


Introduction
Since the first kidney transplantation (KT) was successfully performed between identical twins in a Western country in 1954, advances in immunosuppressive (IS) agents have improved short-term outcomes of allografts, reducing acute rejection [1]. Unfortunately, IS agents also cause many unwanted complications, including increased tumors, new-onset diabetes after transplantation, opportunistic infections, hair loss, neuropathy, and paradoxically, nephrotoxicity [2,3]. Malignancy in kidney transplant recipients (KTRs) is an important issue because it is the third most common cause of death and is also related to graft and patient survival during the late period after KT [1]. Previous reports have revealed a higher incidence of cancer in KTRs than in the general population worldwide [4–10]. Therefore, present guidelines recommend regular surveillance to screen for cancer in KTRs [11–14].
Due to advances in medical therapy, an extension of life span has been achieved in populations worldwide, including patients with end-stage renal disease (ESRD) [15–17]. In addition to an increasingly aging population, advances in medical equipment and an accumulation of experience have led to an increase in the number of patients with cancer diagnosis and treatment, in parallel with the increase in tumor incidence associated with aging [18]. The incidence of cancer has also increased over time in Korea [19]. As a result, the number of KT candidates receiving cancer treatment before transplantation is increasing.
Guidelines for KT candidates emphasize more frequent cancer screening among older patients [20]. Patients with pretransplant malignancies were not considered KT candidates in the past. However, an increase in cancer-free survival has increased the demand for transplant among ESRD patients with a previous malignancy to achieve freedom from lifelong dialysis. Therefore, the consensus KT guidelines were changed to permit transplantation on a case-by-case basis [2,14,21,22].
Despite an emphasis on tumor screening related to KT in the guidelines [20], the presence of cancer during the posttransplant period has rarely been investigated in KTRs with pretransplant malignancies. In this study, we sought to measure cancer recurrence and incidence rates in KTRs treated for pretransplant malignancies before KT.
Methods
Patient classification and clinical outcomes
We retrospectively reviewed data from 3,748 KTRs from The Catholic University of Korea, Seoul St. Mary’s Hospital after March 1969 and from Keimyung University Kidney Institute after November 1982, when the first KT was conducted in each institute, until December 2016. In each center, both pre- and posttransplant data of KT included donor and recipient information registered in a computerized system. KTRs with pretransplant malignancies were divided into three eras based on the progression of the nationwide regular surveillance system in Korea.
In the Republic of Korea, a cancer surveillance plan that covers the entire nation and targets medical aid beneficiaries was initiated in 1999. The national surveillance system gradually extended the diseases and cancer types monitored over time. Finally, the national policy recommended surveillance of specific cancer types in the entire adult population aged 40 and 66 years in a program called “The Life Transition Period Health Examination at the Korea Association of Health Promotion” in 2007. Therefore, we defined the first era as before and including 1998, the second era as between 1999 and 2006, and the third era as 2007 and beyond.
We investigated the proportion of KTRs with pretransplant malignancies, cancer type of pretransplant malignancies, cancer-free intervals until KT in KTRs with pretransplant malignancies, and posttransplant outcomes. All patients with pretransplant malignancies were monitored in the two transplant centers, including eight KTRs among these patients who experienced allograft failure. All tumors were confirmed by histopathological and radiological findings. Patients were diagnosed with only one cancer type. Patients with pretransplant malignancies in our institutes underwent KT based on previous guidelines [14,21,22]. This study was retrospective and exempted from written informed consent. This study was approved by the institutional review boards of The Catholic University of Korea, Seoul St. Mary’s Hospital and Keimyung University Dongsan Hospital (KC17REDI0665; 2017-10-007).
Changes in immunosuppressive regimen
Maintenance IS agents in the two centers consisted of azathioprine and corticosteroids until 1984. After that time, IS agents consisted of cyclosporine, as a calcineurin inhibitor, combined with corticosteroids, with or without azathioprine. Tacrolimus was introduced in 1998. Mycophenolate mofetil was introduced in 1999 for treatment of patients. However, since 2001, mycophenolate mofetil has been administered as an initial maintenance strategy. The target trough levels of tacrolimus and cyclosporine were 8 to 12 ng/mL and 150 to 300 ng/mL during the first 3 months and 3 to 8 ng/mL and 50 to 100 ng/mL thereafter, respectively. In May 2002, basiliximab was introduced as an induction therapy for most patients. Antithymocyte globulin was used as an induction therapy in highly immunized patients. At both centers, in 2009, a tailored desensitization strategy was initiated with combination therapy consisting of rituximab, plasmapheresis, and intravenous immunoglobulin for ABO-incompatible KT and for transplantation in highly sensitized patients.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 24.0 (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as the means and standard deviation and categorical variables are presented as frequencies (%). For normally distributed variables, between-group differences were evaluated using a Student’s t test. All tests were 2-tailed, and the results were considered significant when P < 0.05.
Results
Proportion of kidney transplant recipients with pretransplant malignancies
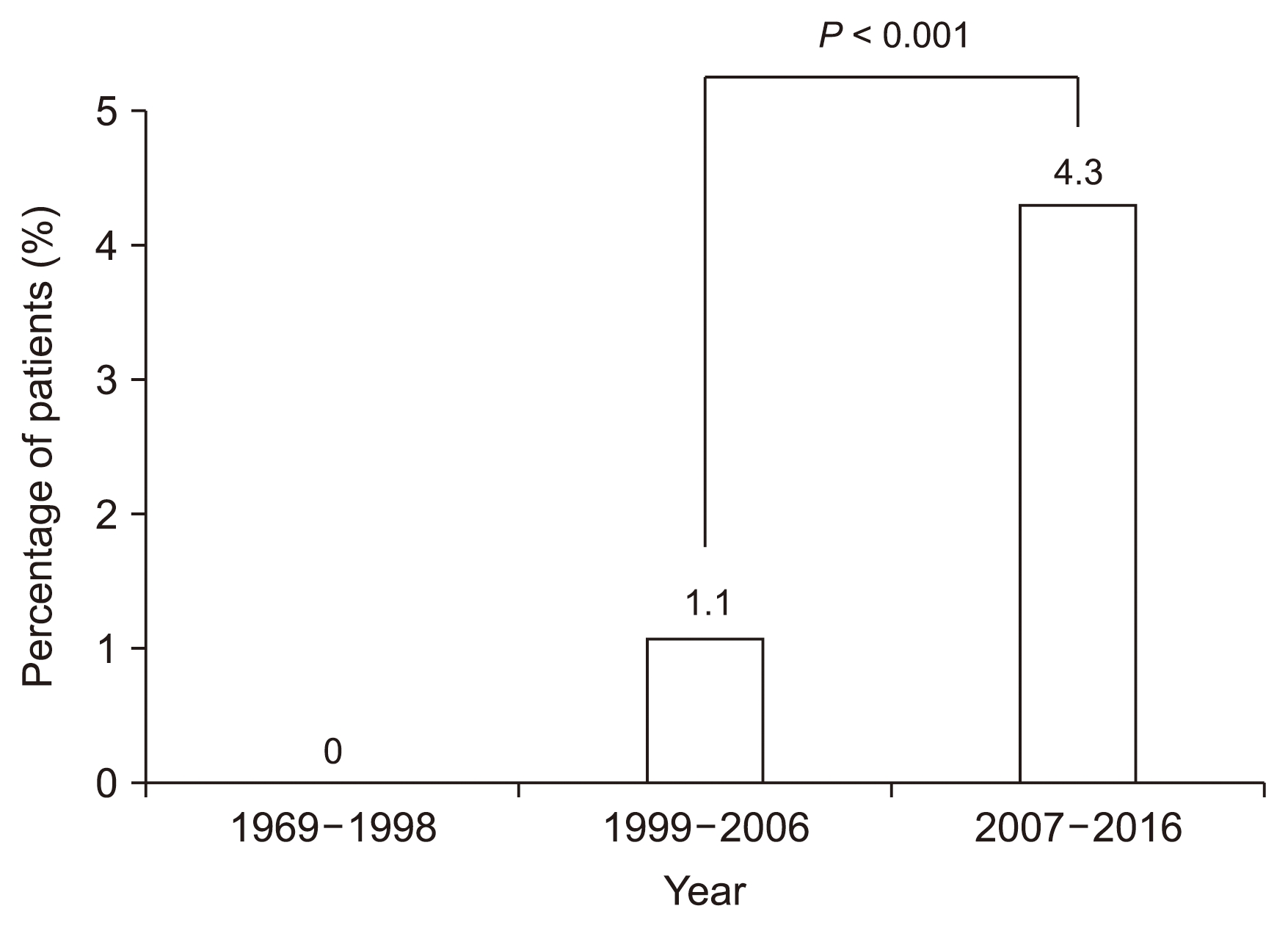
The mean age of the total patients was 40.6 years, and the proportion of males was approximately 60%. Table 1 summarizes the clinical characteristics of the patients. The incidence of KTRs with pretransplant malignancies based on regular surveillance is shown in Fig. 1. A total of 1.9% (72 patients) of KTRs among the total patients were cured of pretransplant malignancies. No patients with cancer underwent transplantation prior to 1998. A total of 1.1% (7 patients) of KT patients with pretransplant malignancies underwent transplantation between 1999 and 2006. The percentage of those patients increased to 4.3% (65 patients) during the third era. The proportion of KTRs with pretransplant malignancies significantly increased over time (P < 0.001).
Changing patterns in cancer type
Types of cancer in KTRs with pretransplant malignancies are summarized in Fig. 2. The major types of cancer in the second era were stomach (n = 2), liver (n = 2), and bladder (n = 2) cancer. Thyroid cancer (n = 20), renal cell carcinoma (RCC) (n = 13), stomach cancer (n = 6), and breast cancer (n = 6) were common in the third era. Therefore, the most common type of pretransplant malignancy for the entire period was thyroid cancer (n = 21), followed by RCC (n = 13), stomach cancer (n = 8), and breast cancer (n = 6). The cancer types in the remaining patients included cervical, colorectal, acute myeloid leukemia, carcinoid, endometrial, lymphoma, melanoma, pituitary, and anal cancer. During the third era, the majority of cancers were thyroid cancer and RCC. All thyroid cancers were classified as the papillary type, and all RCCs were classified as the clear cell type.
Cancer-free interval and incidence of posttransplant malignancy in patients with pretransplant malignancies
The mean cancer-free duration of each tumor type is displayed in Table 2. The mean cancer-free duration of all patients with pretransplant malignancies was 70.0 ± 66.6 months. In the KTRs with pretransplant malignancies, cancer was found in 3 patients (4.2%) during the posttransplant period. However, 259 (6.9%) KTRs without pretransplant malignancies were treated for cancer during the same period. The incidence of cancer in KTRs with pretransplant malignancies was not significantly different from the incidence in those without pretransplant malignancies (P = 0.48).
The types of cancer in all patients after transplantation are summarized in Table 3. Recurrent cancer occurred only in KTRs with pretransplant malignancy. After transplantation, the interval between de novo malignancy and recurrent cancer was 122.6 months and 59.8 months, respectively. These were not significantly different.
Discussion
The results of our study demonstrated that the number of KTRs treated for pretransplant malignancy has increased over time, and the common cancer types before KT have changed. The most common cancer types in KTRs with pretransplant malignancies were thyroid cancer and RCC. However, the recurrence rate of cancer was not increased in KTRs with pretransplant malignancies.
The most important finding of this study was that the proportion of KTRs with pretransplant malignancies increased over time. No cancer patients were reported for approximately 30 years prior to 1998. However, the proportion of cancer patients was 1.1% during the next 10 years and markedly increased to 4.3% during the final 10 years. The reason for this trend may be inferred from previous reports based on the regional population. The National Cancer Screening Program (NCSP) was initiated in 1999. Thereafter, the cancer types monitored by the NCSP gradually expanded, and the number of beneficiaries also increased over time. In addition, the number of participants who were also potential beneficiaries continuously increased during this time [23,24]. The national surveillance strategy includes the entire adult population aged 40 to 66 years for cancer screenings according to the policy of “The Life Transition Period Health Examination at the Korea Association of Health Promotion” instituted in 2007 [25]. Additionally, life span extension has occurred in all populations, including ESRD patients [15–17]. Both an increment of the aging population and advances in medical techniques have contributed to cancer diagnoses and cures [18]. The outcome of these factors has been an increase in the detection of cancer in the regional population over time [19]. In particular, early cancer detection has gradually increased, while the mortality from each type of cancer has decreased [26]. These findings suggest that we may encounter an increased number of KTRs with pretransplant malignancies in the near future. Thus, it is important to address the issue of safety associated with posttransplant cancer development in KTRs with pretransplant malignancies.
Pretransplant malignancies were barriers to KT in the past. These factors included an unestablished guideline for KT candidates cured of pretransplant cancer, inappropriate living donors, a limited number of deceased donors, and the introduction of the desensitization protocol. However, several guidelines were helpful for conducting KT in these subjects [14,21,22]. Some patients waited a long time for their children to reach adulthood in order to be a donor or to find another suitable deceased donor. Recently, other patients have been allowed to undergo KT after desensitization, resulting in the development of an acceptable strategy to treat KTRs with pretransplant malignancy over time.
The cancer types observed have also changed. In this study, the most common pretransplant malignancy found was thyroid cancer, followed by RCC. These two cancers have recently shown an increasing incidence. Indeed, not only was the cancer incidence distinct compared to those of other countries [27–29], but the pattern was different from that in the general population in Korea [19,24]. In domestic studies of CKD patients before dialysis and ESRD patients on dialysis, there were high incidences of colorectal, stomach, kidney, lung, thyroid, breast, prostate, and liver cancers [30–32]. The difference in prevalence of common cancer incidence and pretransplant malignancy in renal transplant recipients may be related to the age-related distribution of carcinoma patients, the cancer-free interval, and the increase in patient condition or mortality between the waiting periods during treatment. The major burden of these cancers affects the NCSP. The local population showed the highest incidence of gastric cancer, followed by thyroid, colorectal, and lung malignancies over the past 15 years [19]. In particular, the number of patients with small thyroid cancers rapidly increased, and these patients underwent thyroidectomy in considerable numbers, according to recent regional data [19,33]. Therefore, marked increases in thyroid cancer were observed in this study. Most subjects in the current study underwent dialysis for more than 5 years prior to KT. The presence of ESRD and its duration are independent risk factors for RCC. Therefore, RCC is the second leading cause of pretransplant malignancy in this study [34]. Interestingly, all thyroid cancer and RCC patients had the same type of cancer, papillary cell type and clear cell type, respectively. The types of cancer observed were comparatively less dangerous than other types of cancer [35,36]. These two relatively curable cancer types are different from the cancer types reported in previous studies [37]. Therefore, these findings suggest regular screening for thyroid cancer and RCC before KT.
The mean cancer-free interval before KT in the total patient group was 70.2 months, which was a substantial cancer-free interval despite the wide range of cancer types. Considering previous guidelines [14,21,22], this interval also complied with the criteria. Therefore, the favorable results of the current study were possibly due to achieving a cure for each cancer and a sufficient cancer-free interval. The other interesting finding in the present study was the lack of a significant difference in the cancer incidence of KTRs with pretransplant malignancies compared to that of KTRs without pretransplant malignancies. Only 3 patients in this study developed recurrent cancers; however, no patient developed de novo cancer. The low incidence of posttransplant malignancies among KTRs with pretransplant malignancies was inconsistent with the results found in other studies [37,38]. This discrepancy may be due to the slightly younger mean age of our patients [37]. Several studies have described a considerable incidence of cancer during the early period after KT [5,37,39]. However, this observational study followed patients for approximately 5 years (the longest follow-up duration was 17 years) and was able to significantly demonstrate the trend toward increasing safety in terms of posttransplant malignancy in KTRs with pretransplant malignancies.
This study has some limitations. First, cancer staging was not performed in this study. Second, the follow-up duration may not have been sufficient to analyze the incidence of all tumors. However, the mean follow-up time in the pretransplant malignancy group was approximately 5 years. Therefore, this duration may provide evidence that contradicts the high incidence of malignancy reported during the early period after KT in previous studies [5,37,39]. Third, despite cancer work-up before KT and regular posttransplant cancer screening, the issue of patient adherence may have affected cancer incidence. Although additional investigations of malignancies before transplantation are needed, we aimed to assess whether transplantation is safe after cancer treatment in KTRs with pretransplant malignancies compared to those without pretransplant malignancies. Nevertheless, the results of the current study showed that pretransplant cancer screening requires different strategies based on regional data, which may allow safer transplantation in KT candidates with pretransplant malignancies.
In conclusion, the number of KTRs with pretransplant malignancies is gradually increasing, and changes in the type of cancer presented have been observed. This observational study suggests that KT in patients who have been cured of pretransplant malignancies and have achieved a sufficient cancer-free interval may be safe with regard to recurrent and de novo cancer during the posttransplant period. Regular surveillance based on the present guideline is equally helpful for detecting cancer in KTRs with and without pretransplant malignancies.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









