


Introduction
Red cell distribution width (RDW) expressed as a percentage is a measure of the variation in red blood cell size and is routinely reported in a complete blood count [1]. RDW in association with mean corpuscular volume (MCV) has traditionally been useful for diagnosing certain types of anemia, as RDW is increased in iron deficiency, sickle cell disease, myelodysplasia, and chronic liver disease [2].
Recent evidence has shown that a high RDW is associated with high cardiovascular morbidity and mortality as well as all-cause mortality [3,4]. Thus, RDW is considered an emerging risk prediction tool that is both inexpensive and easy to measure. However, the mechanisms underlying these associations with RDW are not well understood.
There are a growing numbers of studies on RDW and its association with the kidneys, most of which have demonstrated that RDW has predictive power for poor prognosis in patients with existing chronic kidney disease (CKD) [5ŌĆō8]. On the other hand, only a few studies have investigated the association between RDW and the development of renal disease [9,10]. Albuminuria is not only a well-known marker of target organ damage in hypertension and diabetes, but is also an important component for diagnosing CKD [11,12]. Furthermore, albuminuria is a strong risk factor for poor renal outcome in CKD as well as high cardiovascular and all-cause mortality in the general population [13,14]. A few studies comprising relatively small numbers of patients have reported an association between RDW and albuminuria in a high-risk group with hypertension and diabetes [15ŌĆō17], while one large study with national data verified the relationship between RDW and albuminuria [18]. However, because these studies were cross-sectional by design, they are unable to provide evidence of a causal relationship.
The purpose of this study was to analyze the relationship between RDW and development of albuminuria in patients without evidence of CKD and to confirm this association in a large-scale longitudinal study.
Methods
Study design and population
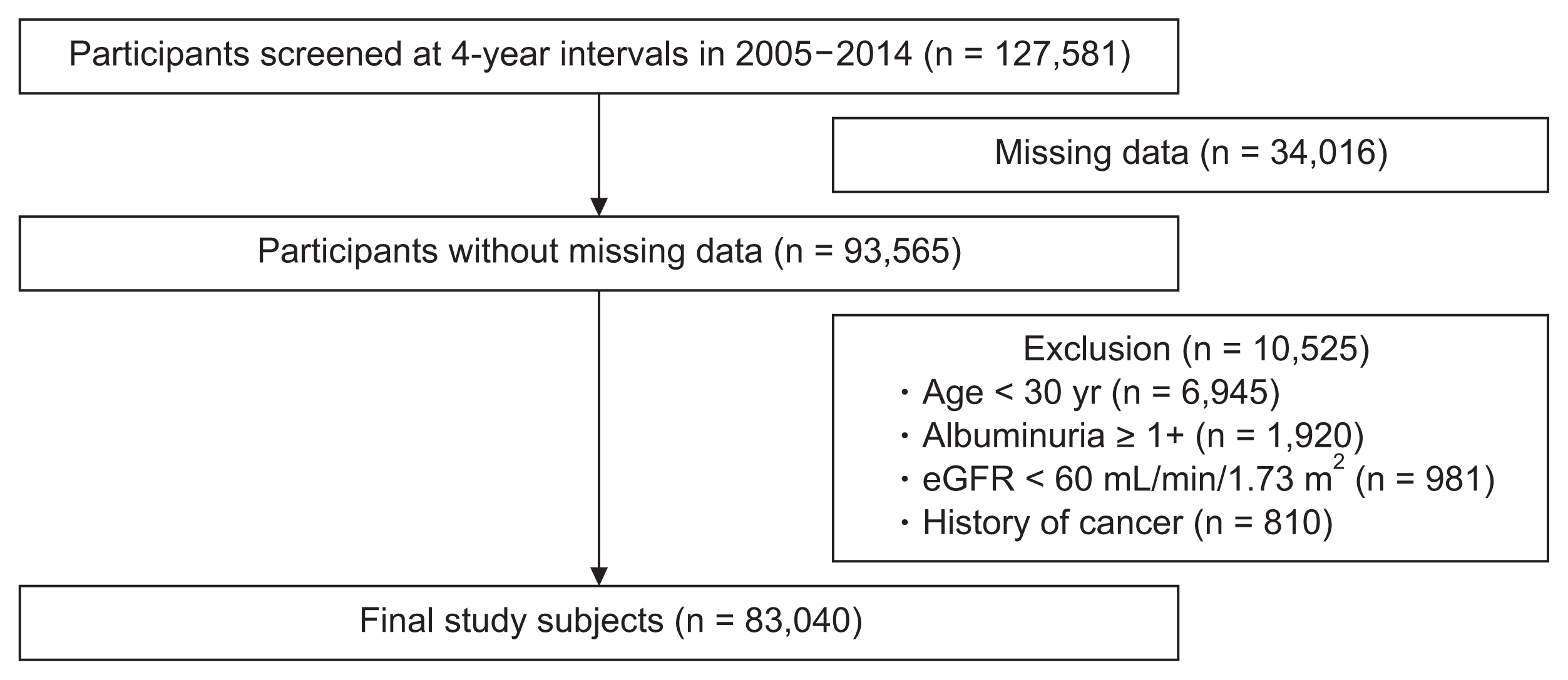
We constructed a retrospective cohort using participants who received regular health maintenance exams at Kangbuk Samsung Hospital, Sungkyunkwan University, Seoul, Korea. A total of 127,581 participants who visited the center twice at a 4-year interval between 2005 and 2014 were considered for inclusion in the study cohort. We excluded 34,016 records due to missing data for the variables of interest. We also excluded subjects aged < 30 years in order to prevent the possibility of orthostatic proteinuria (n = 6,945). We further excluded participants with evidence of CKD (dipstick albuminuria Ōēź 1+, n = 1,920; estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2, n = 981) or a history of cancer (n = 810) at baseline. The final analysis included 83,040 participants. The process for constructing the retrospective cohort is summarized in Fig. 1. This study was approved by the Institutional Review Board at Kangbuk Samsung Hospital (KBSMC 2017-01-033).
Clinical and laboratory measurements
The health check-up consisted of a medical history, physical examination, health-related behavior questionnaire, biochemistry studies, and anthropometric measurements. The examining physicians assessed each patientŌĆÖs medical history and prior use of medications. Height, weight, and blood pressure were measured by trained nurses while the participants were wearing a light hospital gown without shoes. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
Blood specimens were sampled from an antecubital vein after > 12 hours of fasting. Hemoglobin, mean corpuscular volume, and RDW were measured with an automated hematology analysis system Sysmex XE-2100D (Sysmex Corporation, Kobe, Japan) and Advia 2120 (Siemens Medical Solutions Diagnostics, New York, NY, USA). Plasma glucose, total cholesterol, triglycerides (TG), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein cholesterol, and uric acid level were measured using an autoanalyzer (Advia 1650 Autoanalyzer; Bayer Diagnostics, Leverkusen, Germany). Insulin was measured by immunoradiometric assay (Biosource, Nivelles, Belgium). Insulin resistance was assessed with the homeostasis model assessment of insulin resistance (HOMA-IR) calculated as fasting blood insulin (╬╝U/mL) ├Ś FBG (mg/dL)/405. Serum creatinine level was measured with the alkaline picrate (Jaffe) method.
Trained medical technicians performed regular calibration and quality control for creatinine measurements during the study period using a validated calibrator and quality control materials. In addition, our clinical laboratory participated in an annual inspection and survey by the Korean Association of Quality Assurance for Clinical Laboratories and is certified for quality control and performance of various measurements. Because the laboratory method that was used to measure serum creatinine levels from 2002 to 2009 was not traceable to isotope dilution mass spectrometry, GFR was estimated using the 4-variable Modification of Diet in Renal Disease Study equation [19,20]. Urine albumin was determined at each examination with a single urine dipstick semi-quantitative analysis (URiSCAN Urine strip; YD Diagnostics, Yongin, Korea). Dipstick urinalysis was performed on fresh, midstream urine samples collected in the morning. The amount of urine albumin was reported as absent, trace, 1+, 2+, 3+, or 4+, corresponding to albumin levels of undetectable, 10, 30, 100, 300, or 1,000 mg/dL albumin, respectively. Albuminuria was defined as a grade Ōēź 1+.
In this study, diabetes was defined as fasting glucose Ōēź 126 mg/dL, a history of previously diagnosed diabetes, or the use of anti-diabetic medications. Hypertension was defined as systolic blood pressure Ōēź 140 mmHg or diastolic blood pressure Ōēź 90 mmHg, a history of hypertension, or the use of antihypertensive medications. Dyslipidemia was defined as total cholesterol > 240 mg/dL or previous history of dyslipidemia.
Statistical analyses
Continuous variables were expressed as the mean ┬▒ standard deviation for normally distributed variables or the median (interquartile range) if not normally distributed. Continuous variables were compared between two groups using StudentŌĆÖs t-test or the MannŌĆōWhitney U test. Analysis of variance or the KruskalŌĆōWallis test was used for comparisons between the four groups. Categorical variables are expressed as percentages and compared using the Žć2 test. We used multivariate logistic regression analysis to determine the odds ratios (ORs) for developing albuminuria by RDW quartile. The lowest RDW quartile was used as the reference. Covariates for multivariate analysis consisted of age, gender, BMI, hypertension, diabetes, dyslipidemia, hemoglobin, mean corpuscular volume, eGFR, high-sensitivity C-reactive protein (hsCRP), current smoking status, alcohol intake, and vigorous exercise frequency. For statistical calculations, we used Stata version 14.0 (StataCorp LP, College Station, TX, USA). Two-sided P values less than 0.05 were considered statistically significant.
Results
The baseline characteristics of study participants according to RDW quartile are summarized in Table 1. Unexpectedly, subjects who were in the 2nd or 3rd RDW quartile, but not the 4th, had worse metabolic characteristics. For example, BMI was 23.4 ┬▒ 3, 23.7 ┬▒ 3.1, 23.7 ┬▒ 3.1, and 23.3 ┬▒ 3.2 (P < 0.001) for the 1st through 4th quartiles, respectively. Likewise, the percentage of participants with hypertension was 10.8, 12.1, 12.9, and 11.0 (P < 0.001) for the 1st through 4th quartiles, respectively.
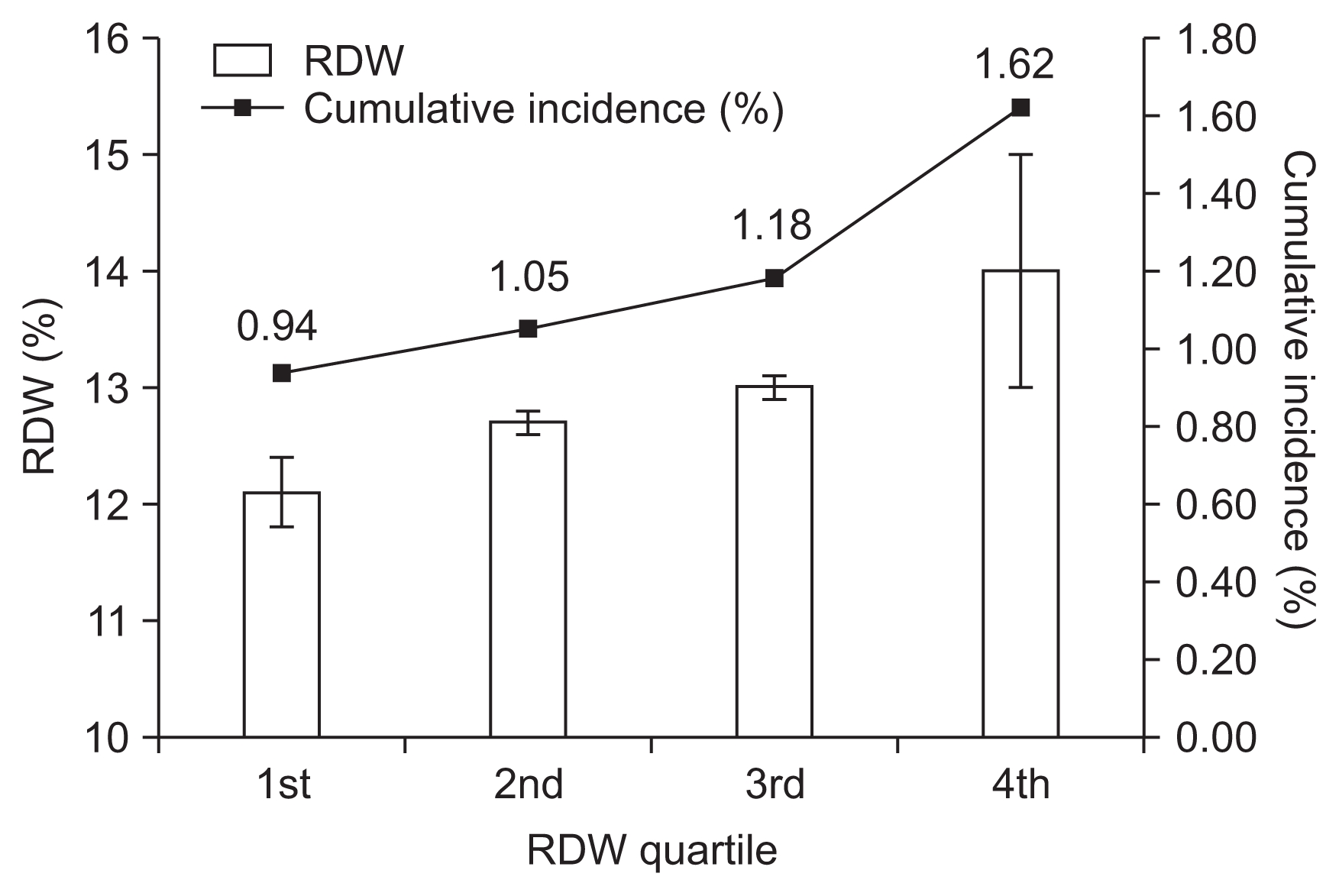
A total of 982 cases of incident albuminuria were observed in the retrospective cohort of 83,040 participants over a period of 4 years. The degree of albuminuria was 1+ in 712 participants, 2+ in 242 participants, 3+ in 17 participants, and 4+ in 11 participants. The numbers (%) of patients with incident albuminuria from the lowest to highest quartiles were 230 (0.94), 224 (1.05), 196 (1.18), and 332 (1.62), respectively (Fig. 2).
The characteristics of participants with incident albuminuria were compared to those without albuminuria and are shown in Table 2. In general, participants with incident albuminuria had an unhealthy profile compared to participants without albuminuria. Specifically, patients with incident albuminuria were older and had higher BMI, systolic blood pressure, diastolic blood pressure, serum glucose, total cholesterol, LDL cholesterol, TG, HOMA-IR, hsCRP, uric acid, and alcohol intake. Participants with incident albuminuria were also more likely to be male and current smokers and to have hypertension or diabetes.
Table 3 shows the association between RDW level and incident albuminuria according to multiple logistic regression analysis. The development of albuminuria was associated with a high RDW. As shown in Table 3, the OR for incident albuminuria in the 4th quartile compared to the 1st quartile was 1.88 (95% confidence interval, 1.58ŌĆō2.24; P < 0.001) in the fully adjusted model 3. To test the robustness of this association, we repeated the analysis with different subgroups (Table 4). In the repeat analysis, the 4th quartile when compared to 1st quartile of RDW was associated with incident albuminuria in participants without diabetes or hypertension (OR, 1.86; P < 0.001), as well as in participants without hypertension or heart disease (OR, 1.82; P < 0.001). This result was similar for participants who were not underweight (OR, 1.92; P < 0.001).
Discussion
In this study, we found that high RDW was associated with incident dipstick albuminuria 4 years later in Koreans without previous CKD. This relationship was independent of markers of inflammation and nutrition as well as other potential risk factors for developing albuminuria.
Studies on RDW in the area of nephrology have largely addressed its potential to predict mortality, and RDW is indeed associated with high mortality in different CKD populations, including predialysis patients, patients on hemodialysis or peritoneal dialysis, and kidney transplant recipients [5ŌĆō8]. However, little is known about the specific relationship between RDW and CKD, although several studies have investigated the association between RDW and renal function or albuminuria. Lippi et al [21] was the first to show an inverse and graded association between RDW and eGFR in a large Italian outpatient cohort. This inverse association was reaffirmed in 723 kidney transplant recipients and was shown to be independent of various comorbidities and markers of inflammation and nutrition [22]. In the present study, eGFR was low in patients with the highest RDW, which was compatible with the results of previous studies. In terms of albuminuria, Afonso et al [18] analyzed 8,499 representative participants in the National Health and Nutrition Examination Survey and found that elevated RDW was independently associated with microalbuminuria. A few other studies have demonstrated the same relationship in smaller, high-risk groups of patients such as those with hypertension or diabetes [15,16,23]. However, the studies described above were cross-sectional in design, and only two other small longitudinal studies have been performed. These longitudinal studies analyzed patients undergoing coronary angiography or percutaneous coronary intervention and showed that increased RDW predicts renal function decline after use of contrast media [9,10]. Thus, to the best of our knowledge, this is the first longitudinal study to show that high RDW predicts future development of albuminuria. Importantly, this relationship was valid in participants without major risk factors such as diabetes or hypertension, as well as participants who were not underweight, which is a possible risk factor for albuminuria [24].
The mechanism involved in RDW and incident albuminuria is not clear, but there are several possible explanations. First, RDW acts as a general marker of the severity of various comorbidities. For example, anisocytosis assessed as a high RDW is prevalent in different illness including cardiovascular disease, cancer, diabetes, lung disease, and liver disease [4], and most of these diseases are important risk factors for kidney damage and albuminuria. Although we corrected for major comorbidities and laboratory results in our analysis, it was not possible to completely cover the entire array and severity of all accompanying diseases. Second, previous studies have suggested that inflammation, oxidative stress, and malnutrition might mediate the association between RDW and poor outcome [25,26]. Certainly, inflammation and oxidative stress are closely related to albuminuria [27,28], and malnutrition is one of the important characteristics of CKD. Thus, the two conditions might be connected through a common pathway, although the specific mechanism should be clarified in the future. A third explanation is that a high RDW itself might be directly harmful to kidneys. Specifically, an increased RDW is associated with decreased RBC deformability, which can result in impairment of microcirculation and hypoxia [29]. In addition, RDW is also related to endothelial dysfunction assessed by flow-mediated dilation [30], and both hypoxia and endothelial dysfunction are associated with different diseases that present with albuminuria [31,32].
This study had several limitations. First, we measured albuminuria only once at each examination. However, transient albuminuria can be observed in conditions such as febrile illness, strenuous exercise, emotional stress, and urinary tract infection [33]. Second, we used the semi-quantitative dipstick test to evaluate albuminuria, which might be influenced by urine concentration. However, the effects of urine concentration would not favor a specific direction of results; thus, errors from variation in urine concentration would have been minimized by the large sample size. Third, we did not have information on the use of medications such as angiotensin-converting-enzyme inhibitors or angiotensin receptor blockers, which could affect the amount of albumin excretion. However, our results did not change after excluding patients with hypertension and heart disease, a population that has a high likelihood of taking these medications. Despite these limitations, the present study is significant in that it is the first to show an effect of high RDW on the development of albuminuria in individuals without CKD.
In conclusion, we identified a graded independent association between higher RDW and new onset dipstick albuminuria in Korean adults without previous CKD. Further research is warranted to determine the exact mechanism by which RDW leads to the development of albuminuria and renal injury.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









