


Introduction
Renal artery aneurysm and pseudoaneurysm are rare disease entities with a prevalence of 0.01â0.09% in the general population for aneurysm [1] and 1% after partial nephrectomy for pseudoaneurysm [2]. They cause pain, renal infarction, hematuria, hematoma, and death. Sometimes, they are found incidentally during diagnostic procedures such as abdominopelvic computed tomography (CT) and magnetic resonance imaging performed for diagnosing other diseases. Although aneurysms and pseudoaneurysms are asymptomatic, treating them is important, as rupture can be fatal. They arise from arterial injuries or defects which are caused by noninflammatory, inflammatory, traumatic, and genetic origins. Behçet's disease is a chronic, relapsing, multisystemic inflammatory condition. Vascular involvement, affecting vessels of any size, has been reported in 7.7â38% of patients with Behçet's disease [3]. Although venous manifestation is more common, arterial manifestation can be fatal. The most severe complications are aneurysm formation and rupture. Abdominal aorta and pulmonary artery aneurysms are common; however, renal artery aneurysms are rare. Here, we report the case of a woman with incidental renal artery pseudoaneurysm in Behçet's disease who was treated successfully with endovascular treatment.
Case report
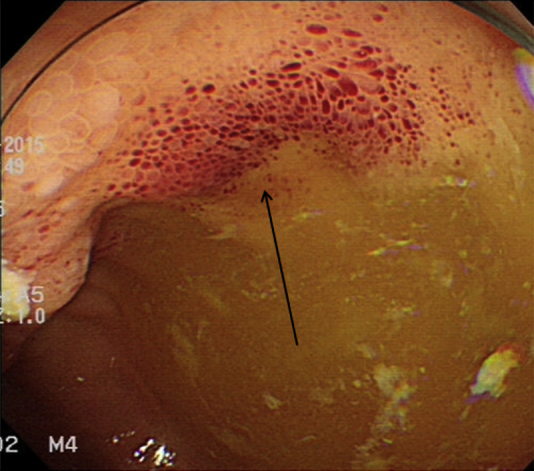
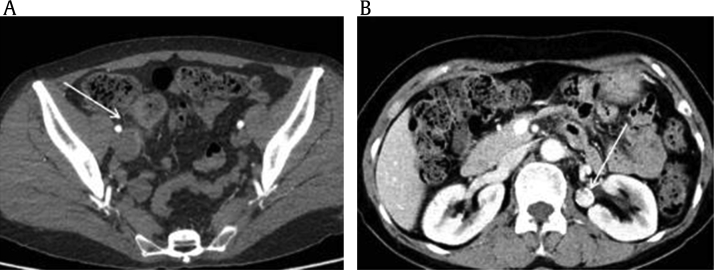
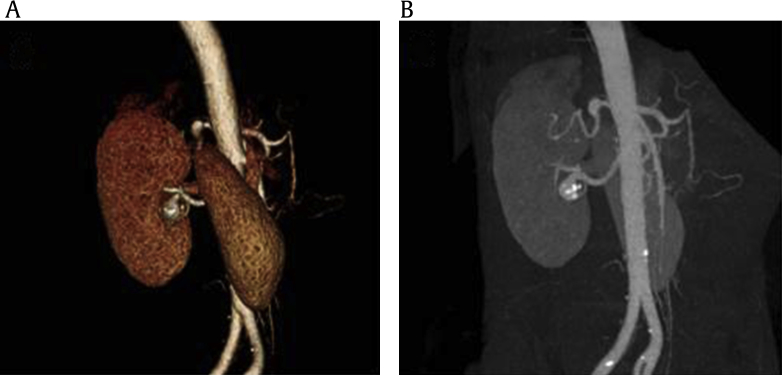
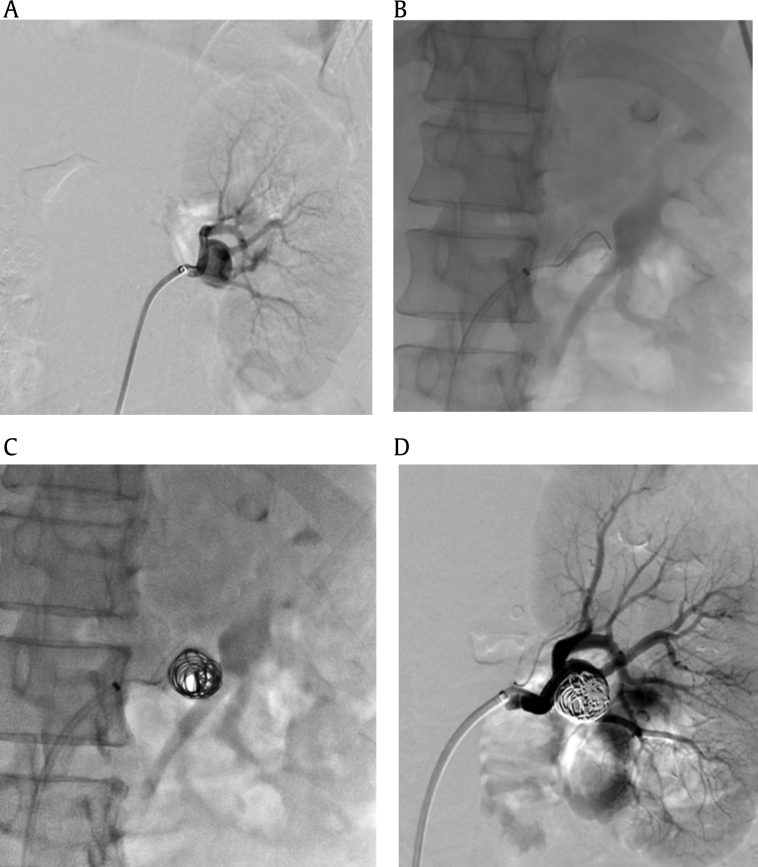
A 56-year-old woman visited the gastroenterology department with abdominal pain and bloody stool. She was previously diagnosed with Behçet's disease with recurrent terminal ileitis and oral and genital ulcer 13 years ago. She had been taking colchicine 1.2 mg and sulfasalazine 2,000 mg for a day for 3 months and antihypertensive medicine for 10 years, and her blood pressure was well controlled. Terminal ileal ulcer was detected on colonoscopy; however, there was no evidence of active bleeding (Fig. 1). At that time, her abdominal CT revealed terminal ileitis and an 18 mm-sized left renal artery saccular pseudoaneurysm with calcification (Fig. 2); she was then referred to the nephrology department. On admission, her vital signs were as follows: blood pressure, 110/60 mmHg; heart rate, 81 bpm; respiratory rate, 20 bpm; and body temperature, 36.5°C; and physical examination did not reveal any abnormalities. Her complete blood count revealed the following: hemoglobin level, 11.6 g/dL; white blood cell count, 6,440/mm3; and platelet count, 212,000/mm3. A basic metabolic panel revealed no abnormalities; her blood urea nitrogen level was 14.1 mg/dL and creatinine level was 0.72 mg/dL. C-reactive protein level was 0.11 mg/dL. Urinalysis was negative for protein, pH 5.5, 1.011 for specific gravity with no red blood cell and white blood cell on microscopic examination. A left renal artery saccular pseudoaneurysm was detected on CT angiography (Fig. 3) for which endovascular treatment was administered. There was no aneurysm or microaneurysm on contralateral renal artery. A left renal artery aneurysm measuring 15 à 18 mm was observed near the proximal part of the inferior branch on the angiogram. We inserted a wall stent (Palmaz Blue; Cordis, Miami lakes, FL, USA) measuring 5 à 19 mm and performed embolization with 6 coils (Tornado Embolization Microcoil; Cook, Bloomington, IL, USA) at the proximal inferior branch of the left renal artery (Fig. 4). There were no complications of endovascular treatment until 6 months after operation.
Discussion
Behçet's disease is a chronic inflammatory disease that is clinically diagnosed by the presence of recurrent oral and/or genital ulcer along and other mucocutaneous, ocular, vascular, and gastrointestinal lesions. Behçet's disease is the only type of systemic vasculitis that involves both arteries and veins of any size and is caused by repeated remissions and exacerbations. Although its prognosis is relatively good, it may become worse when the neurovascular and major vessels are involved. One of the types of vascular involvement is aneurysm or pseudoaneurysm. Aneurysm is a dilatation of the vessel lumen involving all 3 layers and pseudoaneurysm is a perfused hematoma contained by the adventitia and perivascular tissues that is in communication with the lumen of an adjacent artery or vein [4]. Common causes of renal artery aneurysms are fibromuscular dysplasia, atherosclerosis, and intrinsic collagen deficiencies such as EhlersâDanlos syndrome and Marfan syndrome. On the other hand, pseudoaneurysms can be caused by inflammatory and traumatic episodes, which result in disruption of the arterial wall continuity. Aneurysms and pseudoanuerysms have poor prognoses and often cause acute catastrophic hemorrhage. It is speculated that pseudoaneurysms develop in Behçet's disease because of endarteritis obliterans of the vasa vasorum and intense inflammation of media adventitia, leading to distension of the vessel due to the destruction of the media and weakening of the arterial wall [5]. The abdominal aorta is the most commonly affected site, followed by the pulmonary artery. Manifestation in other sites such as the celiac, subclavian, coronary, tibioperoneal, iliac, and ulnar arteries is rare [6], [7], [8]. Isolated renal artery aneurysm or pseudoaneurysm is very rare, especially in Korea. A search through KoreaMed and KMbase databases revealed only reported case of renal artery aneurysm. That case is different from the present case because in that case, the patient had Behçet's disease and had developed renal arterial stump aneurysm because of anastomotic dehiscence after abdominal aortic aneurysm surgery [9]. In other countries, cases of renal artery aneurysm with renal infarction caused by microaneurysm in the segmental artery [10], perirenal hematoma with arcuate artery microaneurysm [11], and left ventricular aneurysm with ruptured renal artery pseudoaneurysm have been reported [12]. However, the case presented in this report is also rare because it involved isolated extraparenchymal renal artery pseudoaneurysm without any complication in a patient with Behçet's disease. The cause of the patient's renal pseudoaneurysm may be debatable because although she had a long history of hypertension, her blood pressure was well controlled with a single medication (amlodipine 5 mg/day), and end-organ damage and renovascular hypertension were not present. Furthermore, atherosclerosis is rare in Behçet's disease than in other autoimmune diseases [13], and there was no evidence of atherosclerosis in other arteries on CT scan. Hence, we thought that the calcification of the aneurysm indicated repeated vascular injury and recovery, which is the main characteristic feature of Behçet's disease. Pseudoaneurysms caused by Behçet's disease are treated at the earliest opportunity because they present a high risk of rupture that does not depend on the size of the aneurysm unlike in atheromatous aneurysms [14]. Surgical repair is the standard method used for treatment of organ-threatening aneurysmal dilatation, stenosis, and obstruction. The most frequent postoperative complication is anastomotic dehiscence, and therefore, controlling preoperative systemic inflammation is important. Endovascular treatment of arterial pseudoaneurysms in Behçet's disease is now effective and safe with acceptable vascular complications. However, there are some limitations of renovascular intervention because of the complexity and size of the renal arteries. Despite limitations, coil embolization can be performed in cases of saccular aneurysms in the main renal artery [15]. In our case, although the aneurysm was located near the renal artery bifurcation, we performed coil embolization of the renal artery aneurysm successfully. It was enough to do embolization with coil only; however, the risk of renal infarction during procedure was high because of its location, stent-assisted coil embolization was done. Therefore, we hope to share our experience with other clinical physicians.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









