



Introduction
Metabolic acidosis is one of the most common complications in patients with chronic kidney disease (CKD) [1]. This condition should not be overlooked by nephrologists in clinical settings because it has been associated with a wide range of poor outcomes including bone demineralization [2], insulin resistance [3], muscle protein proteolysis [4], functional limitations in older individuals [5], and cognitive impairment [6]. Importantly, metabolic acidosis is also associated with cardiovascular outcomes and mortality in CKD patients [7–9]. Basic studies showed that acid retention induced by nephron loss or dietary acid load causes kidney tissue injury through endothelin-1 activation, the renin-angiotensin-aldosterone system, and the alternative complement pathway [10–13]. In contrast, in several clinical cohort studies, low serum bicarbonate levels were shown to be associated with a faster progression of CKD [14–18]. Indeed, randomized controlled trials and corresponding meta-analyses revealed that alkali therapy conferred beneficial effects against the progression of CKD to kidney failure with replacement therapy (KFRT) [19–24].
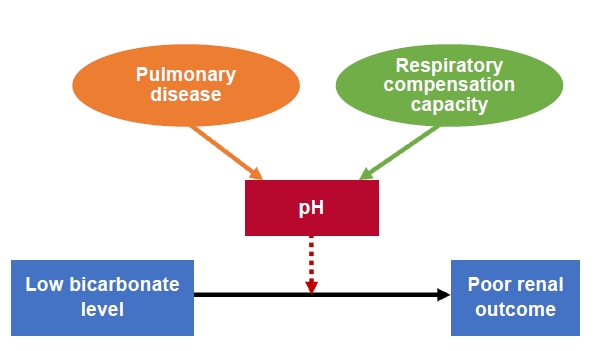
According to current guidelines, alkali therapy initiation is recommended when serum bicarbonate levels are <22 mEq/L [25,26]. However, this recommendation is based exclusively on serum bicarbonate levels (Fig. 1). Additionally, clinical trials of veverimer, a recent novel approach for treating metabolic acidosis, have highlighted the possibility that anion gap acidosis is an important cause of CKD progression. In this review, our objective was to reconsider the effects of metabolic acidosis on the progression of CKD from two different perspectives: blood pH and the anion gap.
Blood pH modulates the association between low bicarbonate level and progression of chronic kidney disease to kidney failure with replacement therapy
Normal H+ concentration in extracellular fluid is almost one-millionth of the concentrations of N+, K+, Cl−, and HCO3−. However, compared with larger cations, such as Na+ or K+, small H+ ions have stronger affinities for small and negatively charged parts of molecules. Therefore, smaller fluctuations in H+ concentrations are required for normal cellular functions [27].
A textbook on acid-base physiology outlines that an initial diagnosis of acid-base disorders should begin with measuring the blood pH [28]. However, blood pH is not frequently measured in certain clinical settings, such as in the United States. Rather, the serum total CO2 (TCO2) is measured to screen for acid-base disturbances, because (TCO2) is affected by both metabolic and respiratory disorders. The screening test ranges from US$26–$33 per test. In contrast, in Japan, a venous blood gas test, that includes measuring Na+, K+, Cl−, pH, pO2, pCO2, and HCO3−, is routinely performed to diagnose acid-base disorders in the clinical outpatient setting [29]. This venous blood gas test costs US$126 based on current exchange rates (US$1 is almost 110 Japanese yen). Importantly, this cost was established by the Japanese government and all Japanese patients are required to have medical insurance; therefore, Japanese clinicians may not be aware of the direct cost as this is covered by patient insurance.
In the United States, serum (TCO2) is used as a surrogate marker of (HCO3−). In Japan, pH and pCO2 in venous blood are measured in clinical laboratories and blood (HCO3−) is calculated using the Henderson-Hasselbalch equation [30]. In the United States, blood gas measurements are rarely performed in the main clinical laboratory and typically assessed in a blood gas laboratory [30], which may not be located in a convenient location for patient referrals from clinics. Further, to minimize errors, the measurements should be taken soon after the blood gas samples are obtained. These barriers to measuring blood gases may account for why blood pH is not frequently measured in the outpatient settings.
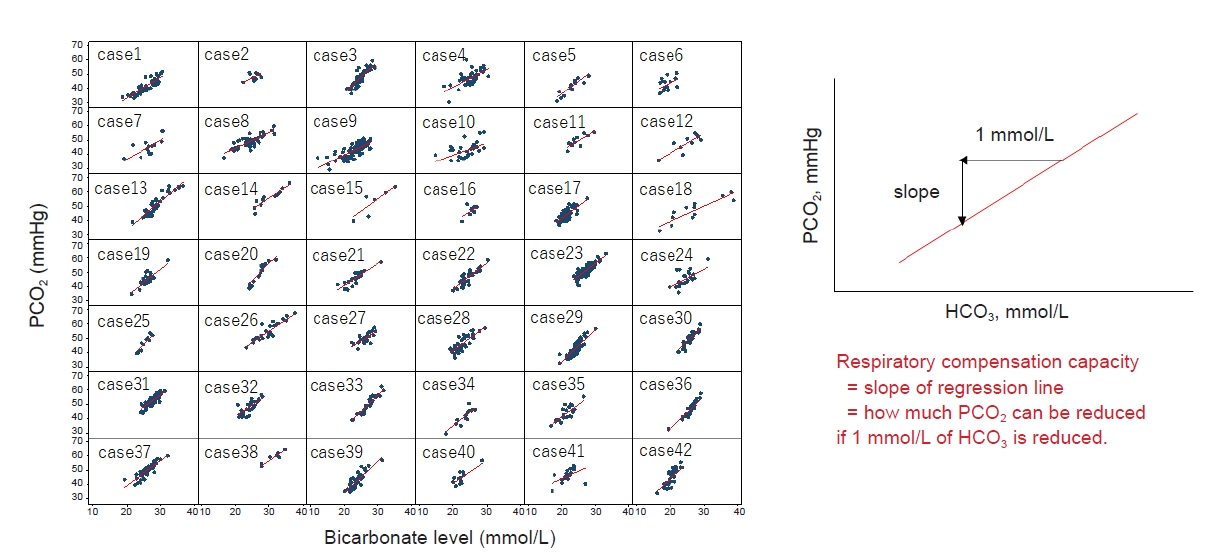
As described above, acid-base disorder diagnoses and prescriptions for alkali therapy were based exclusively on blood (HCO3−) test values. However, the degree to which alterations in blood pH affect CKD progression remains unclear. Recently, Kajimoto et al. [31] addressed this important issue by conducting a retrospective cohort study of Japanese CKD patients. In this approach, they used pH data that were measured along with other parameters in blood gas analyses and analyzed hazard ratios for incident KFRT using Cox proportional hazard models with/without acidemia (pH ⋚7.32). Kajimoto et al. [31] evaluated pulmonary diseases, such as chronic obstructive pulmonary disease or interstitial pneumonia in CKD patients and estimated respiratory compensation capacity using venous blood gas data (Fig. 2). They calculated respiratory compensation capacity using large amounts of blood gas data. We plotted the pressure of carbon dioxide against bicarbonate levels and calculated the slope of the regression line using a mixed-effect model. In this context, the slope of the regression line represents the respiratory compensation capacity and represents how much the carbon dioxide pressure can be reduced for each 1-mmol/L decrease in bicarbonate (Fig. 3).
The cohort included 1,058 CKD patients, among which a total of 374 developed KFRT during the median follow-up of 3.0 years. This study determined that 38% of CKD patients with hypobicarbonatemia ((HCO3−) ≤ 21.5) had normal pH (7.32 ≤ pH ≤ 7.42), whereas 59% with the same (HCO3−) values had acidemia (pH < 7.32). These data indicated that approximately 40% of CKD patients with hypobicarbonatemia ((HCO3−) ≤ 21.5) did not have acidemia, which resulted from an adequate respiratory compensation capacity. This implies that a substantial proportion of patients within the indicated target range for alkali therapy do not exhibit acidemia. The same observation was made in healthy individuals described in the Health ABC study. Approximately 60% of individuals with low bicarbonate levels were determined not to have acidemia [32]. Among CKD patients with acidemia (pH < 7.32), the lowest bicarbonate quartile exhibited a 2.29-fold higher risk of KFRT compared with the highest bicarbonate quartile. In contrast, among patients without acidemia (pH ≥ 7.32), the risk of KFRT in the lowest bicarbonate quartile was not significantly different from that in the highest bicarbonate quartile. In summary, a substantial proportion of CKD patients with hypobicarbonatemia may not be at risk for KFRT, but these patients should be considered as targets for alkali therapy.
With respect to the possibility of increased blood pressure and sodium retention induced by alkali therapy, previous physiologic studies have suggested that NaHCO3 is easier to excrete than NaCl because HCO3− is excreted predominantly as NaHCO3, and not as KHCO3 [33]. Therefore, when dietary sodium intake was restricted to approximately 200–700 mg/day, alkali therapy (200 mEq/day, 16.8 g/day NaHCO3) did not induce increases in blood pressure or body weight in a small number of CKD patients [33]. However, a comparable intake of NaHCO3 (100 mEq/day, 8.4 g/day) and NaCl (100 mEq/day, 5.85 g/day) still induced increases in blood pressure and weight gain [34]. In the general clinical setting, CKD patients do not typically adhere to recommendations to follow very strict restrictions for dietary sodium intake. A recent analysis of CKD patients found that the median salt intake was 8 g/day [35]. Indeed, recent alkali therapy trials excluded patients with uncontrolled hypertension and/or obvious congestive heart failure [36] and patients with decompensated heart failure [22]. Accordingly, CKD patients that meet criteria for alkali therapy should be selected carefully. The report by Kajimoto et al. [31] may provide important guidance for selecting the most appropriate CKD patients for alkali therapy. According to the study, CKD patients with low bicarbonate levels without acidemia may not require sodium bicarbonate. However, subclinical metabolic acidosis with normal serum bicarbonate has recently emerged and is suggested to have clinical significance [37]. In addition, a previous study revealed that alkali therapy caused greater renal function preservation in patients with normal venous total CO2 [20]. Therefore, additional clinical evidence is needed to address the question of which patients will benefit the most from alkali therapy.
Anion gap levels impact the progression of chronic kidney disease to kidney failure with replacement therapy
Two categories of metabolic acidosis have been defined based on anion gap levels; normal anion gap (hyperchloremic) acidosis and high anion gap acidosis. Normal anion gap acidosis is usually identified during the early course of CKD, whereas high anion gap acidosis occurs in later stages of CKD owing to the accumulation of nonchloride anions, including phosphate, sulfate, and a wide range of organic acids [38]. As previously described, low bicarbonate levels have been associated with rapid progression of CKD [14–18]. However, the current clinical understanding of how high anion gap acidosis affects renal outcomes, notably in the later stages of CKD is limited. Some initial studies have reported that uremic acids such as indoxyl sulfate, p-cresyl sulfate, and trimethylamine N-oxide cause renal fibrosis that is induced by kidney injury [39-42].
A recent series of clinical trials of veverimer, a nonabsorbable binding polymer for hydrochloric acid, showed intriguing results that are relevant for therapeutic strategies for metabolic acidosis in CKD [43–45]. Veverimer (TRC101) was developed as a treatment for metabolic acidosis in CKD patients. Veverimer is an orally administered, sodium- and counterion-free hydrochloric acid binder and hydrochloric acid binding is a novel therapeutic concept for treating metabolic acidosis that does not add problematic counterions, such as sodium or potassium. Veverimer selectively captures and removes hydrochloric acid from the gastrointestinal tract and increases serum bicarbonate [44]. In a multicenter randomized controlled trial, treatment with veverimer improved renal outcomes, identified as occurrence of renal replacement therapy, or a decline in estimated glomerular filtration rate (eGFR) of at least 50%, over 52 weeks [43]. Initial research in the veverimer trials hypothesized that chloride ions would increase with veverimer treatment. However, chloride ion levels did not increase in response to veverimer. Interestingly, administration of veverimer reduced the anion gap in CKD patients at 5, 12, and 52 weeks after trial initiation [43,44,46] (Table 1). These data may suggest that veverimer improves kidney function through anion gap reduction.
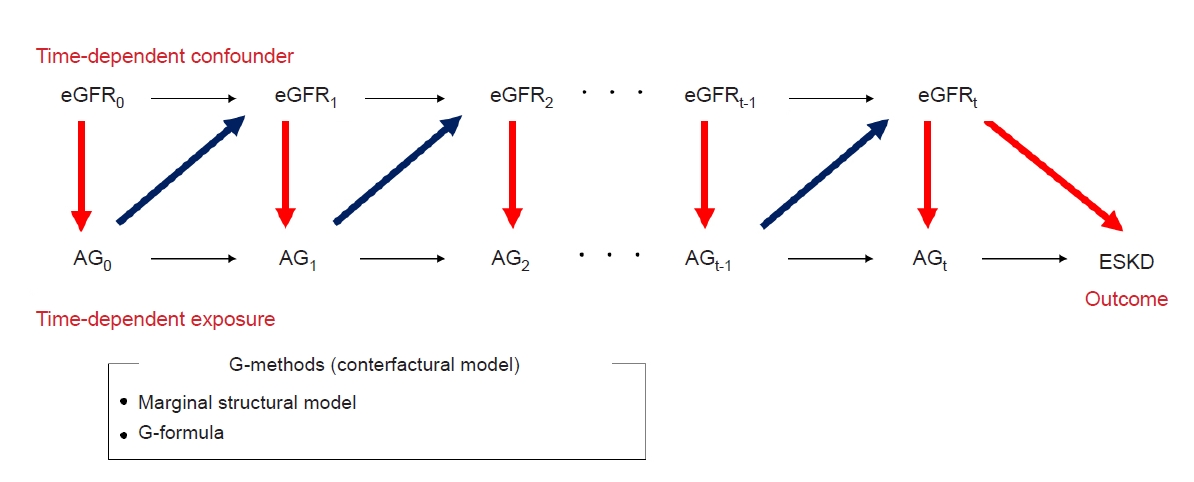
Asahina et al. [47] examined the association between anion gap and renal outcomes using cohort data from 1,168 Japanese CKD patients. It is well established that high anion gap acidosis develops during the later stages of CKD and the anion gap changes with progression of CKD. The anion gap has been repeatedly measured in conjunction with eGFR in Japanese outpatients and kidney function (eGFR) directly affects the anion gap. Moreover, an elevated anion gap may subsequently affect kidney function (eGFR). In this manner, exposure-confounder feedback is generated between the anion gap and eGFR (Fig. 4). Therefore, eGFR is believed to be a time-dependent confounder of the anion gap and renal outcomes. When the association between the anion gap and renal outcomes was analyzed in the presence of a time-dependent confounder, application of the conventional time-dependent Cox proportional hazard model alone was noted as an insufficient method for analysis as it can provide biased estimates [48,49]. Therefore, G-methods should be used for analysis in these situations.
G-methods include marginal structural models (MSMs) and the G-formula. MSM is explained herein for simplicity (Fig. 5); MSM is a counterfactual outcome model that is applied to account for time-dependent confounding. When applying MSMs, analysts establish imaginary pseudo-populations with or without exposure. The pseudo-populations that are established are balanced by inverse probability weighting in terms of baseline covariates and other time-dependent confounders. Asahina et al. [47] obtained time-varying inverse probability weights based on the inverse probability of treatment weights and the inverse probability of censoring weights. By analyzing differences between these pseudo-populations, they were able to determine an assumption for the exposure effect on outcomes.
As previously indicated [50], significantly elevated high anion gap acidosis occurred after stage 4 CKD [47]. In the MSM analysis, metabolic acidosis with a high anion gap was associated with a 3.04-fold rate of KFRT and a 5.56-fold rate of all-cause death, compared with the normal anion gap. However, in the conventional multivariate Cox proportional hazard models, high anion gap acidosis was not associated with a significantly higher rate of KFRT or all-cause death compared with normal anion gap acidosis, suggesting that analyses using Cox proportional hazard models may underestimate the association between the anion gap and renal outcome/mortality.
In a previous study of 1,145 patients with moderate CKD [51], patients in the highest traditional anion gap tertile (11.8–maximum mEq/L) had a higher risk of end-stage renal disease compared with adults in the middle tertile (8.1–11.8 mEq/L) using a frailty model (relative hazard, 1.76; 95% confidence interval [CI], 1.16–2.32). The highest tertile of the full anion gap (19.54–maximum mEq/L) was also associated with a higher risk of all-cause mortality compared with adults in the middle tertile (15.93–19.54 mEq/L) based on a frailty model (relative hazard, 1.20; 95% CI, 1.01–1.39). A possible explanation for the smaller effect size in the analyses by Banerjee et al. [51], compared with those of Asahina et al. [47], may be the difference in renal function of participants (eGFR: 30–60 vs. 10–60 mL/min/1.73 m2, respectively), rather than the difference in statistical methods. The re-analyses that were stratified by eGFR in the study by Asahina et al. [47] revealed that high anion gap patients with an eGFR of ≥30 mL/min/1.73 m2 did not have a significantly higher risk of KFRT compared with normal anion gap patients within the same renal function range.
Anion gap constituents in chronic kidney disease
In the study by Asahina et al. [47], the association between a high anion gap and an increased occurrence of KFRT remained significant when the analysis was adjusted for albumin and phosphate, both of which are primary constituents of the anion gap in CKD patients, suggesting that substances other than albumin and phosphate may be involved in the progression of CKD in response to a high anion gap. In recent metabolomic analyses of human samples identified 492 uremic solutes from patients that continued on hemodialysis compared with age-matched control patients [52]. This included 214 with unknown chemical structure and 278 with known chemical structure, including well-known uremic solutes, 3-indoxyl sulfate, p-cresol sulfate, and trimethylamine N-oxide, all of which were reported to induce renal injury [39–42]. However, 3-indoxyl sulfate, p-cresol sulfate, and trimethylamine N-oxide were only observed at low levels among the 492 uremic solutes, suggesting that other uremic solutes that comprise the anion gap in CKD patients may accelerate the progression of CKD.
Uremic solutes are effectively excreted through both glomerular filtration and tubular secretion [53,54], suggesting that tubular malfunction may lead to accumulation of uremic solutes, and accumulation of solutes may induce kidney injury. Indeed, in the Chronic Renal Insufficiency Cohort study of 3,416 CKD patients, those with reduced tubular secretion of organic acids including kynurenic acid, pyridoxic acid, indoxyl sulfate, xanthosine, isovalerylglycine, and cinnamoylglycine, were found to have a significantly higher risk of progression to CKD [55].
Recently, the human intestinal flora was reported to play a pivotal role in the production of uremic solutes [56]. Renal insufficiency itself strongly affects the colonic microenvironment and alters the composition of intestinal flora to the extent that the environment easily produces toxic uremic retention solutes [57,58]. Several small interventional studies targeting the intestinal flora in patients with renal insufficiency have been performed in response to these data on the association between renal function loss and changes in intestinal flora (known as dysbiosis). Such interventions, including probiotics, prebiotics, and synbiotics, were reported to decrease indoxyl sulfate or p-cresol sulfate in predialysis and dialysis patients [59–64]. However, it is largely unknown if such interventions can in fact reduce anion gap levels in patients. Therefore, further studies to elucidate the mechanism and clinical implications will be needed.
Conclusions
Assessment of venous pH may lead to a reduction in alkali therapy targets for CKD patients with metabolic acidosis. Therefore, it may be possible to reduce the number of cases with adverse effects from sodium bicarbonate supplementation.
Compared with sodium bicarbonate, anion gap-reducing reagents such as veverimer are a novel therapeutic approach for metabolic acidosis and may improve renal outcomes in CKD patients.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









