Use of low-dose sulodexide in IgA nephropathy patients on renin–angiotensin system blockades
Article information
Abstract
Background
Despite using renin–angiotensin system (RAS) blockades, some of the patients with immunoglobulin A (IgA) nephropathy often had persistent proteinuria of more than 500 mg/d. They need to be managed further by alternative methods to halt the progression of the disease; these methods could also be applied safely over a long period of time. In this context, sulodexide has been studied for the management of diabetic nephropathy.
Methods
A retrospective review was carried out involving 20 patients with IgA nephropathy who had been taking sulodexide (50 mg daily) as an add-on therapy together with an optimal dose of RAS blockades during 2008–2009. We evaluated the proteinuria reduction rates and renal function changes.
Results
During 11.1±72.7 months of follow-up duration, urinary protein-to-creatinine ratio (UPCR) decreased for 1.57±0.6 to 1.17±0.7 g/g (P=0.032). Twenty-five percent of the patients showed a greater than 50% reduction of UPCR, and 40% had a UPCR of less than 1.0 g/g at their final observations. The analysis of the factors contributing to the effect found that a higher pretreatment UPCR showed a significant correlation with the UPCR decrease (r=0.45, P=0.047). Neither the adverse effects nor the renal function impairments were documented during the management.
Conclusion
Low-dose sulodexide has an additional modest antiproteinuric effect on IgA nephropathy undergoing RAS blockade therapy.
Introduction
Immunoglobulin A (IgA) nephropathy is one of the most common primary glomerulonephritides, progressing to end-stage renal disease (ESRD) in about a third of its patients over a period of 20–25 years after diagnosis [1], [2]. There are many factors related to disease progression and development, such as renal function at diagnosis, proteinuria, hypertension, microscopic hematuria, glomerulosclerosis, interstitial fibrosis, and so forth [3], [4], [5]. Of these factors, proteinuria has been regarded as not only a reflecting, but also a causative factor for renal damage [6].
A dominant therapeutic approach to IgA nephropathy is the inhibition of the renin–angiotensin system (RAS), which can be achieved using RAS blockades such as angiotensin-converting enzyme inhibitors (ACEi) and angiotensin II receptor blockers (ARB) [5], [7]. However, the efficacy of RAS blockades have been found to be insufficient in overt proteinuric IgA nephropathy; therefore, immunosuppressive approaches, including glucocorticoids and/or cytotoxic agents, have been adopted [7], [8]. Although immunosuppressive regimens have shown sufficient efficacies in some patients with IgA nephropathy, their adverse effects could be problematic [9]. Therefore, we need to find a safe and long-term method for reducing renal damage.
Sulodexide is an oral formulation of a highly purified mixture of glycosaminoglycans (GAGs). It is composed of 80% fast-moving heparin sulfate and 20% dermatan sulfate, and is the most extensively investigated GAG mixture for diabetic patients [10], [11]. It bears a strong chemical similarity to heparin, but does not show anticoagulant properties when given orally. Sulodexide has emerged as a potential treatment for diabetic nephropathy. Multiple studies have demonstrated reductions in urinary protein excretion with GAG therapy [12], [13]. However, only a few studies demonstrate the effects of sulodexide on the management of primary glomerular diseases.
We conducted this research to investigate the antiproteinuric effect of sulodexide in patients with IgA nephropathy showing persistent proteinuria, in spite of optimal management with RAS blockades.
Methods
Study participants
Retrospective analyses were performed in all patients with IgA nephropathy who were on RAS blockades and sulodexide between September 2008 and May 2009. We selected those patients who were over 18 years old, had received RAS blockades, had stable blood pressure levels of less than 130/80 mmHg for at least last 6 months, and showed persistent proteinuria [urinary protein-to-creatinine ratio (UPCR) >0.5 g/g]. The patients who received immunosuppressants in the last 1 year or had systemic lupus erythematosus, chronic liver diseases, malignancies, or inflammatory bowel diseases were excluded.
Data collection
We reviewed the records of the patients to collect data on accompanying medications, comorbidities, changes of blood pressure, and dose and duration of sulodexide administration. Laboratory data included serum creatinine, serum albumin, serum total cholesterol, and urinary protein levels, by checking the UPCR on every visit to the outpatient department. Glomerular filtration rates (GFRs) of the participants were calculated by the Modification of Diet in Renal Disease Study equation. Pathologic findings regarding IgA nephropathy of the patients were rated into five grades, according to the WHO classification proposed by Churg and Sobin [14]. Specifically, we added the data regarding the states of the foot process effacements (FPE) on electron microscopy by grading them into three levels: mild (<30%), moderate (30–70%), and severe (>70%) [15].
Outcomes
The change in UPCR between the initiation of sulodexide administration and the last laboratory report from the survey was calculated to determine whether the treatment offered a reasonable reduction of proteinuria. Factors related to the antiproteinuric effect of sulodexide were analyzed as well.
Statistical analysis
The SPSS (SPSS version 15.0; SPSS Inc., Chicago, IL, USA) package was used for statistical analysis. The efficacy of sulodexide in diminishing proteinuria during treatment was analyzed using the Wilcoxon signed-rank test. To analyze the correlations between the factors and the outcome, the Spearman's correlation, the Kruskal–Wallis test, and the Pearson's chi-square test were used. Two-sided P values were reported, and a value of 0.05 was considered as the level of statistical significance. All data were shown as mean±standard deviation for continuous variables or frequency (percent) per observation for nominal variables.
Ethics statement
Approval was obtained from the local ethics committee for an anonymous analysis of routinely collected clinical data, with a waiver of informed consent.
Results
Baseline characteristics of the participants
A total of 20 patients were included in the study. The duration of the previous RAS blockade therapy was 2.9±1.9 years, during which the doses were raised in case of 16 patients (80%), and a combination of ACEi and ARB was given to two patients (10%) for maximizing antiproteinuric effects, except when disabling hypotension was encountered. All the patients had been taking 50 mg of sulodexide daily for 11.1±2.7 months (Table 1).

Baseline characteristics
Pathologic findings indicated that WHO grade III was predominant (65%), and the FPE showed over 50% effacement in most cases (Table 2). There were no significant correlations between the FPE finding and the initial UPCR or WHO grade.

Pathologic features of IgA nephropathy at baseline
Changes in blood pressure, biochemical values, and renal function
Well-maintained blood pressure under 130/80 mmHg was observed throughout the sulodexide treatment period (Table 1). Biochemical values, including serum creatinine, albumin, uric acid, and total cholesterol, were stable without any significant differences between the initial and the final findings (Table 3). Of the patients, 11 (55%) had chronic kidney disease (CKD) stage 2, and six (30%) CKD stage 3. No additional changes in renal function were detected throughout the treatment period (Table 3).

Comparison of laboratory findings before and after sulodexide therapy
Antiproteinuric effect of sulodexide
The UPCR during the pre-treatment (baseline) period was 1.5±0.6 g/g. There were no patients with nephritic-range proteinuria (>3.5 g/g). At the end of the observation period (11.1±2.7 months), the UPCR was reduced to 1.1±0.7 g/g (P=0.032) (Fig. 1). While the rate of UPCR reduction was 25% in more than half of the patients (Fig. 2A), 40% of them who had a pre-treatment UPCR of more than 1 g/g showed a UPCR of less than 1 g/g at the final observation (Fig. 2B).
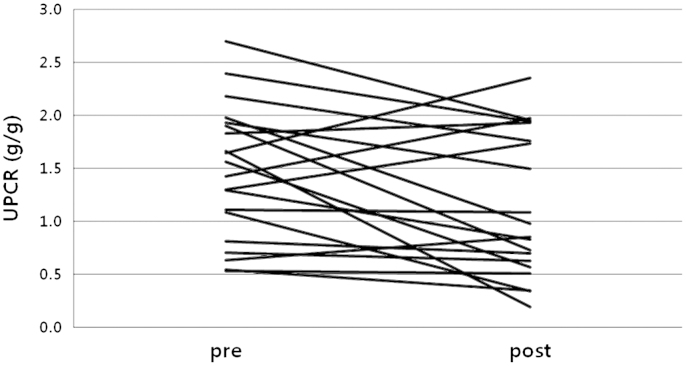
Changes in UPCR before and after sulodexide therapy. The Wilcoxon signed-rank test was used for the analysis, which indicated its significance (P=0.032).
UPCR, urinary protein-to-creatinine ratio.
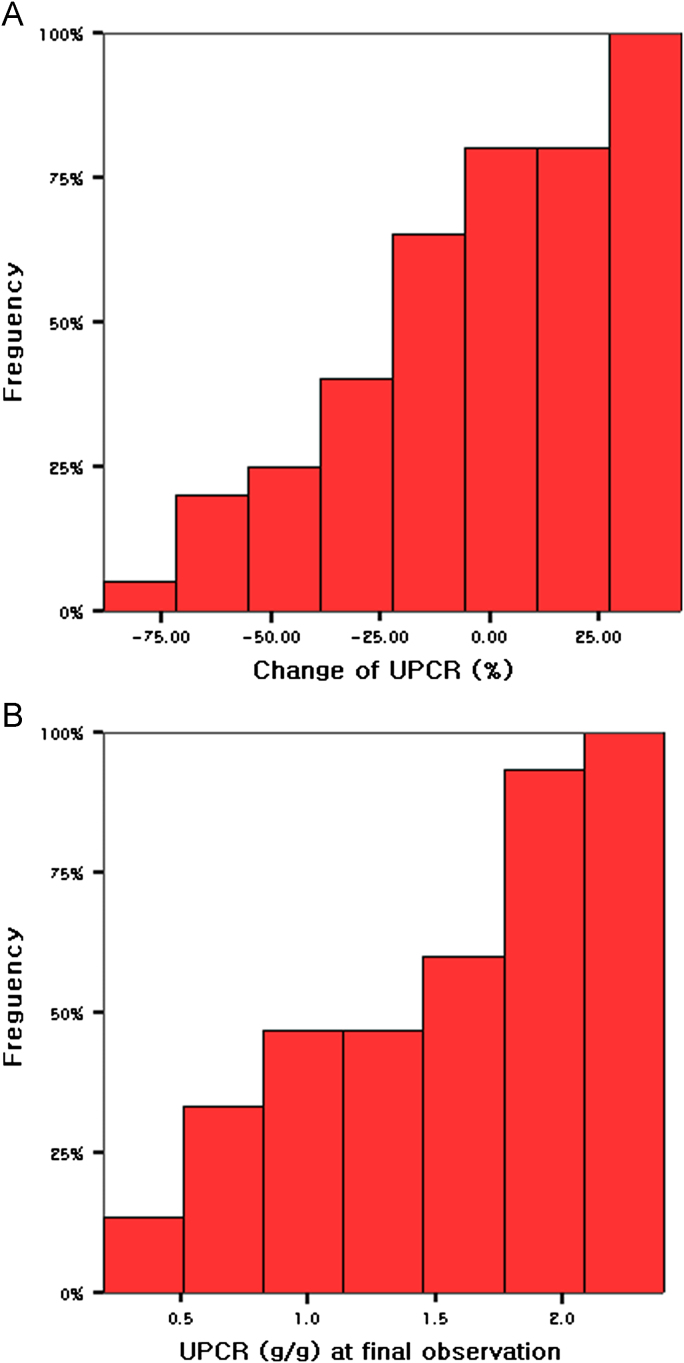
Analyses of the patterns in UPCR reduction by using cumulative histograms. (A) Frequency of each unit in the UPCR changes. (B) Frequency of each unit in the UPCR decreases at the final observation.
UPCR, urinary protein-to-creatinine ratio.
The initial findings were analyzed to identify which of the following factors were correlated with the decrease in UPCR: the pre-treatment eGFR, the year-duration of the RAS-blockades therapy, the pre-treatment UPCR, and the degree of FPE. In the analysis, we found that the pre-treatment UPCR showed a significant correlation with the decrease of UPCR (r=0.450, P=0.047), while the other factors did not (Fig. 3).
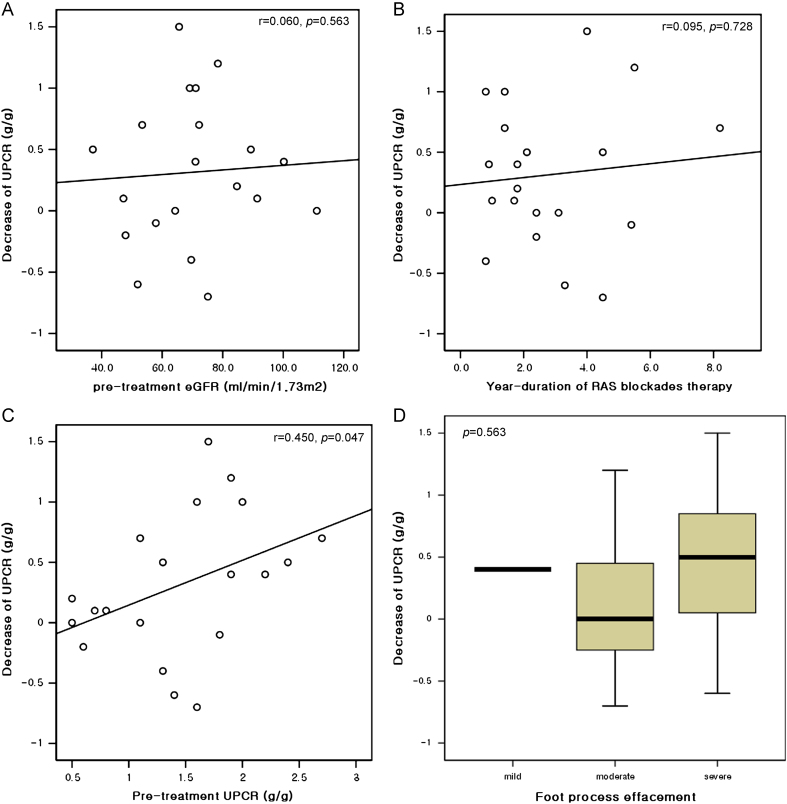
Correlation analyses between baseline factors and UPCR decreases. Pretreatment eGFR (A), year-duration of RAS blockades therapy (B), pre-treatment UPCR (C), foot process effacement (D) were the baseline factors used for analyses. The Spearman's correlation and the Kruskal–Wallis test were also used in these analyses. Pretreatment UPCR showed a significant correlation with decreases of UPCR (P=0.047).
eGFR, estimated glomerular filtration rate; RAS, renin–angiotensin system; UPCR, urinary protein-to-creatinine ratio.
Adverse effects
No adverse effects were reported after starting the sulodexide administration.
Discussion
In this study, we found a possible association between additional low-dose sulodexide therapy and further antiproteinuric effect in patients with IgA nephropathy who had persistent proteinuria (UPCR >0.5 g/g) despite optimal treatment with RAS blockades. The antiproteinuric effect was more pronounced in patients with high pre-treatment UPCR.
Sulodexide has been studied as a therapeutic tool for reducing urinary protein excretion in experimental models of diabetic nephropathy with diverse physiological properties related to renoprotection, including prevention of podocyte apoptosis [16], [17], inhibition of heparanase-1 activity [18], restoration of glomerular glycoprotein in the glomerular basement membrane (GBM) and mesangium with GAG supplementation [19], and restoration of the negative charge of GBM [20], [21]. It also suppresses the overexpression of transforming growth factor ß (TGF-ß), which is responsible for the enhanced expression of the mesangial matrix and collagens [22].
The efficacy of sulodexide in patients with diabetic nephropathy has been evaluated in some clinical studies. In the Diabetic Nephropathy and Albuminuria Sulodexide (Di.N.A.S.) study [23], the authors reported a decrease of albuminuria, including macroalbuminuria, by 74% in a dose-dependent manner. Low-dose oral sulodexide, 50 mg daily, was also investigated as an effective therapy for diabetes patients with albuminuria, including macroalbuminuria, which showed a reduction of the baseline albuminuria by a geometric mean of 63.7% for 6 months. The effect was greater in the macroalbuminuric patients [24]. But a recent randomized controlled study failed to prove the renoprotective effect of sulodexide in patients with overt type 2 diabetic nephropathy after 1029 person-years of follow-up [25]. Disappointing aspects were also seen in the studies of microalbuminuric diabetic patients. The Sulodexide Microalbuminuria Trial (SUN-Micro-Trial) could not demonstrate a decrease of urinary albumin excretion in microalbuminuric patients [26]; the same result was replicated in another recent randomized controlled trial in which any change in albuminuria was identical in both the treatment group and the control group [27].
A report related to GAG therapy in IgA nephropathy came out a few years ago, which included 12 patients with progressive IgA nephropathy who were administered RAS blockades and heparin/warfarin, resulting in the reduction of 24-hour urinary protein excretion by 71% at the final observation over a mean time period of 34 months [28]. A randomized, double-blind study of sulodexide treatment in IgA nephropathy patients was conducted recently [29]. As a pilot study, 77 patients with IgA nephropathy who already received RAS blockades participated and were assigned to placebo, 75 mg of sulodexide daily, or 150 mg daily groups. At 6 months, six (21.4%) of the total 28 patients in the 150 mg group showed more than 50% reductions of UPCR, while in the 75 mg group only one (4.0%) of the total 24 patients showed such a reduction. Although our results were similar to theirs concerning greater-than-half reductions of UPCR, there were three differences. First, the dose of sulodexide used in our study was lower than that in their study, but it appeared to be effective in 25% of the total patients. Second, most of patients in their study did not have significant baseline proteinuria, the mean being 0.6–0.7 g/g in UPCR, which was much lower than that in our study (1.5±0.6 g/g). Unlike in their study, we failed to see effective proteinuria reduction in patients with low baseline proteinuria (less than 1 g/g in UPCR) in the 75 mg group. Third, the duration of administration in our study was twice as long as that in their study. We assume that with the long-term use of low-dose sulodexide the effect can be achieved.
Although the presence of persistent proteinuria, over 500 mg/day, has repeatedly been demonstrated to be associated with an adverse long-term prognosis, it is very clear from well-done retrospective studies on large cohorts of patients with IgA nephropathy that a partial remission of proteinuria to levels less than 1.0 g/d is associated with a dramatically better prognosis [6]. In this present study, the proportion of the patients whose UPCR was decreased to 1.0 g/g was 40%, which is not inferior to the results from previous studies with glucocorticoid-based therapy. Our patients were not responsive to RAS blockades, which means that the result of the study might indicate an additive effect of sulodexide to the RAS blockade-based therapy cohort in which the proportion of remission of proteinuria was about 30–40% [7], [8]. The estimated response rate of conservative treatment with RAS blockades or with a RAS blockade–sulodexide combination therapy could approach about 60–65%, which is comparable to those (about 70–75%) in glucocorticoid-based studies [30], [31].
Patients with IgA nephropathy who received little benefits form RAS blockades have been studied in some trials in an add-on fashion. Combination of corticosteroids with ACEi or ARB may provide these patients with a high remission rate of up to 80% and a stable renal function [32], [33], [34]. Addition of oral calcitriol to RAS blockades for managing persistently proteinuric patients resulted in a modest decrease of proteinuria [35], [36].
In this study, throughout the sulodexide treatment period, no adverse effects were observed. Other trials with sulodexide did not document serious adverse effects either [26], [29]. In a recent meta-analysis of glucocorticoid-based therapy, however, the authors reported that widely recognized adverse effects could occur [31]. A study using a regimen of prednisolone (40–60 mg daily) for 4 months also reported that complications related to glucocorticoids occurred in 40% of patients [37].
Some practical recommendations suggest that the treatment of patients with IgA nephropathy who present hematuria and non-nephrotic proteinuria with or without mild renal impairment should include initial RAS blockades with or without fish oil for at least 3–6 months [7], [8]. However, the effects of fish oil in IgA nephropathy patients were noted to be inconsistent across studies, and its required doses were too large for the patients to continue the treatment [8], [9]. Therefore, in such cases, we suggest replacing fish oil with sulodexide and prolonging the management period with a RAS blockade–sulodexide combination therapy for up to at least 12 months in order to achieve an equivalent antiproteinuric effect of glucocorticoid-based therapy, unless there is an emerging nephrotic proteinuria or serious renal impairment.
Our study has some limitations. Small sample size could not allow the study to have a strong statistical power, and even some of the patients (25%) showed increasing UPCR at the final observation. Retrospectively collected data could not guarantee quality. There was no document of factors influencing the values of the variables, such as amounts of dietary sodium and protein intake and specific times of urine collection; neither could we ensure a treatment free of any adverse effects.
Our study is a case series dealing with uncontrolled paired comparisons. Therefore, we needed to take historical controls that contain outcomes such as 24-hour urinary protein excretion or UPCR. We found two trials depicting the progression of proteinuria using RAS blockades. One of the two trials showed that proteinuria had decreased by the first year in the most responsive patients, but did not report the remission rate [38]. Another documented that partial remission rate (<500 mg/d/1.73 m2) was 40% at the mean 38-month follow-up, but did not report serial data [39]. Thus, none of them could be used as a feasible control. From the two trial results, however, we presumed that about 60% of the patients treated only with RAS blockades would remain nonresponsive after the first year. The main issue is what to do with these patients [7]. Although sulodexide recently failed to demonstrate a renoprotective effect in patients with overt type 2 diabetic nephropathy [25], it is difficult for us to discard the possibility of sulodexide to treat IgA nephropathy, the most common nondiabetic glomerular disease. Large randomized controlled trials with longer managing periods are needed to confirm its antiproteinuric effect.
In conclusion, our work have shown that low-dose sulodexide has an additional modest antiproteinuric effect on IgA nephropathy patients receiving RAS blockade therapy.
Conflict of interest
All authors declared no competing interests.
References
Acknowledgments
This work was supported by a clinical research grant from the Pusan National University Hospital in 2011.