



Introduction
Kidney disease has been recognized as a crucial public health concern due to the increased risk of early death, poor quality of life, as well as the high cost of treatment [1–3]. The Global Burden of Disease 2019 study estimated that 1.43 million deaths and 41.5 million disability-adjusted life-years were attributable to chronic kidney disease (CKD; defined as an estimated glomerular filtration [eGFR] less than 60 mL/min per 1.73 m2), with increases of 28.8% and 20.1% since 2010, respectively [4]. In South Korea, approximately 11% of adults (around 4.6 million people) were estimated to have CKD in 2017, and the total medical care expenses for CKD were estimated at 1,707 billion Korean won (about $1.3 billion) [5]. In the United States, about 15% of adults were estimated to have CKD in 2021 [6], and the total Medicare fee-for-service spending for beneficiaries with CKD exceeded $100 billion in 2018 [7].
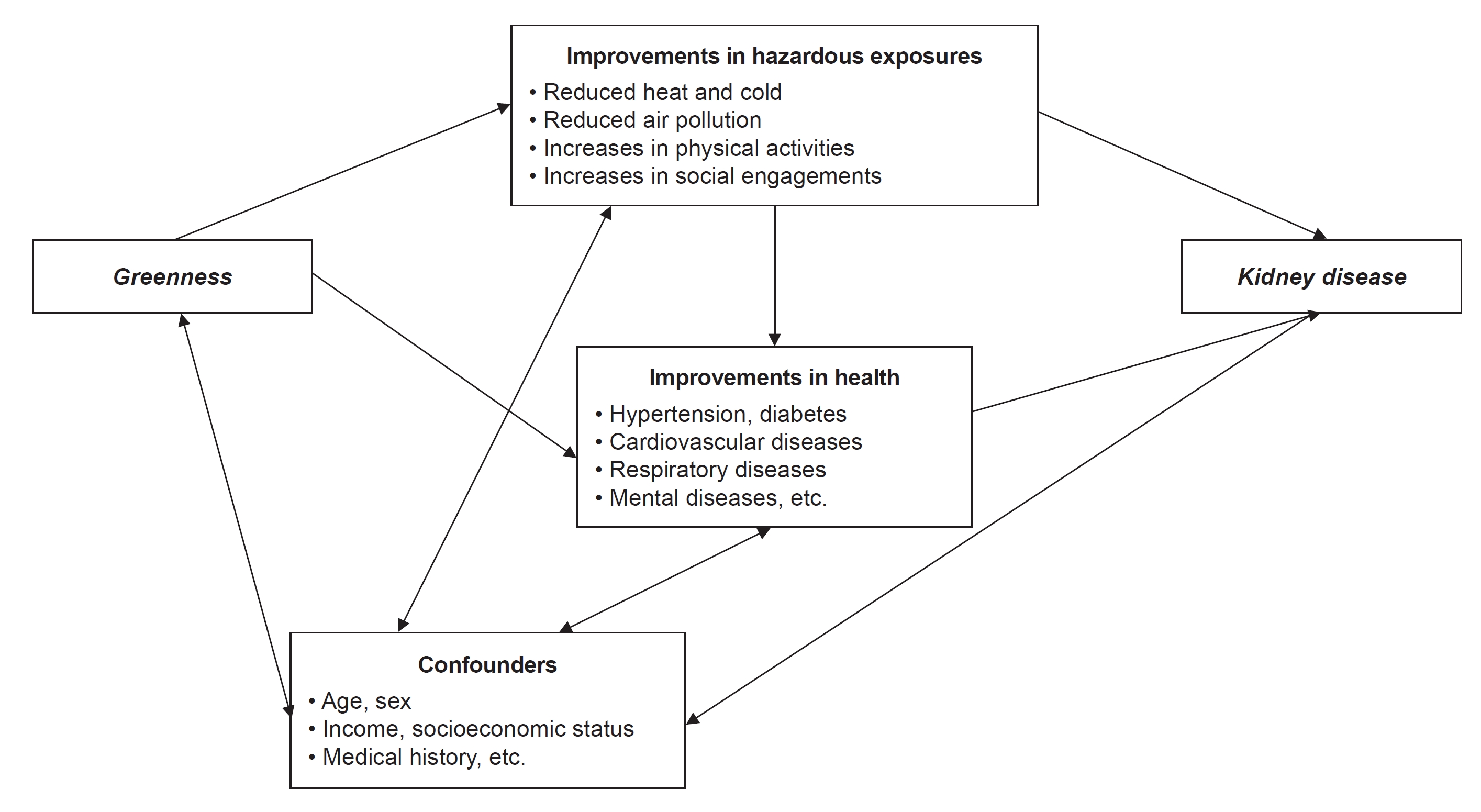
Recently, numerous studies have consistently reported the health benefits of green space, especially in relation to circulatory and endocrine diseases, which are major risk factors for kidney disease. Previous studies have reported that higher exposure to greenness may be related to a lower risk of hypertension, diabetes, and cardiovascular diseases, by increasing physical activities and social engagements [8–10] and reducing noise, extreme temperatures, and air pollution exposures [11,12]. In addition, greenness may alleviate air pollution concentration and extreme temperature events [13,14], and recent epidemiological studies identified that exposure to air pollution and extreme temperatures are associated with kidney diseases [3,15–18]; these results imply that reduced air pollution and extreme temperature events by green space can be directly or indirectly linked to the reduced risk of kidney diseases (Fig. 1). Despite these plausible mechanisms, however, studies on the relationship between greenness and kidney disease were limited [19].
In this review, we discuss the epidemiological evidence on the contribution of greenness exposures to kidney diseases. We also suggest important findings and limitations of previous studies and propose points that should be carefully addressed in future studies to reduce some of the knowledge gaps.
Epidemiological studies on greenness and kidney diseases
A literature search was performed using electronic databases PubMed, MEDLINE, Google Scholar, and Web of Science for published studies from 1990 to March 2023. We searched for relevant studies using the keywords ‘greenness and kidney disease,’ ‘green space and kidney disease,’ ‘open space and kidney disease,’ ‘green and kidney disease,’ and ‘green and chronic kidney disease,’ limiting the search to research articles addressing human and published in English. Finally, we summarized a total of seven studies (Table 1).
Greenness indices in epidemiological studies
In general, previous epidemiological studies measured a level of residential greenness using two representative satellite-based vegetation indices: normalized difference vegetation index (NDVI) and enhanced vegetation index (EVI). The NDVI is calculated as the difference between near-infrared reflectance (NIR) and red reflectance (RED) divided by their sum: NDVI = (NIR – RED) / (NIR + RED) [20]. Thus, the calculated NDVI ranges from –1 (non-vegetated areas) to +1 (full-vegetated areas) with higher values indicating denser vegetation. The concept and calculation procedure of EVI is similar to NDVI; however, EVI corrects potential distortions in the reflectance due to the particles in the air, ground cover below the vegetation, and canopy background noise, and it is more sensitive in areas with dense vegetation [21]. The equation of EVI is as follows: EVI = G × [(NIR – RED) / (NIR + C1 × RED – C2 × BLUE + L)]. G is a gain factor, and BLUE is the reflectance in the blue band measured by a satellite. L is the canopy background adjustment, and C1 and C2 are the coefficients of the aerosol resistance terms using the blue and red bands. In other words, EVI indicates a ratio between RED and NIR values, while reducing the background and atmospheric noises, thus the valid range is –1 to +1, with higher values meaning higher vegetation [22].
Literature review
To our knowledge, a study by James et al. [23] in 2016 first suggested the potential association between greenness and kidney disease. From the Nurses’ Health Study prospective cohort in the United States with 108,630 female participants from 2000 to 2008 (627,008 person-years), the study found that women living in areas with higher greenness showed lower mortality risk, with a hazard ratio (HR) of 0.63 (95% confidence interval [CI], 0.38–1.04) for a 0.1 increase in an average (January, April, July, and October) NDVI in the 250-m areas around each participant’s address.
Since 2019, studies showing the linkage between exposure to green space and the prevalence/incidence of kidney disease have begun to emerge [24]. A cross-sectional study in New Taipei City including 21,656 participants reported that the association between proximity to open space (majorly consists of green space) and adult renal function, with an odds ratio (OR) of 1.071 (95% CI, 1.007–1.138) for 100-m increase in a distance to open space.
In 2021, a multihospital-based prospective cohort study in South Korea examined the association between residential greenness and clinical outcomes of CKD patients [25]. The study constructed a large-scale cohort including 64,565 patients diagnosed with CKD from multiple metropolitan hospitals, and an average NDVI during the summer (June to August) corresponding to each participant’s residential address was used as an exposure to green space. For CKD patients, HRs were 0.96 (95% CI, 0.93–1.00; mortality) and 1.01 (95% CI, 0.98–1.04; progression to end-stage kidney disease [ESKD]) for 0.1 increase in NDVI (1,250-m buffer). Mortality of ESKD patients showed an evidently negative association with NDVI (1,250-m buffer) with an HR of 0.91 (95% CI, 0.87–0.97).
In 2022, two cross-sectional studies on CKD and green space were conducted in East Asia. Liang et al. investigated the relationship between residential NDVI and the presence of CKD based on the China National Survey of Chronic Kidney Disease with 44,876 individuals from 2007 to 2010 [26]. They found a negative association between all-season NDVI and CKD presence with an OR of 0.79 (95% CI, 0.73–0.86) for 0.26 (an interquartile range) increase in NDVI. Chien et al. [27] also performed an ecological study including 40,375 participants older than 30 years from the health screening program from 2007 to 2009 in the Metropolitan area in New Taipei City. They defined the urban open green space incorporating parks, green, plazas, public schools, and sports venues, as exposure to green space, and found the OR of CKD prevalence comparing the distance to small public urban open space over 200 m and 200 m or less was 1.14 (95% CI, 1.06–1.24).
In 2023, two cohort studies on greenness and kidney disease were published. A cohort study for electricity generating authority of Thailand employees with 2,022 participants aged 25 to 55 years in the Bangkok Metropolitan region showed that the interquartile increase in all-season NDVI was related to a higher eGFR, with 1.03% increase in eGFR (95% CI, 0.33–1.71) [28]. However, they did not find an association between eGFR and the EVI, which is an optimized satellite-driven vegetation index that corrects distortions in the reflectance [21].
Another cohort study was performed in Massachusetts, the United States. Lee et al. [19] constructed a longitudinal retrospective cohort including 1,462,949 Medicare beneficiaries living in Massachusetts from 2000 to 2016 (9.8 million person-years). This study used annual-average EVI for each beneficiary’s residential zip code as exposure and the first hospital admission for kidney diseases (total kidney disease, CKD, and acute kidney injury [AKI]) as outcome variables based on the International Classification of Diseases diagnostic codes. They found a negative association between greenness and the first hospitalization for the total kidney disease (HR, 0.95; 95% CI, 0.93–0.97), and the association was more pronounced in AKI (HR, 0.94; 95% CI, 0.92–0.97) compared to CKD (HR, 0.98; 95% CI, 0.95–1.01).
Discussion
This study reviewed a total of seven epidemiological studies on greenness and kidney disease. Although there were differences in statistical significance, all studies showed a beneficial association between higher exposure to green space and kidney disease. NDVI, a satellite-based vegetation index, was majorly used to measure exposure to greenness, and the prevalence or incidence of CKD was addressed as a kidney disease outcome.
As mentioned in the Introduction section, higher exposure to green space can alleviate the risk of kidney disease by increasing physical and social activities [8–10] and reducing environmental hazards such as air pollution and heat [11,12]. Previous studies identified that decreased physical activities and poor mental health may be associated with lower kidney function [29–31]. Furthermore, recent epidemiological studies consistently reported that exposure to extreme temperatures and air pollution was associated with a higher risk of kidney disease. Cohort studies in the United States reported that exposure to air pollution and heat increases the risks of incident CKD [17,18] or hospitalization for CKD [15] and AKI [19,32]. Korean studies based on the National Health Insurance System also showed that exposure to heat and air pollutants increases hospital admissions related to kidney disease [16,33]. Furthermore, previous studies suggested that the beneficial effects of green space on cardiovascular diseases [12,34], which are major causes of kidney diseases, should be majorly addressed in the beneficial roles of greenness on kidney health [19,25]. These results from multiple studies support biological mechanisms and epidemiological evidence of the beneficial effects of greenness on kidney health.
Nevertheless, several points should be discussed further. First, previous studies have respective limitations in relation to their study design. Relevant studies in Taiwan and China [24,26,27] were cross-sectional studies, which are limited in assessing the association between exposure and incidence of health outcomes [35]. James et al. [23] designed the study to examine the association between green space and various causes of mortality, not only for kidney disease-related deaths. The cohort study of Park et al. [25] was based on a large-scale prospective cohort, but covered patients enrolled at metropolitan hospitals, thus there were limitations in addressing nonmetropolitan areas, particularly rural areas which are generally more vulnerable to medical services [36]. Paoin et al. [28] also conducted a prospective cohort study; however, their study included only employees in a certain company with limited age distribution (25 to 55 years), thus the generalizability of the study result may be less than in other population-based or multilocation cohort studies. The study by Lee et al. [19], which is the latest in this review, performed a population-based cohort with the largest sample size (1.4 million beneficiaries) to achieve more generalizable results on greenness and kidney disease. Nevertheless, because this study was based on a retrospective cohort in Massachusetts based on Medicare claim data, it was limited in reflecting other regions in the United States and addressing sufficient individual-level variables that might be crucial confounders [19].
Second, indices for greenness exposure that previous studies used were heterogeneous among studies, and evaluations for association with kidney disease were also sensitive to the greenness indices. Most of the studies in this review used NDVI [23,25–28], which is a standardized satellite-based index based on reflectance. However, measuring NDVI can be sensitive to distortions in the reflectance caused by particles in the air, ground coverage below the vegetation, and areas with a large amount of chlorophyll [21], thus it might be not optimized in certain circumstances. Paoin et al. [28] showed that the association with eGFR differed from the results of NDVI when EVI (that corrects the limitations of NDVI) was used as exposure. Furthermore, we should note that different buffer sizes to measure NDVI can increase the uncertainty of association assessment. Studies in this review used different buffer sizes: 250 m, 1,250 m [23,25], and 1,000 m [26]; and the evaluated association between greenspace and kidney outcomes was not robust to the buffer sizes [25]. Therefore, various sensitivity analyses and further studies to find the optimal greenness index and buffer sizes are required.
Third, most of the studies in this review addressed CKD or gradual changes in eGFR as kidney outcomes. This is a common characteristic in epidemiological studies regarding greenness as well as air pollution [3,19] because the effects of greenness are generally considered gradual effects [11]. However, interestingly, a previous study found that the association with greenness was more evident in AKI outcomes than in CKD outcomes and conjectured that reducing extreme temperature events by greenness can be related to AKI, which is an acute event [19]. This study suggested dehydration which is one of the major risk factors of AKI [33,37] and the well-known association between short-term exposures to extreme temperatures and hospitalization for heart failures, respiratory events, and urinary tract infections [38,39] might play an important role to explain the relationship between greenness and AKI. Therefore, future studies should address various kidney outcomes that are potentially associated with greenspace based on plausible mechanisms.
Fourth, potentially different exposure levels and health effects of green space depending on socioeconomic characteristics should be addressed importantly in future studies. Many studies in this review were performed in urban areas [24,25,27,28], thus there is a knowledge gap in explaining whether the beneficial effects of green space exist in rural areas. In addition, urbanicity is closely related to socioeconomic and environmental status as well as demographic compositions [40]. In general, it could be expected that the population living in urban areas showed higher average socioeconomic status (e.g., income) and levels of medical services, which may be beneficial for kidney health [19]. Previous studies reported that higher socioeconomic status populations are more likely to live in areas with higher levels of health-promoting greenspace (such as urban parks that can increase recreational and physical activities in neighborhoods) [41,42], and a previous study also showed that the beneficial effects of green space on kidney disease were more prominent in people with higher socioeconomic status than in people with lower socioeconomic status [19]. Concurrently, however, urban areas generally have higher air pollution levels and extreme heat events [43], and in some areas, urban areas also showed a larger population % below the poverty level and lower accessibility to healthcare services due to the large amounts of population [44]. A recent study in Massachusetts also showed that the beneficial impacts of green space on kidney disease were observed in both urban and rural areas (the differences were not statistically significant) and mentioned that the results should be interpreted carefully, in relation to the complexity of urbanicity [19]. Thus, the urban-rural disparities in relation to greenness and kidney disease should be examined in-depth in the future.
Fifth, most of the relevant studies were performed in Asian regions [24–28], thus more various study regions should be addressed to bring more generalizable effects of greenness. In particular, most studies reviewed in this article were conducted in countries or regions with temperate climates. Although we were not able to find a global or multicountry study that addressed the climate and kidney disease at a large scale, earlier studies have consistently reported kidney disease has seasonality [37] and climatic factors like extreme temperatures [33], and these findings strongly suggest the impacts of greenness on kidney disease can be highly associated with study regions which have different weather and environments. Therefore, more studies in various regions should be performed to address these knowledge gaps.
Lastly, most previous studies that investigated the association between greenness and kidney disease did not address advanced statistical models that can consider complicated spatiotemporal correlations among study subjects. Previous studies investigating kidney diseases in the entire United States showed that there were complex spatial patterns in the occurrence and prevalence of kidney diseases [3,15]. Further, in many countries, the prevalence of kidney disease has been increasing or showing evident temporal patterns [7,16]. However, we were unable to find previous studies on greenness and kidney disease performing spatiotemporal models (such as the Integrated Nested Laplace Approximation, called INLA). Thus, it is difficult to exclude the possibility of estimation bias due to the spatial and temporal autocorrelation in previous results measuring the association between green space and kidney disease, and the usage of advanced statistical models that can address this issue should be considered weightily in future studies.
Conclusion
Recently, the word “Green nephrology” has been raised very actively [45]. Of course, this concept mainly addresses more environmental conditions (energy consumption, water, high volumes of waste, etc.) for dialysis, but in a wide sense, the benefit of green space on kidney health can be closely related to the environmental sustainability of kidney care, which is a major aim of “Green nephrology”. Thus, in order to contribute to more sustainable strategies to address kidney disease, the ultimate goal of studies on greenness and kidney should be to identify the relationship between greenness and kidney disease at both experimental and epidemiological levels and provide scientific evidence for medical and public health implications to alleviate the medical and economic burden due to kidney diseases.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









