



Introduction
Remarkable technical advances have been made with regard to dialysis membranes and hemodialysis (HD) machines in recent decades. In spite of such improvements, mortality rates remain high, and the overall 5-year survival rate in patients of kidney failure with replacement therapy (KFRT) is 30% in the United States [1]. Unfortunately, dialysis treatment alone cannot improve clinical outcomes, and a comprehensive approach is required. Such an approach should include blood pressure control, appropriate body fluid control, elimination of middle-sized molecules, removal of inflammatory substances, osteoporosis and anemia management, and the provision of sufficient nourishment. Hemodiafiltration (HDF) can facilitate the achievement of these diverse goals [2ŌĆō5]. In fact, HDF has many advantages over conventional HD, which include its higher clearance of low and middle molecules and inflammatory cytokines, improvement of anemia, and maintenance of hemodynamic stability [6,7]. Notably, recent clinical trials have shown that HDF increased patient survival rates compared to conventional HD, especially in patients who received high-volume convective therapy [7,8].
There are two representative HDF modes: pre- and postdilution. Each has strengths and limitations. Postdilution HDF is the most effective way to maximize molecule clearance. However, blood concentrations can be elevated using HDF, which can cause thrombosis. On the other hand, predilution HDF can resolve this problem [9] but requires about three times more purified water than postdilution HDF and does not guarantee maximal clearance. Therefore, the use of mixed-HDF emerged to compensate for the shortcomings of the other two HDF modalities [10,11]. In mixed-HDF, the substitution fluid required for dialysis is injected at both the entrance and exit of the dialysis membrane. Using a continuous monitoring and feedback system to assess transmembrane pressure (TMP) in the dialyzer, dialysis is automatically switched to either pre- or postdilution HDF mode and optimizes TMP during HD [12]. Despite these advantages of mixed-HDF, clinical studies testing the efficacy of mixed-HDF versus pre- or postdilution HDF are lacking. Several studies have reported that the efficiencies of small- or large-sized molecule removal between mixed-HDF and pre- or postdilution HDF are comparable. Also, TMP is maintained at a more stable level in mixed-HDF compared with postdilution HDF [13ŌĆō15]. In parts of East Asia such as Japan, most HD units tend to use predilution HDF due to intrinsic problems with postdilution HDF, including high TMP and the tendency to promote clot formation [11,16]. This is also true in Korea, where utilization of predilution HDF is increasing [8]. However, whether mixed-HDF performs well in comparison to predilution HDF remains unknown. Therefore, we conducted a randomized controlled trial to compare predilution HDF with mixed-HDF in Korean patients with KFRT.
Methods
Study design and participants
This study was a prospective, randomized, open-label trial conducted at two hospitals in Korea (Severance Hospital, Seoul; National Health Insurance Service [NHIS] Ilsan Hospital, Goyang). Individuals aged 20 to 75 years who had received HD 3 times weekly for Ōēź3 months were allowed to participate in the study. Exclusion criteria were as follows: (1) life expectancy < 12 months, (2) dialysis treatment received for less than 3 months or initiated due to acute kidney injury, (3) current history of malignancy, (4) pregnancy, (5) contraindication to anticoagulants, (6) systemic blood pressure < 90 mmHg, and (7) previously received HDF before enrollment. The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board at each center (No. 4-2016-0702 for Severance Hospital; No. 2018-11-002 for NHIS Ilsan Hospital). All participants provided informed consent when enrolled in the study.
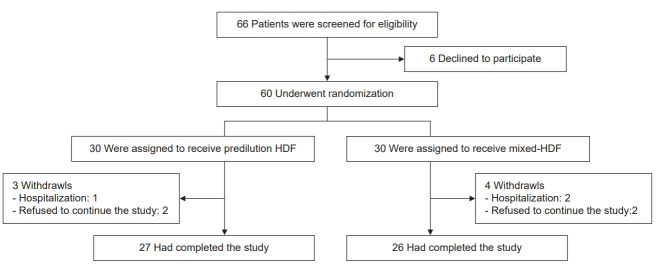
Between January 2017 and December 2019, a total of 66 patients was screened. After a 1-month screening period, 60 patients were randomly assigned at a 1:1 ratio to receive either mixed-HDF or predilution HDF for 6 months. The random assignment was performed using a web-based, random allocation table that considered institution, sex, and causative disease of KFRT (Fig. 1).
Treatment procedures
All participants received thrice-weekly dialysis for at least 3 hours. Both groups were treated with the 5008 or 5008S dialysis system using CorDiax dialyzer (Fresenius Medical Care, Bad Homburg, Germany) and maintained a blood flow rate of 250 mL/min and dialysate flow rate of 700 mL/min. TMP was not expected to exceed 400 mmHg in either predilution HDF or mixed-HDF patients. Prescribed ultrafiltration rate and substitution fluid in both predilution and mixed-HDF groups were calculated using previously reported equations [17].
Study variables
The demographic and medical history of participants was collected at enrollment. We recorded dialysis-related information at baseline and every 3 months thereafter. Information collected included dialyzer characteristics, dialysis time, dialysis machine, blood and dialysate flows, substitution volume, TMP, height, dry body weight, pre- and postdialysis body weight, delivered convective volume, net ultrafiltration volume, and predialysis systolic and diastolic blood pressure. Further, the following laboratory data were measured at 0, 3, and 6 months after initiation of this research: hemoglobin, hematocrit, white blood cell differential count, platelet count, predialysis urea concentration, creatinine, sodium, potassium, concentration of bicarbonate using total carbon dioxide, calcium, phosphate, intact parathyroid hormone, high-sensitivity C-reactive protein (hs-CRP), albumin, and fasting glucose. To determine the reduction ratio (RR) of ╬▓2-microglobulin at pre- and postdialysis, serum ╬▓2-microglobulin level was measured at 0 and 6 months. All laboratory tests were performed locally using standard procedures in certified laboratories. The RR of ╬▓2-microglobulin was calculated using pre- and postdialysis serum ╬▓2-microglobulin levels and the following formula: RR (%) = [1 ŌłÆ (concentration of serum ╬▓2-microglobulin obtained after dialysis/concentration of serum ╬▓2-microglobulin obtained before dialysis)] ├Ś 100. Extracellular fluid and total body water volumes were measured via multiple frequency bioelectrical impedance analysis (BCM; Fresenius Medical Care). Measured extracellular fluid volume is presented as overhydrated (L). Measured relative extracellular fluid volume considering total body water fluid volume is presented as overhydrated-extracellular fluid (%).
Outcomes
The primary outcome assessed was the delivered convection volume difference between mixed-HDF and predilution HDF treatment methods [18]. Since the predilution mode of therapy used twice as much replacement fluid as the postdilution mode, we calculated effective convection volume ratios for mixed-HDF as follows: effective convection volume = substitution volume in predilution mode + 2 ├Ś substitution volume in postdilution mode + ultrafiltration volume. In addition, we compared convection volume adjusted for body surface area between two groups. Secondary outcomes included middle- (RR of ╬▓2-microglobulin) and small-sized molecule clearance (Kt/V urea), changes in predialysis levels of an inflammatory marker (hs-CRP) and phosphate, TMP, blood pressure, and intradialysis tolerance.
Power calculation
The total substitution fluid volume is always greater when using predilution HDF versus mixed-HDF. Because mixed-HDF uses both pre- and postdilution modes during the dialysis session, we hypothesized that the effective convective volume in mixed-HDF would be 120% of that of predilution HDF, and the difference in convective fluid would be approximately 7.5 L, which was used as a noninferiority limit. Thus, it was determined that 25 patients within each group were needed to detect a 10-L delivered convective volume difference between the two groups assessed with a power of 90% and an ╬▒-value of 0.05. Considering a dropout percentage of 20%, the number needed per group was 30 patients.
Statistical analyses
All data were analyzed according to the per-protocol principle. Data are expressed as mean ┬▒ standard deviation or as median (range) for skewed data. Baseline clinical data and laboratory findings, measured at the time of random group assignment, were compared using the t-test and chi-square test. In addition, changes in primary and secondary outcome parameters were analyzed using repeated measures analysis of variance (ANOVA). Continuous variables were assessed using a mixed model approach for repeated measurements, after adjustment for age, sex, serum albumin and hemoglobin levels, systolic blood pressure (SBP), predialysis serum ╬▓2 microglobulin concentration, and dialysis blood flow. A two-sided significance test was used throughout the analysis, and values of p < 0.05 were considered significant. All statistical analyses were performed using the STATA version 16 statistical package (StataCorp, College Station, TX, USA).
Results
Baseline patient characteristics
The baseline characteristics of patients and treatment parameters are summarized in Table 1. The mean age was 59.7 years, and 50.9% of study participants were male. All patients had been on dialysis treatment for 2 years (range, 1ŌĆō4 years). Overall, there were no differences in baseline characteristics observed between the two groups. However, the serum ╬▓2-microglobulin level of the mixed-HDF group was significantly higher than that of the predilution HDF group. Among dialysis parameters, dialysis time, TMP, dialysis flow rate, and net ultrafiltration did not differ between the two groups. However, the mixed-HDF group had slightly lower blood flow rate than the predilution HDF group.
Primary outcome
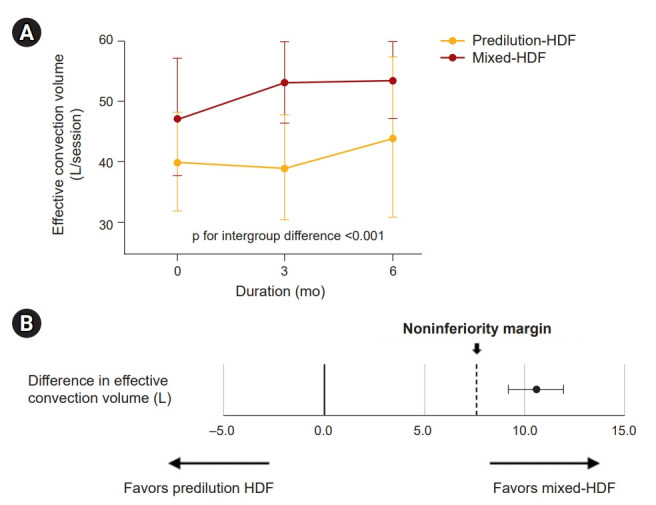
Table 2 and Supplementary Fig. 1A show convection volumes of the two HDF groups during the 6-month period considered. In the predilution HDF group, the mean convective volume determined by averaging values from three time points was 41.0 ┬▒ 10.3 L/session, and the convective volume was constantly delivered during follow-up. In the mixed-HDF group, the switch to predilution mode was successfully accomplished depending on TMP level during the dialysis session. In this group, the total effective convection volume delivered was 51.5 ┬▒ 9.0 L/session in the mixed-HDF group, which was approximately 20% higher than that of the predilution HDF group. The difference in effective convection volume between the two groups was 10.5 ┬▒ 1.3 L/session, which met our preset noninferiority criteria (Fig. 2B, Supplementary Fig. 1B). This finding suggests that mixed-HDF is comparable to predilution HDF with respect to convection volume. Repeated ANOVA analysis and linear mixed model assessment also showed that effective convection volume was greater in the mixed-HDF group than in the predilution HDF group throughout the study period. These results were similar when body surface area-adjusted volumes were compared (Table 2 and Fig. 2).
Secondary outcomes
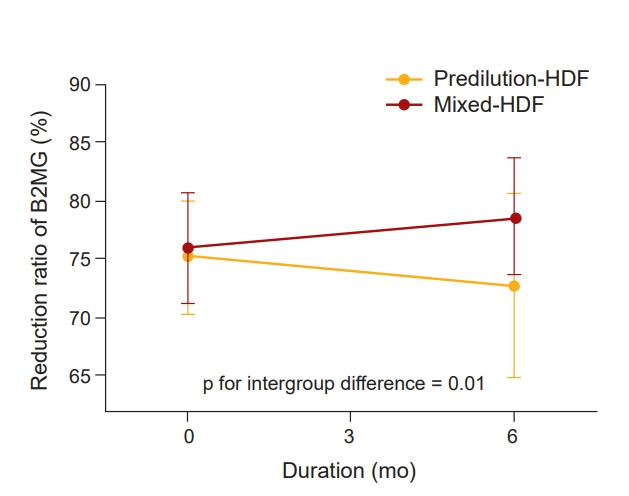
In secondary outcome analyses, we first compared middle- and small-molecule clearance rates of mixed-HDF and predilution HDF groups. The predialysis serum ╬▓2-microglobulin level was significantly higher in the mixed-HDF group than the predilution HDF group during the study period. However, serum ╬▓2-microglobulin level of the mixed-HDF group significantly decreased from the baseline value (25.4 ┬▒ 5.6 mg/L to 22.2 ┬▒ 4.4 mg/L), while they remained relatively constant in the predilution HDF group at the same time period (p for intergroup difference = 0.02) (Table 3, Supplementary Fig. 2A). The ╬▓2-microglobulin RRs at baseline did not differ between the two groups (75.2% ┬▒ 4.9% in the predilution HDF group vs. 76.0% ┬▒ 4.8% in the mixed-HDF group). The RR significantly decreased in the predilution HDF group at 6 months, whereas it increased in the mixed-HDF group (p for intergroup difference = 0.01) (Table 3, Fig. 3). Kt/V urea values, used as a traditional index for small-molecule clearance, were similar between the two groups throughout the study period (Table 3, Supplementary Fig. 2B). We also monitored TMP level during dialysis sessions because the mixed-HDF technique involves switching of HDF mode based on TMP level. The mixed-HDF group had consistently higher TMP level compared to the predilution HDF group during the 6-month study period (p for intergroup difference = 0.001) (Table 3, Supplementary Fig. 2C).
During the study period, there were no significant between-group differences in terms of serum hs-CRP, albumin, phosphate, sodium, potassium, and bicarbonate concentrations (Table 3). Out of 53 patients, 47 had available bioimpedance analysis data. As shown in Table 3, the proportions of overhydration status did not differ between the groups.
At baseline, SBP for the predilution HDF and mixed-HDF groups were 147 ┬▒ 25.7 and 148.1 ┬▒ 22.6 mmHg, respectively. SBP increased at 3 months relative to baseline but then decreased at 6 months relative to the increase observed at 3 months in both groups. The difference observed between the two groups did not reach statistical significance. DBP of both groups remained similar throughout the 6-month study period (Table 3). Most patients tolerated HDF therapy well, and the symptomatic adverse event rate was remarkably low. The most common adverse effect observed was an asymptomatic decrease in SBP by >10 mmHg during a dialysis session, which occurred in 44% of all patients. However, symptomatic intradialytic hypotension was rarely observed in either group (3.7% versus 1.3% in predilution and mixed-HDF, respectively). There were no differences in any other event rates observed between the two groups (Table 4).
Discussion
In this randomized controlled study, we demonstrated that mixed-HDF therapy produces outcomes similar to predilution HDF. Convective volume was delivered well in the mixed-HDF group, and the difference in effective convection volume met noninferiority criteria. We also showed that mixed-HDF more efficiently decreased ╬▓2-microglobulin circulating level compared with predilution HDF. There were no differences in removal rates of small molecules, nor were other clinical or biochemical parameter differences observed during the study period. All adverse events were minor and occurred similarly in the two groups. These findings suggest that mixed-HDF is comparable to predilution HDF with regard to convection volume delivery, and that it removes middle molecules more efficiently.
HDF has been established as effective dialysis therapy, and its use has many advantages over conventional HD. These include higher clearance of middle molecular weight uremic toxins, better maintenance of hemodynamic stability, greater removal of inflammatory cytokines, and better responsiveness to erythropoietin [19,20]. Several randomized controlled trials have demonstrated that HDF reduces all-cause mortality, and even cardiovascular mortality, compared with conventional HD when an optimal convective substitution fluid was used [21ŌĆō25]. Such proven benefits have resulted in the increased utilization of HDF in European countries [26]. There have been remarkable advances in HDF techniques, and several HDF methods have been implemented in clinical practice, including predilution, postdilution, and mixed modes. Most trials to date have tested the effects of postdilution HDF, and studies on other HDF modes are lacking. Interestingly, in East Asian countries, predilution HDF with a low access blood flow rate has been widely used [8]. A recently published observational study in Japan, where predilution HDF is preferred in most centers, suggested that this HDF mode was significantly associated with improved overall and cardiovascular survival compared with conventional HD [27].
Both pre- and postdilution HDF modes have pros and cons. Although the postdilution HDF mode, which is being recommended to most patients in Western countries, is associated with a highly efficient clearance of uremic toxins with a relatively small substitution volume, the limitation of the method is that blood flow should be maintained at a certain speed to reduce risk of blood clot formation. Patients in East Asian countries, who have relatively low blood flow of arteriovenous access, prefer predilution HDF mode to postdilution HDF, due to lower risk of clotting events in the former mode [6]. Recently, a new mode called mixed-HDF was developed to address the drawbacks of pre- and postdilution HDF. Mixed-HDF monitors optimal TMP and automatically switches to pre- or postdilution mode when the TMP level reaches a particular threshold, before a clotting issue occurs [15,28]. This process can compensate for the weaknesses of each HDF mode. Although few studies have compared the efficacy of mixed-HDF versus other HDF modes, Pedrini and De Cristofaro [2] reported that mixed-HDF had a better ╬▓2-microglobulin removal rate than postdilution HDF. In addition, de Sequera et al. [29] showed that mixed-HDF was comparable to postdilution HDF with regard to small and medium-sized and protein-bound molecule clearance.
Delivered convective volume is considered a crucial factor that influences HDF therapy. Mixed-HDF is a new concept of high-efficiency HDF in which predilution and postdilution modes are mixed, and it is difficult to compare quantitatively absolute substitution fluid with those of the predilution mode. Given that a greater volume of substitution fluid is required in predilution mode versus postdilution HDF mode, we developed the concept of using effective convection volume for quantitative comparison between the two groups. Since the predilution mode of HDF uses twice as much replacement fluid as does postdilution mode, we hypothesized that the effective convection volume via mixed-HDF mode consisted of a sum of the substitution volume in postdilution mode times two, substitution volume in predilution mode, and ultrafiltration volume. Although the absolute convection volume was higher in predilution HDF, we showed that the effective convection volume delivered by mixed-HDF was greater than that of predilution HDF. The effective convection volume from mixed-HDF was approximately 20% higher than that of predilution HDF. The optimal convection volume delivered by mixed-HDF remains unknown because no studies have yet examined mixed-HDF outcomes such as mortality or cardiovascular events based on convection volume. In this regard, the concept of effective convection volume might be an alternative tool for the comparison of convection volumes for predilution and mixed-HDF. Notably, differences in effective convection volume might result in improved ╬▓2-microglobulin clearance by mixed-HDF. This is important because the accumulation of middle molecules, such as ╬▓2-microglobulin, is an independent predictor of mortality [30ŌĆō32], and ╬▓2-microglobulin clearance correlates well with convection volume [33]. In addition, dialysis tolerance of patients was similar for the two HDF modes. All adverse events were minor, and the event rates of both groups were similar. Taken together, these findings suggest that mixed-HDF can be an alternative dialysis tool for patients who frequently experience dialysis-related symptoms such as intradialysis hypotension, muscle cramping, and arrhythmia [25].
This study has limitations. First, the sample size was small, and only two centers participated. Therefore, selection bias could not be excluded. Second, we could not determine optimal convection volume. It should be noted that many previous trials with postdilution HDF consistently showed improved patient survival rate compared with conventional HD in patients with adequately delivered convection volume. To date, there has been no randomized controlled trial that has assessed the delivered convection volume in patients given predilution HDF or mixed-HDF therapy. Future studies with larger sample sizes will be needed to address this. Third, we measured ╬▓2-microglobulin and hs-CRP levels as representative middle molecule and inflammatory markers, although other uremic toxins with deleterious effects exist. Because the predilution mode has an intrinsic limitation in the degree of clearance compared with postdilution HDF, the performance of mixed-HDF should be further tested using other molecules. Fourth, we used a simple equation of RR of ╬▓2-microglobulin, which was not calibrated for body fluid reduction during dialysis. However, as there was no significant difference in ultrafiltration volume between the predilution and mixed-HDF groups, ultrafiltration volume is unlikely to alter the outcomes. Finally, we did not evaluate albumin loss via dialyzer during the study. Albumin loss via HDF can differ depending on the dialyzer, dialysis modalities, and convection volumes. Previous studies have reported a wide range of albumin loss between 0.5 and 4.5 g per session in postdilution HDF [34ŌĆō36]. The amount of albumin loss in mixed-HDF is not well known. Although albumin loss is less severe in predilution HDF than in postdilution HDF, albumin loss via HDF can be especially important for patients with marked hypoalbuminemia. However, in this study, the two groups used the same dialyzer that has a very low albumin-sieving coefficient according to the manufacturer. Moreover, serum albumin levels were comparable between the two groups. Thus, albumin loss was unlikely to affect the study results.
In conclusion, we demonstrated that mixed-HDF performed well with regard to convective volume delivery and provided better middle molecule clearance than predilution HDF. For the implementation of mixed-HDF in clinical practice, further studies should explore whether the use of mixed-HDF is advantageous over other dialysis modes with regard to its cost-effectiveness and long-term outcomes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print






")









