

Autosomal dominant polycystic kidney disease (AD-PKD) is the most common inherited disorder leading to end-stage renal disease (ESRD). A mass effect caused by ADPKD can cause symptoms such as abdominal fullness, dyspnea, and early satiety through increased intraabdominal pressure. An obturator hernia is rare, but can be serious in patients with ESRD if not diagnosed promptly. We present a case with inguinal pain caused by an obturator hernia in a patient with ADPKD. A 67-year-old female on hemodialysis for ESRD caused by ADPKD was admitted to the emergency department for acute inguinal pain. She had begun hemodialysis approximately 20 years prior. She reported 7 days of inguinal pain unresponsive to analgesics and developed nausea and vomiting 2 days prior to presentation. She had delivered twice. Congestive heart failure had been diagnosed, but there was no apparent ascites or pulmonary edema. Computed tomography showed multiple air-fluid levels in the small bowel and a diffusely dilated proximal and middle small bowel, accompanied by a focal bowel herniation sac without incarceration (Fig. 1A). Laboratory data were unremarkable. We performed emergency surgery. Initial operative findings included an incarcerated small bowel (Fig. 1B), but the incarceration improved with manual reduction. After confirming recovery of small bowel color, herniorrhaphy was performed. Her symptoms completely resolved. Obturator hernias account for less than 0.1% of all hernias. Theoretically, conditions resulting in increased intraabdominal pressure can induce an obturator hernia. Elderly multiparous women and patients with massive ascites or chronic constipation have increased risk. However, ADPKD may also be a predisposing factor for an obturator hernia. As the kidney volume in ADPKD can increase relatively rapidly following early diagnosis, the possibility of an obturator hernia should be considered if patients with ADPKD have acute inguinal pain.
| Kidney Res Clin Pract > Volume 37(2); 2018 > Article |

|
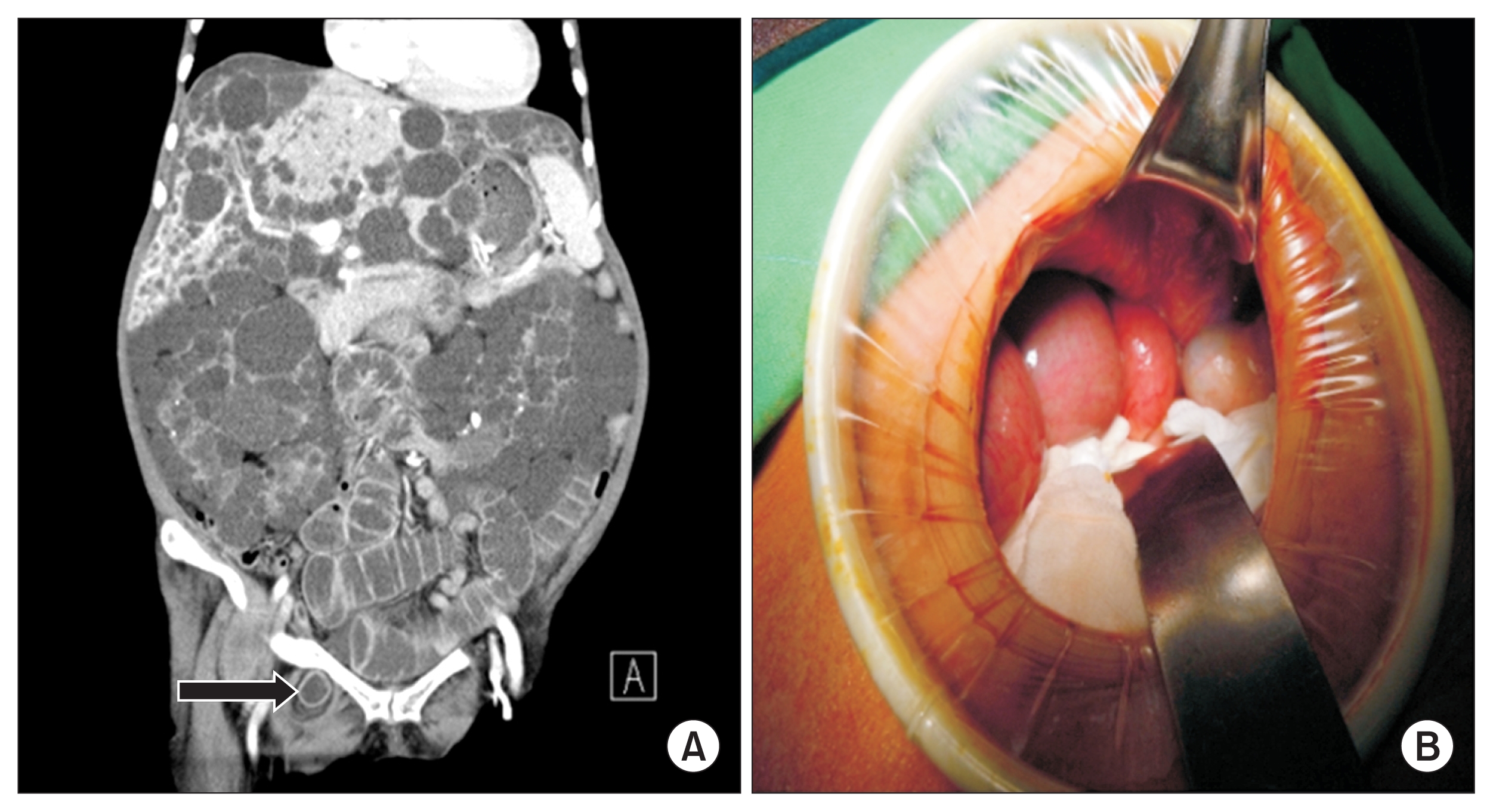
Figure 1
Images of obturator hernia in polycystic kidney disease
(A) Computed tomography demonstrates multiple air-fluid levels in the small bowel and diffusely dilated proximal and middle small bowel, accompanied by a focal bowel herniation sac (arrow) without incarceration. (B) Bluish color change was observed in the small bowel during surgery.
- TOOLS
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print


-
METRICS

- Related articles
-
Cinnamon: an aromatic condiment applicable to chronic kidney disease2023 January;42(1)



")








- Editorial Office
-
#301, (Miseung Bldg.) 23, Apgujenog-ro 30-gil, Gangnam-gu, Seoul 06022, Korea
Tel: +82-2-3486-8736 Fax: +82-2-3486-8737 E-mail: registry@ksn.or.kr
Copyright © 2024 by The Korean Society of Nephrology.

