statin intensity. In the present study, ASCVD risk scores were not significantly different among statin therapy intensity groups, suggesting that statins were not prescribed based on intensity-based dosing recommendations. This may have resulted in a decreased effect of statins on kidney function. Finally, the study cohort included a single ethnic group, with all participants being Korean. Thus, the results should be interpreted with caution, and our findings may not be generalized to other ethnic groups.
In conclusion, among Korean adults with CKD, we did not observe any significant association between statin therapy intensity and CKD progression. However, the findings obtained from our observational study do not provide sufficient evidence on this issue. Given the importance of treating dyslipidemia in patients with CKD, further large and well-designed randomized controlled trials are needed to clearly determine the effects of intensity-based statin therapy on kidney function.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









