



Introduction
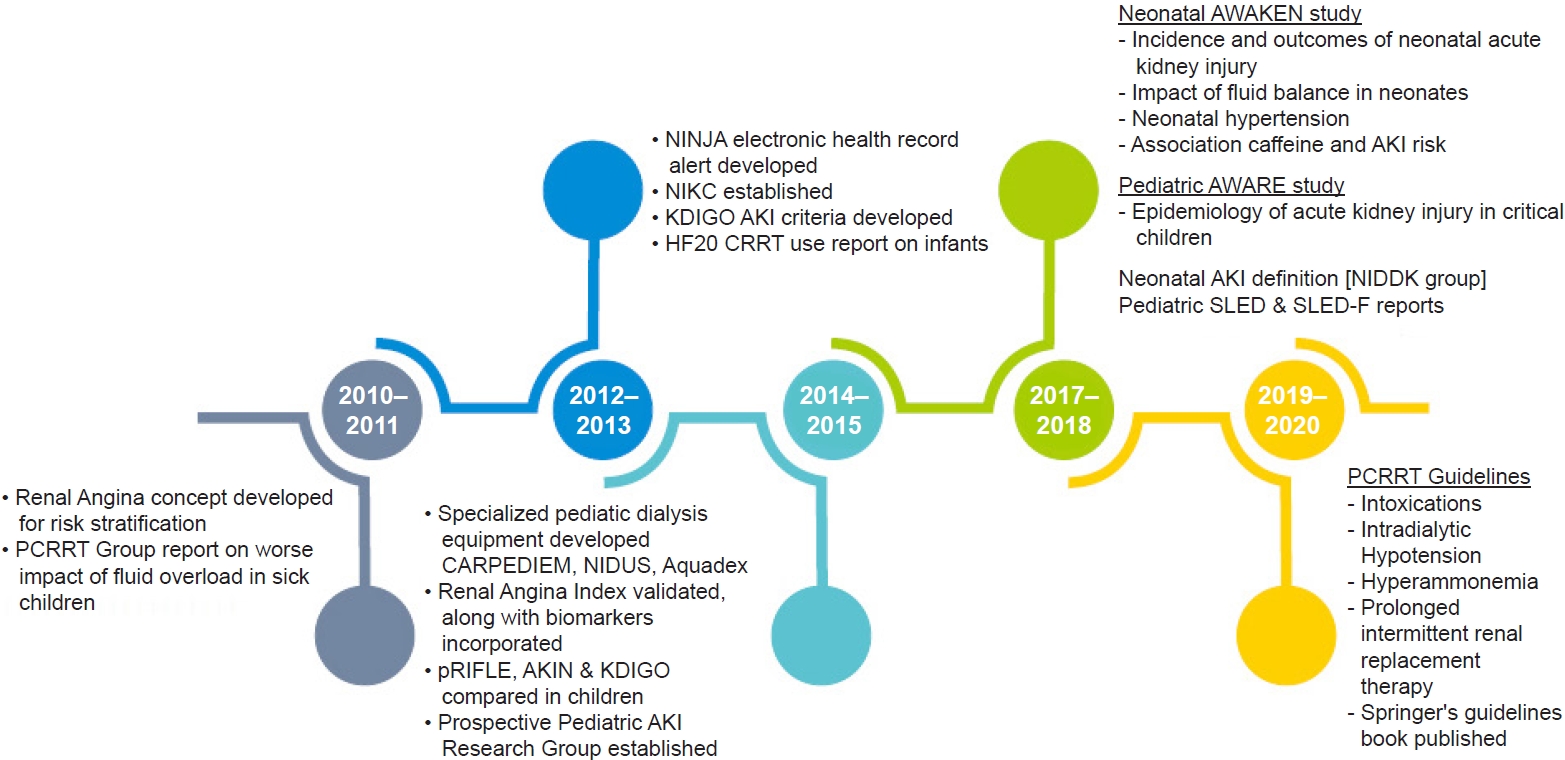
Acute kidney injury (AKI) is a common complication, affecting almost one-third of critically sick children and also noncritically ill children admitted to wards [1,2]. In the last decade, there has been a better understanding of outcomes in the field of pediatric AKI, which include higher morbidity, increased length of stay, duration of ventilation, and mortality [3,4]. There are newer studies on pediatric AKI epidemiology, clearly delineated definitions, newer biomarkers, and new criteria for risk stratification of children admitted in emergency situations. Additionally, definitions and the understanding of neonatal AKI have undergone a drastic change due to recent studies [5]. There is now novel research on machines made especially for smaller children with smaller extracorporeal volume [6ŌĆō8]. This review includes the major advances in the field of pediatric AKI in the last decade that have made a significant impact on learning and practice in this field (Fig. 1). This is a particularly important area of nephrology, where the clinical and translational advances have been performed first in pediatrics, much before the adult nephrology field.
Changing epidemiology of pediatric acute kidney injury
There is increasing evidence that the incidence and awareness of pediatric AKI is rising. In infants and children undergoing cardiac surgery, the incidence varies from 30% to 50% [9ŌĆō12]. Additionally, it is common in pediatric intensive care units (ICUs) and has an incidence of 10% to 35% [13ŌĆō15]. The rate is higher in children who are ventilated and are on inotropes [16]. AKI is also common in wards, especially in children receiving aminoglycosides and multiple nephrotoxins during their hospital stay [17,18].
The first prospective study on pediatric AKI, the Assessment of Worldwide Acute Kidney Injury, Renal Angina and Epidemiology (AWARE ) study, was done over a 3-month observational period and included 4,683 children [19]. This study showed that AKI was seen in 26.9% of children, and severe AKI was seen in 11.6% of children within 7 days of ICU admission. This increase in AKI severity was associated with a stepwise increase in mortality. Additionally, cardiovascular and respiratory disorders had a higher association with severe AKI.
Among the neonate subgroup, the largest retrospective study in the neonatal population, known as Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates (AWAKEN), was performed in 2017. This study included more than 2,000 newborns in four different countries admitted to the neonatal ICU before 14 days of life, who received intravenous fluids for at least 48 hours. AKI was seen in 30% of all newborns and was differently stratified per gestational age, with a higher incidence in extreme preterm birth infants. AKI was also associated with mortality and increased length of stay after adjusting for confounding variables [5].
Additionally, the etiology of AKI varies based on the geographic setting. In the developed world, the setting of AKI has shifted from primary glomerular disorders to hospital-acquired AKI, with common causes being nephrotoxins, critically ill status, postsurgical, posttransplantation, and malignancy [20,21]. In the developing world, especially in rural regions, the etiological factors remain as dehydration, sepsis, and hemolytic uremic syndrome [22].
Newer definitions of pediatric acute kidney injury
The ability of serum creatinine (SCr) to accurately estimate kidney function in a sick child has been problematic. This has resulted in the use of more than 35 definitions of AKI in clinical studies, ranging from changes in SCr to dialysis requirement. Earlier studies employed nonstandard AKI definitions without any grading (defining AKI as the doubling of SCr), thereby excluding early-stage AKI. Since there was no consensus in definitions, comparisons among studies were difficult, resulting in a wide range of quoted epidemiology, morbidity, and mortality rates within the pediatric AKI literature [23].
The Kidney Disease: Improving Global Outcomes (KDIGO) definition and staging system is the most recent and preferred definition even in pediatric AKI literature [24]. Other classification systems include pRIFLE (pediatric Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) and a subsequent modification proposed by the Acute Kidney Injury Network (AKIN) [25,26] (Table 1). Each definition confers its own set of advantages and disadvantages. For example, pRIFLE can diagnose a greater number of mild AKI cases that are usually missed by the other two systems but requires patient height and baseline SCr value, which might not be readily available. In pRIFLE, the estimated creatinine clearance (CCl) is based on the original Schwartz formula to quantitate the change in glomerular filtration rate (GFR) rather than absolute changes in SCr used in the adult RIFLE criteria. Furthermore, the pRIFLE classification has outperformed the AKIN, KDIGO, and conventional grading criteria in predicting AKI in several pediatric patient populations. Zapitelli et al. [27] found that AKI prevalence increased when changes in estimated GFR (eGFR) (pRIFLE) were accounted for rather than changes in SCr (AKIN) in pediatric inpatients. Additionally, Sutherland et al. [23] recently demonstrated notable differences in incidences and substantial disparities in staging resulting from the use of these three definitions on the same cohort of hospitalized children. The AKIN definition appears more specific and does not require height and baseline SCr values; however, it has the most restrictive diagnostic timeframe. The AKIN system, which defines AKI as a Ōēź0.3-mg/dL increase in SCr within a restrictive 48-hour period, eliminates the need to estimate CCl. However, the AKIN criteria have not been adequately validated for use in children and the restricted diagnostic timeframe of 48 hours for a rise in SCr may limit its utility. Although pRIFLE shows a greater sensitivity in detecting AKI than AKIN and KDIGO, all three definitions correlate highly with outcomes (mortality, length of stay in ICU) and enable outstanding inter-stage differentiation [23]. The KDIGO classification is the only one that applies to both children and adults and has a less restrictive diagnostic timeframe than AKIN. Although it does require patient height data (eGFR calculation) for a complete assessment, it is still the preferred definition. The KDIGO AKI criteria have been validated in hospitalized children with both critical and noncritical illness [23,28].
Emerging biomarkers
SCr is an indirect and unreliable marker of GFR that can be confounded by renal tubular secretion and numerous other factors such as fluid balance, muscle mass, and medications. Moreover, changes in SCr lag behind the changes in GFR, which can even take several days. In acute settings, it is estimated that SCr rises after a >50% decline in GFR [29]. Given the inherent shortcomings of the SCr method, alternative functional and damage biomarkers of AKI have been evaluated.
The use of serum cystatin C in children as an endogenous marker is well established. Cystatin C is a cysteine protease inhibitor protein, which is produced by all nucleated cells of the body at a constant rate, is freely filtered by the glomerulus, and is catabolized by the proximal tubule. The plasma cells are not affected by sex, age, diet, or muscle mass, and are identical in adults and children over 12 months of age [30]. It outperforms SCr in children for estimation of GFR. Moreover, there is now pediatric data to show that it is an early predictor biomarker of AKI [31].
Genomic and proteomic technologies have revealed novel biomarkers that appear in urine or plasma well before changes in SCr are detected [29]. The most widely studied and validated early biomarker in children is neutrophil gelatinase-associated lipocalin (NGAL) [32]. Most studies of NGAL have been done in children post cardiac surgery, showing that the urine and plasma levels are significantly high in children within 2 hours of cardiac bypass surgery in patients who subsequently develop AKI [33]. Another study done in infants and children undergoing cardiopulmonary bypass established cut-off thresholds and showed strong associations between early NGAL levels and length of hospital stay, duration, and severity of AKI [11,34]. A recent study done on 220 children undergoing cardiac surgery showed that urine NGAL increased in patients within 2 hours, while urine interleukin-18 (IL-18) and urine liver-type-fatty acid binding protein levels were elevated within 6 hours, and urine kidney injury molecule-1 increased at 12 hours. All markers correlated well with severity, clinical outcomes, and, additionally, improved risk prediction [35]. Thus, a panel of biomarkers may help to establish injury timely and plan appropriate timely interventions. Standardized clinical platforms for measurement of plasma and urine NGAL are now available globally.
Recent clinical data in children and adults support the utility and superiority of a new AKI biomarker test, NephroCheck (bioM├®rieux, Marcy-lŌĆÖ├ētoile, France), which detects urinary tissue inhibitor of metalloproteinase 2 (TIMP2) and insulin-like growth factor binding protein 7 (IGFBP7) concentrations and uses their arithmetic product [36,37]. AKI-induced urinary TIMP2/IGFBP7 elevations are not due to stress-induced gene transcription. Rather, increased filtration, decreased tubule reabsorption, and proximal tubule cell TIMP2/IGFBP7 urinary leakage seem to be the most likely mechanisms [38].
There is recent interest in patients who are ŌĆśbiomarker positive; creatinine negativeŌĆÖ which means their urinary or serum early biomarkers are high while SCr is normal. Two recent studies enrolled more than 4,000 cardiac surgical, critically ill and emergency patients [39,40]. Both studies showed almost >20% of patients had only elevated NGAL in urine. These ŌĆśsubclinical AKIŌĆÖ patients in fact had two- to three-fold higher risk of death and need for renal replacement therapy (RRT). Even in patients with very high creatinine, markedly high tubular markers in urine had a worse prognosis.
Hence, NGAL and a panel of urinary or serum biomarkers may help clinicians make an early diagnosis of AKI and plan supportive care early. Moreover, structural biomarkers may further help in reliably classifying AKI in a mechanistic manner. The various functional and structural markers are illustrated in Table 2.
Risk stratification at admission: application of ŌĆśRenal Angina IndexŌĆÖ
Renal Angina Index (RAI) combines objective parameters of kidney dysfunction (change in SCr and percent change in fluid overload [%FO]) and patient characteristics (AKI risk factors) to ascertain renal angina and has been successfully validated as a functional risk stratification tool in critically ill patients with AKI. An RAI of Ōēź8 within the first 12 hours of ICU admission has shown to entail very high sensitivity and negative predictive value for AKI development or persistence at 72 hours of ICU admission in children [41,42]. RAI is a risk discrimination model that enhances the pretest probability of AKI. It renders context to biomarker measurement and significantly optimizes their predictive performance, akin to the cardiac angina-troponin relationship. RAI has been shown to correlate with an increased need for RRT, prolonged mechanical ventilation, higher oxygenation index, and a higher risk of mortality when compared to children with a negative index score [43,44]. RAI entails moderate discrimination for predicting severe AKI prediction, but it improves after incorporation of biomarkers [45].
Clinical examination
Watch for fluid overload
Over the last decade, there have been studies in the adult population [46,47] and pediatric population (composed of neonates [48], post cardiac surgery [49], children with multiple organ dysfunction [50], and those on dialysis [51]) that have shown that fluid overload is common and is detrimental in sick patients. It is now well practiced in the intensive care to look at the percent fluid overload in sick children.
A common formula used is:
While fluid overload in children itself is not a direct marker of mortality, the adverse effects lead patients to become vulnerable to an increased risk of morbidity and mortality. It also puts patients at risk of being underdiagnosed with AKI and delays treatment, raises odds for mortality associated with complications, can lead to increased hospital and ICU stays, and can prolong ventilator support in the critically ill population [52].
Furosemide stress test to risk stratify patients
Clinicians have access to limited tools that predict which patients with early AKI will progress to more severe stages. In early AKI, urine output after a furosemide stress test (FST), which involves intravenous administration of furosemide (1.0 or 1.5 mg/kg), can predict the development of stage-3 AKI [53]. There are recent studies which suggest use of this test alone or in combination with biomarkers may predict progression to a severe stage of AKI in sick patients. Using an FST in patients with increased biomarker levels may improve risk stratification [53].
Newer laboratory tests in acute kidney injury differentiation
Automated urine technology and centralized laboratory testing are becoming the standard for providing urinalysis data to clinicians. It is critical to remember that urine sediment examination remains a time-honored test that provides a wealth of information about the patientŌĆÖs underlying kidney disease. This test performs very favorably as a urinary ŌĆ£biomarkerŌĆØ for a number of acute kidney diseases. Prerenal AKI from true or effective volume depletion is generally not associated with tubular injury/necrosis. In this setting, urine sediment is usually bland with no/few cells and casts. On the other hand, urine examination is one of the most useful tests in the diagnosis of acute interstitial nephritis and acute nephritic syndrome [54].
In addition to the tests that are commonly used in diagnosing etiology and complications of AKI, urinary indices, especially the fraction excretion of urea (FeUrea), have recently been studied. It is well known that the fractional excretion of sodium (FeNa) is >2% in children and >2.5% in neonates with a higher urine sodium >30 meq/L, which suggests tubular damage, e.g., acute tubular necrosis in the AKI setting. However, in certain situations of diuretic therapy or where the patient is on intravenous saline or presents with chronic kidney disease, FeNa may not be reliable. FeNa can then be substituted by FeUrea [55]. A FeUrea <35% implies prerenal AKI and FeUrea >50% suggests intrinsic AKI. A high FeNa and FeUrea >35% have a 95% negative predictive value for intrinsic AKI [56].
Neonatal acute kidney injury: newer advances
The major challenges confronted by clinicians involved in the care of neonates with AKI stem from numerous factors; unique renal physiology in term and preterm neonates, lack of a standardized AKI definition, and weight- and gestational age-dependent baseline SCr value in the neonates. Moreover, neonates usually have nonoliguric renal failure, making oliguria an insensitive marker of AKI in this cohort [57]. Neonatal AKI is further confounded by the reflection of maternal SCr levels in neonates for the first 3 days postbirth and the variable decline over days to weeks depending on gestational age [58].
The formation of the Neonatal Kidney Collaborative (NKC) was a giant leap forward which accomplished the heretofore unmet need of neonatal AKI quantification at a global level. The AWAKEN study retrospectively evaluated 2,022 neonates from 24 centers across the globe, which formed the NKC. The group concluded that neonatal AKI is common, with an incidence of 29.9%, and is an independent risk factor for mortality and prolonged hospital stay, independent of demographics, severity of illness, and existing comorbidities. The incidence of AKI was 43% in patients <29 weeks gestation, 18% in those between 29 and 36 weeks gestation, and 37% in those >36 weeks gestation [5].
Since maternal SCr is transmitted across the placental barrier and its clearance is dependent upon the infantŌĆÖs gestational age, the KDIGO definition was modified in such a manner that baseline SCr was assumed to be the lowest SCr level noted in each infant. Also, the SCr threshold for stage-3 AKI was reduced to 2.5 mg/dL rather than usual KDIGO threshold of 4 mg/dL [59].
A recent secondary analysis from AWAKEN also showed that caffeine administration in preterm neonates is associated with reduced incidence and severity of AKI. Further studies should focus on the timing and dosage of caffeine to optimize the prevention of AKI [60]. Other ancillary studies from the same group include a report on the association of AKI and hypertension [61], a study showing the association between AKI and mortality in those with severe neonatal encephalopathy [62], the association of AKI and intraventricular hemorrhage [63], and the association of AKI and chronic lung disease in premature and near term/term infants [64,65].
Newer machinery for smaller children
In the last decade, major innovations have been made in designing dedicated machinery with less error for dialysis of newborns and children. The most notable are the Prismaflex HF20 filter (Gambro, M├®yzieu, France), the CARdiorenal PEDIatric Emergency Machine (CARPEDIEM; Bellco-Medtronic, Mirandola, Italy), the Newcastle Infant Dialysis and Ultrafiltration System (NIDUS); and the Aquadex system (Baxter Corp., Minneapolis, MN, USA).
Prismaflex HF20 filters
Continuous RRT (CRRT) with Prisma or Prismaflex dialysis machines and M10 (50 mL) or HF20 (55 mL) filters with access via the internal jugular; 6.5 French hemodialysis (HD) catheters may be used. The Prismaflex HF20 set has recently been developed with relatively low circuit volume (60 mL) and is made of a polyarylethersulfone membrane, which is not associated with bradykinin release syndrome. There have been recent reports of successful use of HF20 filters in unstable infants [66,67].
CARPEDIEM
The challenge to design RRT equipment specifically intended for newborns and small infants weighing in the range of 1.5 to 10 kg led to development of the CARPEDIEM system. It received European certification in 2012 after thorough testing. It is a combination of hardware, software, and disposable circuits miniaturized and designed specifically for newborns and small infants with a reduced priming volume (27 mL including filter) with the roller pumps finely regulated by two precision scales accurate to 1 g. It was used for the first time on a neonate in 2013 and can be used in situations when adequate convective clearance is insufficient due to limited blood supply like in hypercatabolic states, where there is a need for increased dialysis efficiency [68,69].
NIDUS
NIDUS evolved as a novel HD circuit driven by syringes and uncouples the babyŌĆÖs blood flow capacity from requirements of the dialysis filter. The syringe driven machine repeatedly withdraws 5 to 12.5 mL aliquots of blood from a single lumen central venous line, passes and returns it across a dialysis filter, and then returns it back to the baby. At a blood flow rate of 20 mL/min, this processes 5 mL of blood each minute [8]. A multicenter trial on the use of NIDUS is recruiting babies in the pediatric ICU with a body weight of 0.8 to 7.99 kg, who require continuous dialysis as part of their standard clinical care. The recruitment started in January 2015 and is proposed to continue till December 2020 in the UK [70].
Aquadex
In order to mitigate the concerns regarding use of large extracorporeal circuits, the Aquadex circuit was adapted to provide prefilter replacement fluid for continuous venovenous hemofiltration (CVVH). The filter is 0.12 m2 and composed of a polysulfone membrane. Ultrafiltration rates of up to 500 mL/hr can be achieved for clearance of waste products. A recent pediatric experience of Aquadex has been published on ultrafiltration to provide a range of therapies, including CVVH, prolonged intermittent RRT, and slow continuous ultrafiltration. The group was able to initiate RRT with minimal complications, particularly in critically ill neonates [6].
Better understanding in prevention of pediatric acute kidney injury
Drugs to prevent acute kidney injury
Furosemide and bumetanide
In order to improve urine output in critically ill patients, furosemide has been used to maintain fluid balance. However, studies in adults have not provided any evidence that diuretics improve survival or help in recovery of AKI [71]. Studies in infants undergoing cardiac surgery have shown that furosemide infusion may be used instead of boluses to improve urine output [72]. Recently, bumetanide, a newer loop diuretic, has been used in preterm infants with oliguric AKI. While increasing urine output, there was a rise in SCr, highlighting the potential that loop diuretics can cause nephrotoxicity in this vulnerable population [73].
Fenoldopam
A recent study on fenoldopam, a selective dopamine A1 receptor agonist that decreases vascular resistance and increases renal blood flow, improved urine output in neonates requiring cardiac surgery with positive fluid balance despite diuretics [76]. Another recent study showed that a higher dose of 1 ╬╝g/kg/min during cardiac surgery may reduce the urinary NGAL and serum cystatin C levels, even without any changes in SCr [77]. However, the data is sparse on this drug.
Theophylline
During perinatal hypoxia in neonates, adenosine is released, which may cause vasoconstriction in the kidney causing a reduction in GFR [78]. Thus, nonspecific adenosine receptor antagonists, such as aminophylline and theophylline, may help in this specific setting. Three recent randomized trials showed a reduction in SCr and better urine output in severely asphyxiated neonates who were given a single dose of theophylline [78ŌĆō81]. Based on these trials, KDIGO also recommends a single dose of theophylline for asphyxiated neonates since they are at risk of AKI [82]. However, there are concerns about neurological side effects, and more so the relevance of these drugs in the era where hypothermia is a standard of care in these neonates.
Rasburicase
There is a recent interest in rasburicase (a recombinant urate oxidase enzyme) with a retrospective study in seven neonates with AKI. A single bolus of rasburicase reduced SCr, blood urea, and urine output [83]. However, more evidence is needed for the use of this drug in the treatment of AKI in neonates and children.
Electronic hospital software alerts to help clinicians prevent acute kidney injury
Recently, electronic software integrated within hospital management servers has been successfully used to prevent AKI by alerting clinicians well in time. Nephrotoxic Injury Negated by Just-in-time Action (NINJA) is a prospective AKI monitoring program used in Cincinnati ChildrenŌĆÖs Hospital. It uses an automated program to extract data in real time and flags noncritically ill children who are admitted and are receiving three or more nephrotoxins. These children undergo a daily surveillance of SCr, and the center noted a 38% reduction in the rate of nephrotoxin exposure and a concomitant 64% reduction in AKI rates [84]. Recently, a Baby-NINJA initiative in multiple neonatal ICUs reported a reduction in high nephrotoxic medication exposures from 16.4 to 9.6 per 1,000 patient-days (p = 0.03) and a reduction in percentage of nephrotoxic medication-AKI from 30.9% to 11.0% (p < 0.001) [85].
Newer advances in dialysis for children
RRT modalities for pediatric AKI have expanded from peritoneal dialysis (PD), HD to CRRT and sustained low-efficiency dialysis (SLED). Advancements in use of RRT in children have led to a higher standard of care for young and critically ill patients [86]. Since no difference in survival outcomes has been seen with any dialysis method, the optimal RRT modality to be chosen for children with AKI is based on the patientŌĆÖs size, overall clinical status, on the performance of the dialytic modality, and the availability of resources and expertise [87].
PD is the most common and simple method of providing solute and water removal in the ICU. It is easy to perform, can be easily learned, and does not require vascular access or anticoagulation. In a recent worldwide survey by Raina et al., 68.5% of respondents in developing countries preferred PD for treating infant AKI while only 29.1% of physicians in developing countries and 22.2% in developed countries favored PD to treat AKI [88]. Additionally, certain modifications to PD have been made recently to improve ultrafiltration, namely continuous equilibration PD, high volume PD, tidal PD, and continuous flow PD [89].
HD is the most efficient method of dialysis with rapid solute and fluid removal. It is ideal for managing pulmonary edema, hyperkalemia, intoxications, hyperammonemia, and acute tumor lysis syndrome [90]. However, patient hemodynamic stability is a must for a child to be put on HD. It does require a vascular access, careful evaluation of the extracorporeal blood volume (in the circuit and the dialyzer), and the need for anticoagulation [90]. Recently, the Pediatric Continuous Renal Replacement Therapy Foundation (PCRRT) gave recommendations on how to avoid intradialytic hypotension in children [91].
CRRT is the preferred modality for the management of AKI and fluid overload in critically ill children. It can be used with both or one of the diffusion or convection strategies. It is a complex dialysis modality that requires expertise and systemic heparin or regional citrate anticoagulation. The Prospective Pediatric CRRT Registry Group has published guidelines for dialyzing children with sepsis and multiorgan dysfunction in the last decade [51,92,93].
SLED is an alternative to CRRT in hemodynamically unstable pediatric patients with AKI. It utilizes conventional dialysis machines with low blood pump and dialysate flow rates for Ōēź6 hours daily. Recently, Sethi et al. [94,95] published a retrospective and prospective experience of SLED in unstable pediatric patients utilizing heparin-free dialysis and prefilter convective replacement fluid.
Conclusion
Management of AKI is challenging in critical infants and children. Over the past decade, revolutionary landmark studies and machineries have evolved, greatly improving the diagnosis, early detection, and management of renal support in this population. The pediatric nephrology community is working together closely to provide more scientific data to improve renal support in smaller critically sick children.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









