Unmasked chronic renal function deterioration after unilateral adrenalectomy in patients with primary aldosteronism
Article information
Abstract
We report 2 cases of chronic estimated glomerular filtration rate (eGFR) decline after unilateral adrenalectomy due to primary aldosteronism. The patients were diagnosed with unilateral adrenal cortical adenoma releasing aldosterone. Two patients were examined for hypertension and hypokalemia. Unilateral laparoscopic adrenalectomy was performed in both cases, and pathology confirmed adrenal cortical adenoma. After adrenalectomy, hypertension and hypokalemia improved to within normal range. However, the eGFR decreased postoperatively, and abdominal computed tomography scan showed decreased kidney size compared to previous images. Kidney biopsy was performed to delineate the exact cause of renal function deterioration and revealed hypertensive changes with chronic interstitial changes, indicating that glomerular hyperfiltration with aldosterone excess masked renal function damage. Physicians have to consider the probability of postadrenalectomy eGFR decline related to chronic hypertensive change.
Introduction
Primary aldosteronism (PA) is an underdiagnosed cause of hypertension but is being increasingly recognized. It is thought to be responsible for 10% of hypertension in humans [1].
To some degree, renal actions related to aldosterone determine the clinical characteristics. Aldosterone increases the number of open sodium channels in the luminal membrane of the principal cells in the collecting tubule and thus, leads to sodium reabsorption increase [2]. The subsequent loss of cationic sodium makes the lumen electronegative, producing an electrical gradient that favors the secretion of cellular potassium into the lumen through potassium channels in the luminal membrane [3]. The typical signs of PA include hypertension and hypokalemia.
Chronic excess aldosterone leads to renal structural damage. Marked renal histological injury in patients with PA has been reported previously [4]. Recent studies have indicated that many PA patients present with a considerable decline in estimated glomerular filtration rate (eGFR) within 6 months of follow-up because of cessation of glomerular hyperfiltration after adrenalectomy [5].
However, histological change of the kidney has not been investigated to confirm the exact cause of chronic decline of eGFR in the postadrenalectomy state.
We describe 2 patients who underwent kidney biopsy because of steady eGFR decline after adrenalectomy for treatment of PA to distinguish hypertensive structural damage from other causes of kidney damage including surgical or thromboembolic changes.
Case report
Case 1
A 62-year-old woman presented with hypokalemia and hypertension. Her systolic blood pressure (SBP) was 147 mmHg and diastolic blood pressure (DBP) was 94 mmHg. Random serum aldosterone was 698.76 pg/mL, and random plasma rennin activity was 0.8 ng/mL/h. Serum potassium level was 2.5 mEq/L, serum creatinine was 0.8 mg/dL, and eGFR was 76.5 mL/min/1.73 m2. Twenty-four-hour urine catecholamines were normal. Abdominal computed tomography (CT) scan revealed a left adrenal tumor measuring 2 cm in diameter.
The patient underwent left laparoscopic adrenalectomy. Histological examination confirmed adrenal cortical adenoma.
Four months after surgery, she was referred to the nephrology unit for sustained eGFR decline. Her SBP was 109 mmHg and DBP was 67 mmHg, and serum potassium level was 5.49 mEq/L. Serum creatinine was 1.78 mg/dL and eGFR was 29 mL/min/1.73 m2.
She was admitted to the hospital 7 months after surgery. Serum creatinine was 1.8 mg/dL (Fig. 1), and abdominal CT scan showed that the size of the left kidney had decreased from 9.9 to 9.3 cm and the size of the right kidney had decreased from 10.6 to 9.0 cm (Figs. 2A,B).
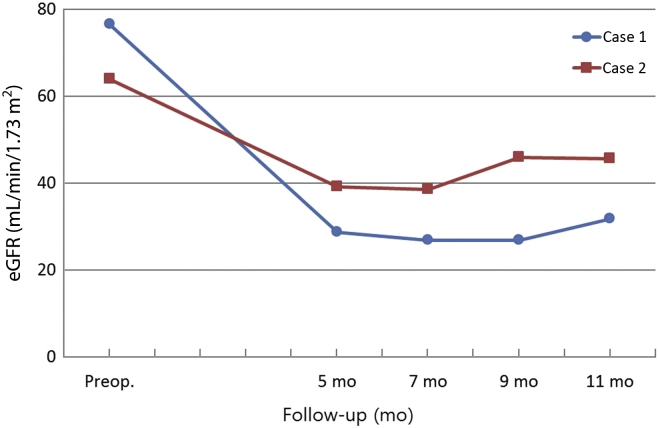
Postoperative changes in eGFR.
eGFR, estimated glomerular filtration rate; Preop, preoperative.
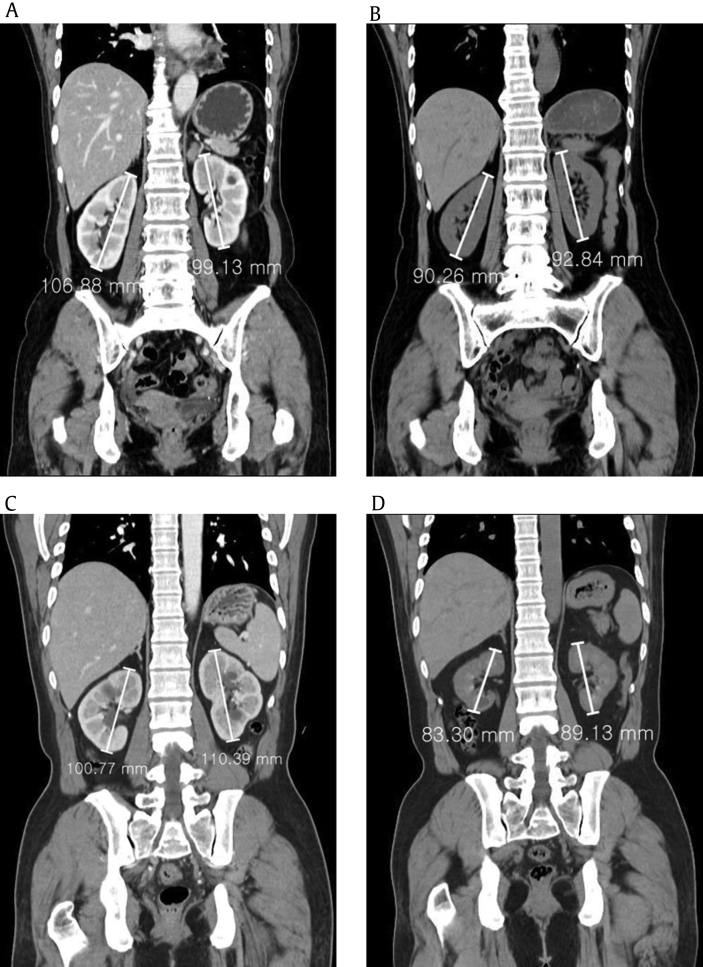
Abdominal computed tomography scan. The size of both kidneys decreased after adrenalectomy in 2 patients (A→B, C→D).
The patient underwent left kidney biopsy to determine the exact cause of renal function deterioration. Pathology confirmed diffuse vascular change with diffuse hyaline arteriosclerosis with hypertensive change, diffuse tubular atrophy, and interstitial fibrosis (Fig. 3A).
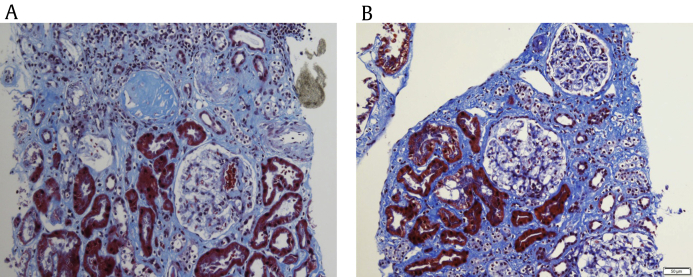
Renal biopsy findings. Light microscopy from the 2 patients (A and B) reveals interstitial fibrosis, tubular atrophy, and hyaline sclerosis of arterioles.
On 1-year follow-up, her serum creatinine remained at 1.8 mg/dL and potassium level was 4.82 mEq/L.
Case 2
A 41-year-old man presented with hypertension and hypokalemia. His SBP was 142 mmHg and DBP was 91 mmHg.
Random serum aldosterone was 1,020 pg/mL, and renal plasma rennin activity was 0.2 ng/mL/h. Serum potassium level was 3.2 mEq/L, serum creatinine was 1.25 mg/dL, and eGFR was 64 mL/min/1.73 m2. Twenty-four-hour urine catecholamines were normal. Abdominal CT scan revealed a left adrenal tumor measuring 1.5 cm in diameter.
The patient underwent left laparoscopic adrenalectomy. Adrenal cortical adenoma was diagnosed on pathology.
He was referred to the nephrology unit for continued creatinine elevation, 6 months after surgery. His SBP was 110 mmHg and DBP was 70 mmHg. Serum potassium level was 4.33 mEq/L and creatinine was 2.16 mg/dL (Fig. 1). Abdominal CT scan showed that the size of the left kidney had decreased from 10 to 8.3 cm and the size of the right kidney had decreased from 11 to 8.9 cm (Figs. 2C,D).
The patient underwent left kidney biopsy to distinguish the cause of eGFR decline. Pathology revealed chronic interstitial change, hypertensive change, and hyaline sclerosis of arterioles (Fig. 3B).
On 8-month follow-up, serum creatinine remained at 1.9 mg/dL and potassium level was 4.74 mEq/L.
Discussion
Patients with PA exhibit glomerular hyperfiltration and glomerular vascular hypertension [6]. Aldosterone induces dose-dependent contraction in both arterioles. The vasoconstricting effect of aldosterone is substantially stronger in efferent arterioles than afferent arterioles [7]. Through its vasoconstricting effect on the postglomerular efferent arteriole, aldosterone increases glomerular capillary pressure. Aldosterone might play an important role in renal vascular resistance. Glomerular hypertension is thought to be responsible for glomerular structural damage [8]. This vasoconstricting effect may account for the pathogenic role of hyperaldosteronism in eGFR decline. Cross-sectional studies on kidney function in PA have revealed a wide variety of renal damage [7]. Animals infused with aldosterone had arteriolar and glomerular thrombotic and proliferative lesions and developed massive proteinuria [9]. Glomerular capillary hypertension is a widely known risk factor for proteinuria and renal insufficiency [10]. Adjusted 24-hour urine albumin excretion was found to be considerably higher in patients with aldosterone-producing adenoma (n = 31) and idiopathic hyperplasia (n = 33) than in 426 primary hypertension patients [10].
However, renal functional deterioration can be masked by glomerular hyperfiltration in patients with PA. Thus, accurate evaluation of kidney function in patients with PA may be a challenge [11]. If a patient with PA suffers from unexpected eGFR decline after adrenalectomy, he may feel very embarrassed with it.
To the best of our knowledge, this case is the first to histologically confirm hypertensive renal change in patients with chronic eGFR decline after adrenalectomy. It could us exclude the possibility related surgical or thromboembolic damages. Excess aldosterone is related to glomerular hyperfiltration. Structural damage involving renal microvascular lesions might develop from chronic hypertensive damage and the direct side effects of aldosterone in kidneys with PA. Decline in eGFR is a special functional response to treatment in PA. Adrenalectomy does not aggravate renal function per se, but it can reveal previously masked renal damage. Correction of excess aldosterone may improve intraglomerular pressure and unmask renal function deterioration.
Prevention of kidney impairment is an important target in the treatment of hypertension. We have to keep in mind the possibility that patients with PA may have structural damage despite normal eGFR and should thus monitor eGFR closely. Early awareness and care of chronic kidney disease are critical in preventing poor outcomes. If postoperative eGFR declines, physicians should consider the possibility that the decline is related to hypertensive change.
Conflicts of interest
All authors have no conflicts of interest to declare.
References
Acknowledgments
This work was supported by Clinical Research grant in 2016 from Pusan National University Hospital.