Type 1 primary hyperoxaluria in a male infant
Article information
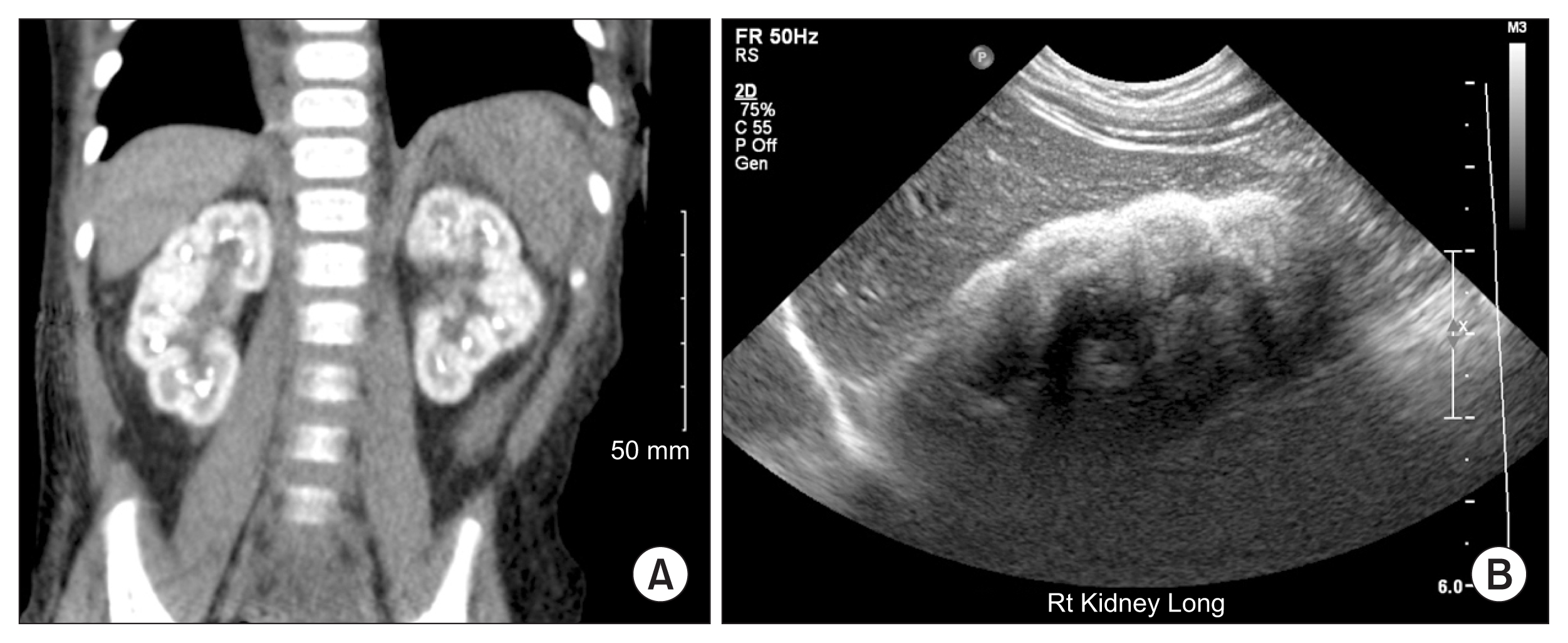
An 8 month old term, previously healthy, male presented with poor feeding, respiratory distress and decreased urine output. He was noted to be in the 1st percentile for weight, and 60th percentile for height. At admission he was hypertensive with systolic blood pressures ranging from 107–124 mmHg and diastolic pressures of 66–72 mmHg. Physical exam was remarkable for fussiness and decreased musculoskeletal tone for age. Labs demonstrated hemoglobin 4.5 g/dL, sodium 121 mmol/L, potassium 7.5 mmol/L, blood urea nitrogen 239 mg/dL, serum creatinine of 15.4 mg/dL, calcium 6.8 mg/dL, and phosphorus 8.3 mg/dL. A non-contrast computed tomographic scan revealed small kidneys with diffuse cortical nephrocalcinosis bilaterally and a renal ultrasound demonstrated increased cortical echogenicity bilaterally (Fig. 1). The right kidney measured 5 cm and the left kidney measured 4.9 cm. The mean renal length for a patient this age is 6.2 cm with a standard deviation of 0.5 cm. Serum oxalate level was 110 μmol/L and alanine-glyoxylate aminotransferase gene analysis confirmed the diagnosis of type 1 primary hyperoxaluria. Given the severity of the disease, he required both hemodialysis and peritoneal dialysis and was transferred to a referral center where he underwent staged liver and renal transplants. Primary hyperoxaluria is a rare inborn error of metabolism that leads to kidney damage through hepatic production of excess oxalate. Excess oxalate will deposit in the kidney leading to nephrocalcinosis and in this case renal failure.
Imaging findings
(A) Coronal view on non-contrast computed tomographic scan reveals diffuse nephrocalcinosis bilaterally. (B) Longitudinal view of the right kidney on ultrasound demonstrating increased cortical echogenicity.
Notes
Conflicts of interest
All authors have no conflicts of interest to declare.