Comparison of clinical outcomes between ABO-compatible and ABO-incompatible spousal donor kidney transplantation
Article information
Abstract
Background
Kidney transplantation (KT) is the treatment of choice for end-stage renal disease patients. The spouse is a major donor in living KT. Clinical outcomes of spousal donor KT are not inferior to those of living related donor KT. In this study, we compared clinical outcomes between ABO-compatible (ABOc) and ABO-incompatible (ABOi) spousal donor KTs.
Methods
Thirty-two cases of spousal donor KT performed from January 2011 to August 2013 were analyzed retrospectively. Twenty-one ABOc KTs and 11 ABOi KTs were performed. We investigated patient survival, graft survival, acute rejection, graft function, and complications.
Results
During follow-up, patient and graft survival rates were 100% in both groups. There were no significant differences in the incidence of delayed graft function, acute rejection, and the change in graft function between the 2 groups. Medical and surgical complications were not significantly different between the groups.
Conclusion
The clinical outcomes of ABOc and ABOi spousal donor KTs were equivalent. In ABOi KT, an emotionally motivated spousal donor KT may be a good alternative to the problem of the absolute shortage of kidney donations.
Introduction
Kidney transplantation (KT) is the treatment of choice for end-stage renal disease (ESRD) patients [1]. With the global increase in ESRD patients with chronic diseases such as diabetes mellitus, hypertension, and chronic glomerulonephritis [2], the need for KT increases annually. However, the shortage of kidney donors is still a critical problem. In Korea, the number of ESRD patients on the waiting list was 14,448 as of December 2013, and only 1,759 patients received KT during 2013 [3]. To solve this problem, living unrelated donor KT, in addition to living related donor (LRD) KT, deceased donor KT, and even extended criteria donor KT are currently being performed [4]. Especially, to compensate for the shortage of kidney donations in Korea, ABO-incompatible (ABOi) KT was first performed in 2007 [5]. The development of immunosuppressive agents and pretreatment methods, such as plasmapheresis, and the use of intravenous immunoglobulin and rituximab have made ABOi KT possible [6]. Several studies reported that outcomes of ABOi KT were not inferior to those of ABO-compatible (ABOc) KT [7], [8], [9]. Along with the trend toward a smaller family size comprising spouses and children in contemporary society, the rate of spousal donor KT has increased. Because a spousal donor currently accounts for most ABOi KT cases, the spouse is the most important donor in living KT [10], [11], [12]. It is known that clinical outcomes of ABOc spousal donor KT are not different from those of ABOc LRD KT [10].
In this study, we compared the clinical outcomes of ABOc KT with those of ABOi KT with a spousal donor.
Methods
Patient characteristics
We retrospectively analyzed the medical records of 143 KTs performed at Dongsan Medical Center, Keimyung University School of Medicine, between January 2011 and August 2013. This study was approved by the Institutional Review Board of Keimyung University School of Medicine (2015-07-053).
Immunosuppression protocols
We performed KT when the removal of donor-specific anti-human leukocyte antigen (HLA) antibodies was observed with serial anti-human globulin complement-dependent cytotoxicity (AHG-CDC) cross-matching. Basiliximab (20 mg on Days 0 and 4, Simulect; Novartis, Basel, Switzerland) was administered for induction of immunosuppression for all recipients of ABOc and ABOi KTs, except for HLA–identical patients. The maintenance immunosuppressive regimen consisted of tacrolimus (Prograf; Astellas Pharma Inc., Toyama, Japan), corticosteroid, and mycophenolate mofetil (MMF, CellCept; Hoffmann-La Roche Inc., Nutley, NJ, USA).
In ABOc KT recipients, tacrolimus (0.05 mg/kg twice a day), corticosteroid (15 mg twice a day), and MMF (750 mg twice a day for weight < 60 kg or 1,000 mg twice a day for weight ≥ 60 kg) were administered on pretransplant Day 2. A trough level of tacrolimus was maintained at 5–10 ng/mL for a month after transplantation and 3–8 ng/mL thereafter. Methylprednisolone was administered at a dose of 500 mg twice a day on the day of the operation and 50 mg twice a day on post-transplant Day 1. Prednisolone (30 mg/d) was administered starting on post-transplant Day 2 for 2 weeks and was tapered to a dose of 10 mg/d by 3 months after transplantation.
In ABOi KT recipients, we excluded the candidate when the initial titer of anti-A/B antibody was greater than 1:256. A single dose of rituximab (200 mg/m2; Roche Pharma AG, Reinach, Switzerland) was administered 2 weeks before KT. MMF was administered 12 days before KT (750 mg twice a day for weight < 60 kg or 1,000 mg twice a day for weight ≥ 60 kg). Tacrolimus (0.05 mg/kg twice a day) and prednisolone (15 mg twice a day) were administered 10 days before KT. A trough level of tacrolimus was maintained as for ABOc KT. All ABOi KT recipients underwent double-filtration plasmapheresis (1.5 plasma volumes exchanged with 5% albumin) every other day, with a final preoperative total plasma exchange (with AB blood type fresh frozen plasma), until anti–blood-type antibody titer was less than or equal to 1:8 at the time of KT. After individual plasmapheresis, intravenous immunoglobulin (100 mg/kg) was administered.
All patients received preventive ganciclovir (2.5 mg/kg twice a day) against cytomegaloviral (CMV) infection for 14 days after KT, trimethoprim–sulfamethoxazole (80 mg/400 mg twice a day) against Pneumocystis jiroveci pneumonia, and oral fluconazole (5 mL once a day) against fungal infection for 6 months.
In this study, we investigated patient and graft survival rates, delayed graft function (DGF), graft function as the change in estimated glomerular filtration rate (eGFR), acute rejection, and medical and surgical complications after ABOc and ABOi KT with a spousal donor during the follow-up period.
Demographic and clinical data
Baseline characteristics of the study populations included donor and recipient age at KT, donor-to-recipient relationship, cause of ESRD, comorbidity, type and duration of renal replacement therapy (RRT), history of KT, number of HLA mismatches, and primary immunosuppressant.
Statistical analyses
We analyzed data using the Student's t test for continuous variables and chi-square test for categorical variables. Continuous variables are presented as the means ± standard deviation, and categorical variables are expressed as numbers and percentages. Analyses of patient and graft survival were performed using the Kaplan–Meier method with log-rank test. Nonparametric tests for comparisons between the 2 groups of nonnormal distribution were performed using the Mann–Whitney test. A P values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS (version 18.0, SPSS Inc., Chicago, IL, USA) statistical software package.
Results
Baseline characteristics of the ABOc and ABOi groups in spousal donor KT
Among 32 spousal donor KTs, 21 kidneys (31.3%) were from ABOc donors and 11 (57.9%) from ABOi donors. There were 12 (57.1%) wife-to-husband and 9 (42.9%) husband-to-wife ABOc KTs, and 9 (81.8%) and 2 (18.2%) ABOi KTs, respectively (Fig. 1). All the wives as recipients had a history of two pregnancies except 1 person. The mean ages of donors and recipients in ABOc KT were older than those in ABOi KT, but there were no significant differences between the groups (Table 1). Among the causes of ESRD, chronic glomerulonephritis was the most common cause in both ABOc KT [15 (71.4%)] and ABOi KT [8 (72.7%)], but there were no significant differences between the groups. The most common type of RRT before KT in ABOc and ABOi patients was hemodialysis [14 (66.7%) and 8 (72.7%), respectively]. The mean numbers of HLA mismatches in ABOc and ABOi KTs were 3.4 ± 1.5 and 4.4 ± 0.8, respectively, and the difference was significant (P = 0.026). The primary immunosuppressive agent in all patients was tacrolimus (21 in ABOc KT), with cyclosporine used in only 1 ABOi KT patient.
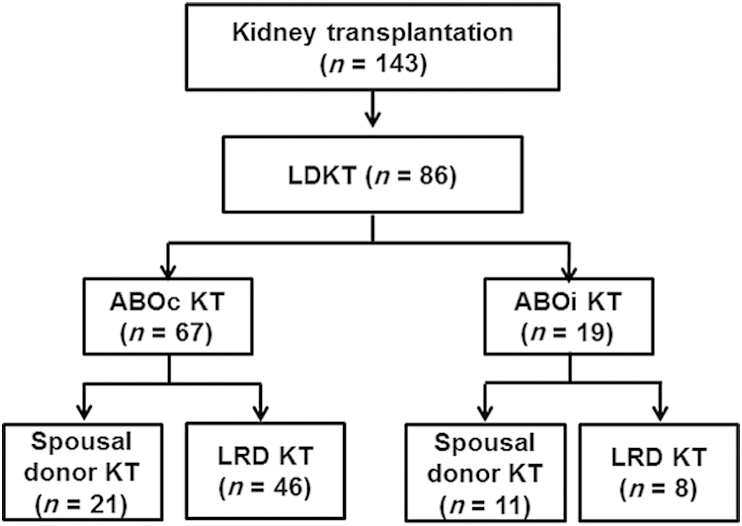
Flow chart of selection for study population.
ABOc, ABO compatible; ABOi, ABO incompatible; KT, kidney transplantation; LDKT, living donor kidney transplantation; LRD, living related donor.

Baseline characteristics of the ABOc and ABOi groups in spousal donor KT
Changes in anti-A/B antibody titer and distribution of ABO type of ABOi spousal donor KT
Changes in anti-A/B antibody titer in ABOi spousal donor KT are shown in Fig. 2. The ABO type of ABOi spousal donor KT patients is shown in Fig. 3A. The range of initial anti-A/B antibodies was from 1:2 to 1:128 (Fig. 3B). The median titer of anti-A/B antibody was 1:32, 1:4, and 1:2 initially, at the time of KT, and 1 week after KT, respectively. The median number of plasmapheresis treatments was 5 (0–6). All patients satisfied the criterion of anti–blood-type antibody titer less than or equal to 1:8 at the time of KT, and the titers remained less than or equal to 1:8 until 1 month after KT.
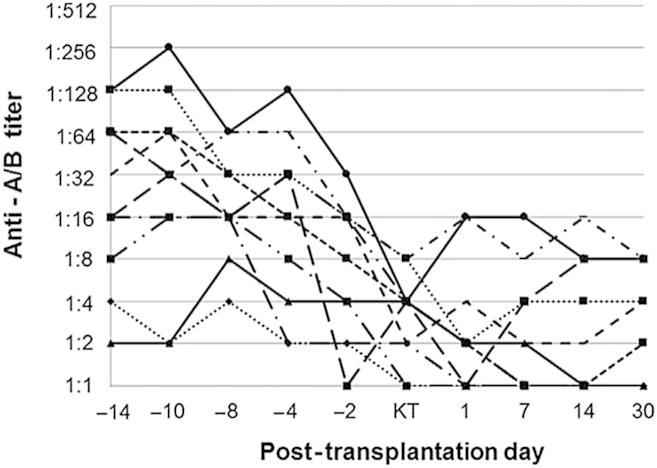
Changes in anti-A/B antibody titer in ABOi spousal donor KT.
ABOi, ABO incompatible; KT, kidney transplantation.
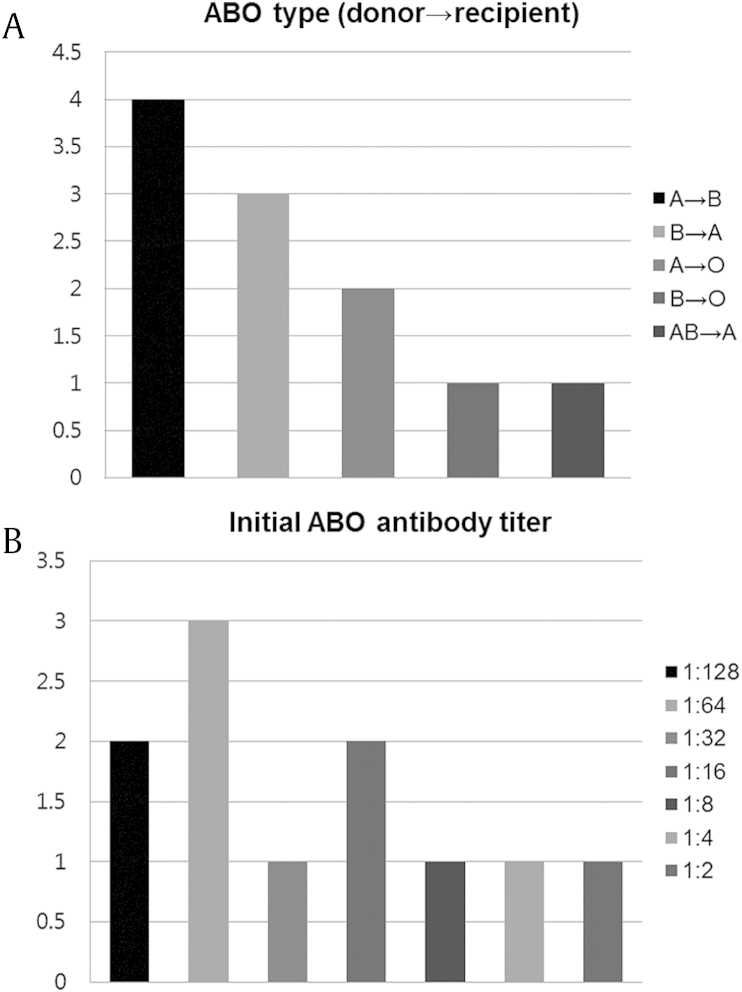
The distribution of (A) ABO type and (B) initial anti-A/B antibody titer in ABOi spousal donor KT.
ABOi, ABO incompatible; KT, kidney transplantation.
Patient and graft survival rates, DGF, renal allograft function, and acute rejection
During the follow-up period, overall patient and graft survival rates were 100% in both groups (Table 2). In ABOc KT, 1 (4.8%) DGF occurred. In ABOi KT, 1 (9.1%) acute antibody-mediated rejection (AAMR) occurred and was verified by renal biopsy. Panel-reactive antibody Class I positivity was 0% and Class II was 80%, but HLA donor-specific antibodies (DSAs) were not tested for. AAMR occurred 9 months after KT because of the persistent low tacrolimus level after CMV gastritis. One week, 1 month, 3 months, 6 months, and 1 year after KT, eGFRs were 79.47 ± 31.73, 70.24 ± 17.41, 62.73 ± 9.78, 64.90 ± 15.53, and 66.01 ± 20.85, respectively, for ABOc KT, and 93.32 ± 28.50, 82.46 ± 21.18, 72.01 ± 19.25, 66.44 ± 16.93, and 67.22 ± 23.20 for ABOi KT, but there were no significant differences between the groups.

Patient and graft survival and post-transplant renal function in spousal donor KT
Complications in spousal donor KT
CMV infection occurred in 4 (19%) ABOc KT and 2 (18.2%) ABOi KT patients (Table 3). Other viral, bacterial, and Candida infections occurred in 2 (9.5%), none, and 1 (4.8%), and 2 (18.2%), 1 (9.1%), and none, in ABOc KT and ABOi KT patients, respectively. Those were varicella-zoster virus, herpes zoster virus, and herpes simplex virus infections. There were no significant differences between the groups. New-onset diabetes after transplantation occurred in 4 ABOc (19%) and 4 ABOi patients (36.4%), but this difference was not statistically significant. Hyperlipidemia occurred in 7 ABOc (33.3%) and 2 ABOi patients (18.2%), but there was no significant difference. Surgical complications such as bleeding, lymphocele, and urinoma occurred in 4 ABOc (19%) and 3 ABOi patients (27.3%), but this difference was not statistically significant.

Complications in spousal donor KT
Discussion
In this study, we demonstrated that KT from an ABOi spousal donor was equivalent to that from an ABOc spousal donor in terms of patient and graft survival, allograft function, and acute rejection. These results are in the extension of the previous studies such as the comparison of spousal donor KT and LRD KT in ABOi KT [13] or that of ABOc KT and ABOi KT [14].
Several studies reported that spousal donor KT showed lower HLA typing compatibility than deceased donor KT [10], but patient and graft survival rates were higher. Although the age of donors and recipients in spousal donor KT was greater than that in LRD KT, the results of transplantation were not significantly different. Several studies demonstrated that the incidence of infection and bleeding was higher in ABOi KT than ABOc KT because of the desensitization process before KT [15], but there were no significant differences in patient and graft survival between the groups.
In our study, recipient age, donor age, cause of ESRD, comorbidity, RRT type, duration of RRT, and the frequency of KT were not significantly different between ABOc and ABOi KT with a spousal donor. It is known that HLA mismatching is an important factor affecting graft survival in KT recipients [16], but the development of immunosuppressive agents has reduced the influence of HLA mismatching on graft survival in KT recipients. Several studies showed that spousal donor KT had low HLA matching compared with cadaveric donor KT but had a higher graft survival rate [17]. In our study, HLA mismatching was significantly higher in ABOi than in ABOc KT but was not significantly associated with the graft survival rate. However, longer follow-up is needed.
There were no significant differences in patient and graft survival between ABOc and ABOi KTs. In ABOc KT, 1 (4.8%) DGF occurred. Blood pressure decreased with the decrease in the hemoglobin level a day after KT, and allograft biopsy showed acute tubular necrosis. ABOi spousal donor KT did not show a higher frequency of DGF compared to ABOc KT. This was consistent with several studies showing that spousal donor KT did not have a higher rate of DGF compared with LRD and cadaveric KTs and that ABOi KT did not have a higher rate of DGF compared with ABOc KT. On 1 week, 1 month, 3 months, 6 months, and 1 year after KT, the mean eGFR was not significantly different between ABOc and ABOi KT.
It is known that there is no difference in the incidence of acute rejection between LRD and spousal donor ABOc KTs [18]. However, LRD and spousal donor ABOi KTs had a higher incidence of AAMR, especially in the first 2 weeks after KT, and was associated with the change in anti-A/B antibody titer after KT [19], [20], [21]. In our study, 1 person had AAMR in ABOi KT. At that time, anti-A/B antibody titer showed no interval change after KT. It could be surmised that the cause of AAMR was HLA DSA, not anti-A/B antibody. The results of our study differed from others reporting that the major antibody for AAMR in ABOi KT was either anti-A/B antibody or anti-HLA antibody, but the latter had greater influence on graft outcome [5].
The medical and surgical complications in spousal donor KT are reported in Table 3. ABOi KT had a higher incidence of viral infection because of intensified immunosuppression and bleeding complications after pretransplantation treatment [21]. Although intensive desensitization for anti-A/B antibody in ABOi KT was performed, there were no significant differences in the prevalence of CMV and other infections between ABOc and ABOi KTs. There were also no significant differences in metabolic complications such as new-onset diabetes after transplantation and hyperlipidemia between ABOc and ABOi KTs. ABOi KT tended to have more frequent surgical complications such as lymphocele or hematoma than ABOc KT, but the difference was not significant. This was not correlated with the frequency of plasmapheresis.
This study has several limitations. First, our study is retrospective, and the number of patients is limited. Therefore, it is possible that unrecognized selection bias may affect the results. Second, because the follow-up period is short, there are limitations in evaluating the patient and graft survival rates. Third, there was no treatment for pretransplant desensitization for patients with a high panel-reactive antibody level because of lack of information about DSA. In ABOi KT, only anti-A/B antibody titer was confirmed, and ABOi KT in highly sensitized patients was not considered. Finally, in our study, ABO titer was lower than that in the other studies, so it could not be the representative of current ABOi transplant, and it was the reason for lower incidence of postoperative complications.
In conclusion, KT from an ABOi spousal donor was equivalent to that from an ABOc spousal donor in terms of patient and graft survival, allograft function, and acute rejection in our study. As nuclear families and marriage age are both increasing, it will be difficult to find suitable LRDs and living unrelated KT donors. A genetically incompatible but emotionally motivated spousal donor can be a good alternative to solve the absolute shortage of kidney donations. Spousal donors already account for most ABOi KT currently performed and could be an important source of donor kidneys for both ABOc and ABOi KTs.
Conflicts of interest
All authors have no conflicts of interest to declare.