


Introduction
Anemia is a common complication of chronic kidney disease (CKD). The most common cause of anemia in patients with CKD is decreased erythropoietin production owing to kidney dysfunction, and the prevalence of anemia increases when the disease progresses to end-stage kidney disease [1]. Anemia in patients with CKD is a known risk factor for the development of cardiovascular events and the progression of CKD [2–5]. It also lowers the quality of life and increases the economic burden on healthcare services [6,7].
Since the introduction of recombinant human erythropoietin in the 1980s, erythropoiesis-stimulating agents (ESAs) have become the primary treatment for anemia in CKD [8–10]. There are four types of ESA: epoetin alfa, epoetin beta, darbepoetin alfa (DA), and methoxy polyethylene glycol-epoetin beta, also known as continuous erythropoietin receptor activator (CERA) [9]. These agents have similar anemia correction effects but different pharmacokinetic profiles owing to differences in their molecular structures. The different half-lives result in different administration intervals [11,12]. ESAs with short half-lives require frequent injections, which create inconvenience for both patients and healthcare providers, and lead to poor treatment compliance, waste of healthcare resources, and high healthcare costs [13,14]. Therefore, recently developed ESAs have longer half-lives because of several molecular modifications [15]. DA and CERA are long-acting ESAs that are generally administered once in 2 weeks (Q2W) and once in 4 weeks (Q4W), respectively.
In the Korean National Health Insurance Service (NHIS), DA costs 40% less than CERA for the same dose, considering the dose conversion ratio (DCR). As the difference in the efficacy for anemia correction between the two ESAs is unclear, the cost aspect makes it difficult for clinicians to select ESAs for patients with monthly outpatient follow-ups. Patients with CKD who have economic problems often want to receive DA Q4W rather than CERA Q4W, and clinicians respect the patients’ wishes and often prescribe DA Q4W in Korea. In terms of half-life, DA Q4W is expected to be less effective for anemia management than CERA Q4W. However, in clinical practice, patients treated with DA Q4W often exhibit equally well-controlled anemia as those treated with CERA Q4W, contrary to expectations. Previous studies have also reported that DA Q4W is effective in patients whose hemoglobin (Hb) levels are well-maintained by Q2W administration [16]. Although the CORDATUS [17] and ACTOS studies [18] showed the non-inferiority of CERA Q4W to DA once in a week (QW) or Q2W, and CERA Q2W to DA QW, a randomized controlled trial (RCT) proving the non-inferiority of DA Q4W compared with CERA Q4W has not been performed.
The current study was conducted to test the hypothesis that subcutaneous DA Q4W is non-inferior in terms of anemia correction and superior in terms of cost-effectiveness to subcutaneous CERA Q4W in ESA-naïve patients with CKD not undergoing dialysis (ND).
Methods
Patients and clinical data
This single-center, randomized, open-label, non-inferiority study was conducted following the principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (No. 2018-05-008; CRiS No. KCT0003999). Informed consent was obtained from all participants.
We prospectively screened 19- to 99-year-old patients with stage 4 or 5 CKD ND at Soonchunhyang University Bucheon Hospital from April 2020 to April 2021. We enrolled patients with Hb levels of 8 to 10 g/dL, serum ferritin levels of ≥100 ng/mL, and transferrin saturation (TSAT) of ≥20%.
Patients with active cancer; decompensated liver cirrhosis; decompensated heart failure; or a history of arrhythmia, asthma, or chronic obstructive pulmonary disease were excluded from the study. Patients who were pregnant or planned to become pregnant and those previously treated with ESAs were excluded. Patients with bleeding events, including gastrointestinal bleeding, trauma, and menorrhagia, which can cause anemia in the past 3 months, were excluded. Esophagogastroduodenoscopy and colonofibroscopy were performed on all participants during the screening period with no evidence of gastrointestinal bleeding. Although we did not explicitly mention acute infection in the exclusion criteria, the infection status that may affect ESA responsiveness [19] of all participants was checked during the screening period, and we confirmed that all patients were free of acute infection
We obtained and analyzed the clinical information and laboratory data of the enrolled patients every 4 weeks during the study period. The estimated glomerular filtration rate (eGFR) was calculated using serum creatinine levels and the Chronic Kidney Disease Epidemiology Collaboration equation.
Erythropoiesis-stimulating agent administration
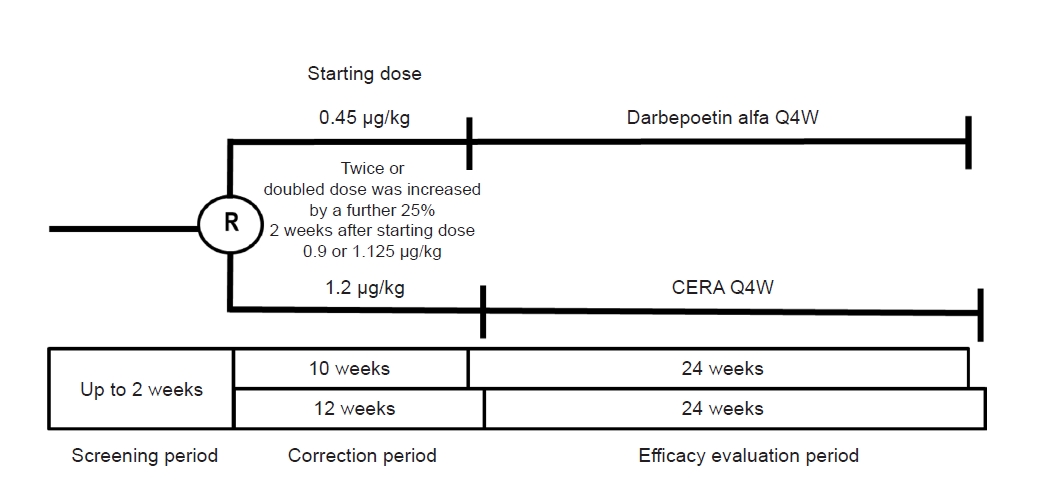
The study drugs were subcutaneously administered to each group. The first dose of each drug was defined as the starting dose. For the DA group, the initial dose was determined 2 weeks after the administration of the starting dose (0.45 μg/kg), and the dosing frequency was Q4W. Therefore, in the DA group, the initial dose differed from the starting dose. When the Hb level increased after 2 weeks, twice the starting dose (0.9 μg/kg/mo) was administered; however, when the Hb level did not increase, the doubled dose was increased by a further 25% (1.125 μg/kg/mo) (Fig. 1). The DA group underwent a 10-week correction period followed by a 24-week efficacy evaluation period (EEP). By contrast, CERA was administered Q4W at the same starting and initial doses of 1.2 μg/kg/mo. The CERA group underwent a 12-week correction period followed by a 24-week EEP (Fig. 1).
The target Hb level range was defined as 10 to 11 g/dL. Both drug doses were adjusted by 25% during the correction period until the target Hb level was reached. Dose adjustments were made during scheduled visits, no more than once every 4 weeks.
Iron supplementation
The protocol for iron supplementation was as follows: if the ferritin level was below 100 ng/mL or TSAT was below 20% during the study period, iron supplementation was initiated. If the ferritin level was 100 ng/mL or above and TSAT was 20% or above, supplementation was discontinued. Only oral iron supplements (ferrous sulfate, 512 mg/day) were used for iron supplementation.
Clinical outcomes
Two primary efficacy endpoints were analyzed: 1) the mean difference in the changes in Hb levels, defined as the difference between the mean Hb levels at the baseline and the EEP; and 2) the Hb response rates, defined as the proportion of patients who reached the target Hb level range during the correction period. The secondary efficacy endpoints included differences in the mean time to reach the target Hb level, the proportion of the duration within the target Hb range, and changes in Hb levels over time.
Safety profiles of the study drugs were monitored and analyzed during the study period. The following parameters were assessed: 1) changes in blood pressure and laboratory safety parameters, including Hb, creatinine, sodium, potassium, ferritin, and TSAT; 2) the nature and frequency of all adverse events (AEs) reported by the enrolled patients or observed by the investigator; and 3) the severity and relevance of the study drugs for all AEs determined based on the judgment of the investigator. Red blood cell transfusions and iron replacement therapy were recorded.
The doses and costs of the drugs in each group were compared over the duration of the study. The DCR was calculated and defined as the dose ratio of DA to CERA. Because the mean dose and cost were calculated as the average value of only the doses administered Q4W, the starting dose and cost in the DA group were excluded and analyzed separately. The cost of the study drugs was calculated based on the price of the pre-filled syringe administered, not the price per milligram, to reflect actual clinical practice.
Statistical analysis
The study’s sample size was calculated by analyzing the expected difference in the mean changes in Hb levels between the two groups. The participants were treated to achieve and maintain Hb levels between 10 and 11 g/dL. The expected difference in the changes in mean Hb levels from baseline to the EEP between the arms was 0 g/dL, and the anticipated standard deviation (SD) was 0.75 g/dL based on the historical DA and CERA clinical trial experience to date [16,20–23]. Because the SD was extremely small in previous studies, the sample size was considerably small when calculated based on it. Therefore, we set the SD at 0.75 g/dL more conservatively. For obtaining 80% power to test the primary non-inferiority Hb hypothesis with a two-sided 95% confidence interval (CI), a pre-specified margin of 0.75 g/dL, and a Student t test, a total of 16 evaluable participants per treatment group were required. Assuming a 20% non-evaluable efficacy rate, the sample size was calculated to be 20 participants per treatment group.
Descriptive characteristics of the study population are reported as mean ± SD for continuous variables and as frequency counts with percentages for categorical and binary variables. Comparisons between the groups were performed using Student t test for continuous variables and either Pearson chi-square test or Fisher exact test for categorical variables, as appropriate.
If the lower limit of the 95% CI was >–0.75 g/dL for the mean difference in the changes in Hb levels and >60% for the Hb response rate, we concluded that DA Q4W corrected anemia with non-inferiority to CERA Q4W. Differences between the two groups in terms of changes in variables over time were analyzed using a linear mixed model, which can minimize data omission due to missing values [24,25].
All statistical tests were two-sided, and p-values of less than 0.05 were considered to indicate statistical significance. All analyses were performed using IBM SPSS version 25 for Windows (IBM Corp.) or GraphPad Prism 5 (GraphPad Software, Inc.).
Results
Study population
Forty patients were enrolled in the study and randomized 1:1 to receive subcutaneous DA or CERA Q4W (n = 20 each) (Fig. 1). We used simple randomization for randomizing patients to each group. Table 1 shows the baseline characteristics and demographic data of patients in the DA and CERA groups. Demographic data, including sex, age, body mass index, blood pressure, and CKD etiologies; baseline serum creatinine levels and eGFR; and baseline anemia profiles, including the mean Hb and TSAT, did not differ between the two groups. Baseline ferritin levels tended to be higher in the CERA group than in the DA group (383.7 ± 404.1 and 235.0 ± 116.4 ng/mL, respectively; p = 0.13). The CERA group showed higher mean serum ferritin levels than the DA group (p < 0.001); however, the mean TSAT did not differ between the groups during the entire study period (Supplementary Fig. 1, available online). The type of antihypertensive agent administered did not differ between the groups. Nine patients dropped out of the study. The causes of discontinuation were loss to follow-up (five patients; three in the DA group and two in the CERA group) and starting hemodialysis (four patients; one in the DA group and three in the CERA group).
Efficacy
The mean difference in the change in Hb levels between the two groups was 0.375 g/dL (95% CI, –0.446 to 1.196) and –0.070 g/dL (95% CI, –0.730 to 0.590) in the intention-to-treat (ITT) and per-protocol (PP) populations, respectively (Fig. 2). The lower limit of the 95% CI for the group difference was above the protocol-specified non-inferiority limit of –0.75 in both the ITT and PP populations, signifying that DA Q4W is non-inferior to CERA Q4W for anemia correction.
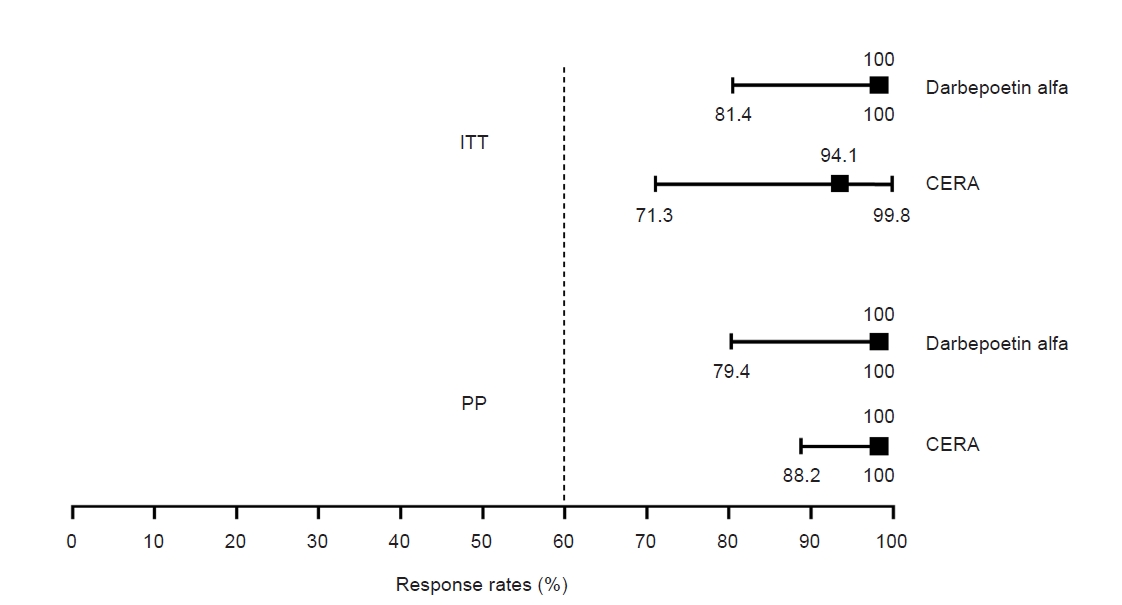
The Hb response rates during the correction period were comparable between the DA and CERA groups: 100% (95% CI, 81.4–100) vs. 94.1% (95% CI, 71.3–99.8) and 100% (95% CI, 79.4–100) vs. 100% (95% CI, 88.2–100) in the ITT and PP populations, respectively (Fig. 3).
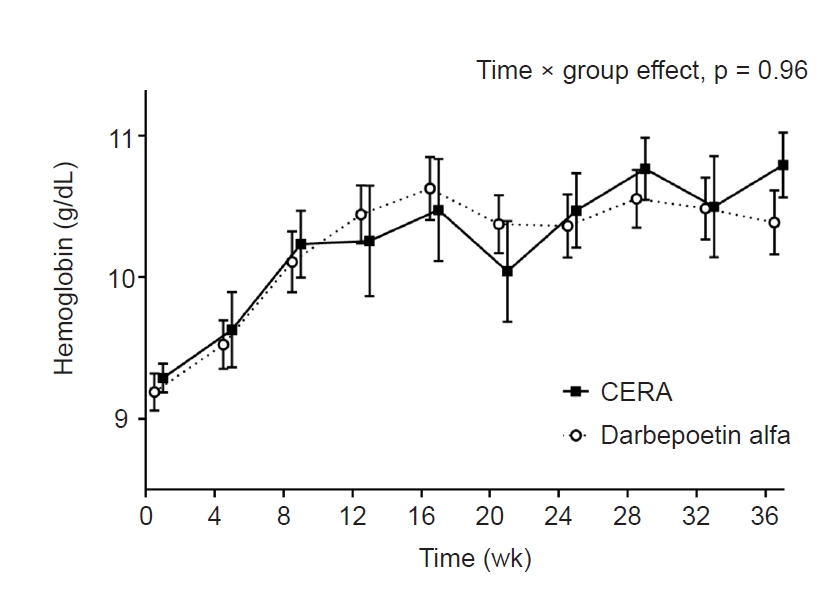
The mean time to reach target Hb levels did not differ between the DA and CERA groups in the ITT or PP population (Table 2). Furthermore, the mean percentage frequencies within, exceeding, and less than the target Hb range did not differ between the two groups in both the ITT and PP populations during the EEP (Supplementary Table 1, available online) and the total study period (Table 2). The mean Hb level increased in both treatment groups during the study period, and there was no significant difference in the change in Hb levels over time during the EEP (Fig. 4).
Nine patients (45.0%) in each of the DA and CERA groups received iron supplementation, with no significant difference in the mean dosage of iron supplementation between the groups (104,913 ± 40,832 and 91,787 ± 55,343 mg, respectively; p = 0.534). During the study period, there was no patient who received red blood cell transfusion.
Safety
The mean eGFR, systolic and diastolic blood pressure, and sodium and potassium levels over time did not differ between the two groups during the entire study period (p = 0.264, p = 0.999, p = 0.823, p = 0.941, and p = 0.978, respectively) (Supplementary Fig. 2, 3; available online).
All AEs in both groups were mild to moderate in intensity (Table 3). No severe AEs led to treatment discontinuation. Four patients in the DA group (20.0%) experienced AEs, including peripheral edema, neck pain, herpes zoster, and dyspnea. Three patients in the CERA group (15.0%) experienced AEs, including urinary tract infection, pulmonary edema, and femoral neck fracture due to a car accident. All AEs were probably (i.e., three out of seven) or definitely (i.e., four out of seven) not associated with the administered drugs and were successfully cured. Neither a cardiovascular nor thromboembolic event, which is a worrisome side effect of ESAs, occurred during the study period. No deaths occurred during the study period. The reasons for drug discontinuation were starting hemodialysis and loss of follow-up, not the administered drugs.
Dose and cost
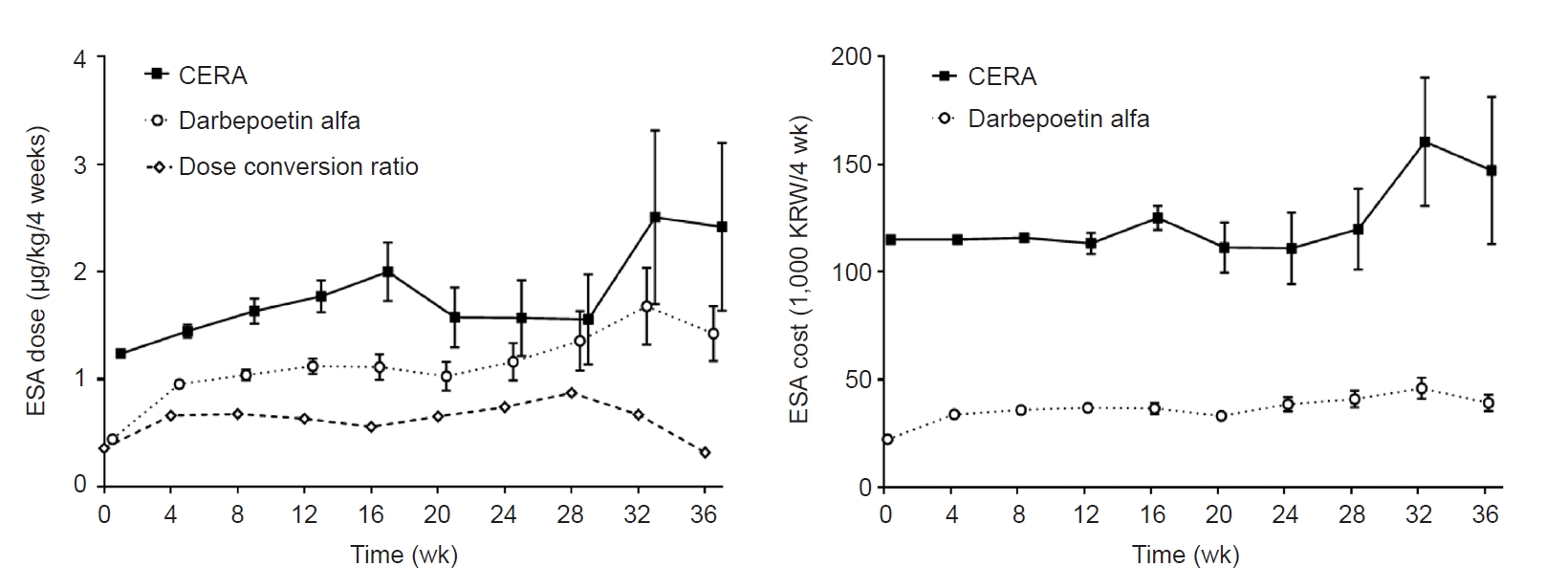
The doses and costs of the drugs administered in each group are presented in Table 4 and Fig. 5. The DCRs of the mean initial and total doses were 1.178 and 0.716, respectively. Changes in the mean ESA dose administered over time did not differ between the groups (p = 0.79). The mean total cost of DA was nearly one-third of that of CERA (34,100 ± 7,600 vs. 115,500 ± 23,600 Korean won/4 weeks, p < 0.001).
Discussion
This is the first RCT to compare DA Q4W with CERA Q4W in ESA-naïve patients with CKD ND. DA Q4W was non-inferior to CERA Q4W for anemia correction, including the mean difference in the changes in Hb levels and Hb response rates. The safety profiles were comparable between the two groups, and no serious AEs occurred in either group. The mean cost of ESAs administered every 4 weeks was nearly one-third in the DA group compared with that in the CERA group. These results suggest that DA Q4W for these patients not only leads to proper management of anemia but is also cost-effective compared with CERA Q4W in the real-world setting of Korea.
To compare the anemia correction efficacies of DA and CERA under the same conditions, the administration interval of the two study drugs was set to Q4W. Less frequent administration of ESAs has various clinical benefits, including increasing patient compliance and lowering the medical burden [26–28]. Over the past 30 years, ESAs with longer half-lives and less frequent administration have been developed through molecular modifications. DA is a synthetic analog of erythropoietin with an increased carbohydrate content and a long serum half-life of approximately 72 hours, and its circulating levels are retained above the erythropoiesis threshold 168 hours after subcutaneous administration [29]. Based on these pharmacokinetic advantages, pharmacodynamic studies on extending the dosing interval of DA to Q4W in patients with CKD ND have been conducted [16,20–23]. Most of these studies were performed in patients whose Hb levels were stably maintained within the target range by DA Q2W [16,20,21]. For these patients, the initial DA dose was calculated by summing the DA doses administered for 4 weeks before switching to Q4W administration; subsequently, the dosing frequency was adjusted to Q4W according to the Hb levels. The clinical outcomes were compared between the post- and pre-switching groups [16,20,21] and the CERA Q4W group [22]. Another study compared DA Q2W and Q4W in ESA-naïve patients with CKD ND [23]. Although interpretation and comparison of the results of each study are needed, all these studies reported that DA, not only Q2W but also Q4W is effective in managing anemia in patients with CKD ND. Although the current study design differed from that of previous studies, the current study also showed that DA Q4W is comparable in anemia correction and similar in safety profile to CERA Q4W. This result provides compelling evidence that DA Q4W can be as effective as CERA Q4W in patients with CKD ND, even though its half-life is shorter than that of CERA.
In the Korean NHIS, the cost of DA is 40% lower than that of CERA for the same dose, considering the DCR. Because the DCR of DA to CERA during the study period was slightly lower than expected, the mean cost of ESAs administered every 4 weeks was nearly one-third for DA compared with that of CERA. The 2012 Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline for Anemia in Chronic Kidney Disease recommends selecting the type of ESA by considering the balance of pharmacodynamics, safety information, clinical outcome data, availability, and costs [30]. In this respect, the results of the current study suggest that DA Q4W is preferable over CERA Q4W in the real-world setting in Korea.
To reflect actual clinical practice in Korea, the current study was designed according to the Korean NHIS’s reimbursement acceptance criteria for subject registration, initial ESA dose, ESA dose adjustment method, target Hb level range, and indications for iron replacement therapy. Therefore, there are several differences in current anemia management guidelines for patients with CKD ND. The 2012 KDIGO and the 2017 National Institute for Health and Care Excellence (NICE) anemia guidelines for CKD suggest that ESAs should not be used to maintain Hb levels above 11.5 g/dL [30] and ESA therapy should achieve Hb levels between 10 and 12 g/dL, respectively [31]. These guidelines indicate that decreasing the ESA dose is preferable to withholding ESA when Hb levels exceed the upper target limit [30,31]. In the Korean NHIS, physicians can start ESA treatment at Hb levels below 10 g/dL in patients with an eGFR of <30 mL/min/1.73 m2, prescribe ESAs only when the Hb level is ≤11 g/dL, and should be withholding ESA treatment when the Hb level is >11 g/dL in patients with CKD receiving ESAs. Taken together, the target Hb level in Korea is actually 10 to 11 g/dL; therefore, it appears that Korean patients with CKD ND are being treated for anemia at a lower and narrower target Hb range. The treatment strategy of withholding the ESA administration rather than reducing the ESA dose may cause large fluctuations in the administered ESA dose. The large fluctuations in the administered ESA dose and the consequent fluctuations in the DCR in the current study appear to be the result of this phenomenon. The inclusion criteria of the current study, according to the iron profile and indication for iron replacement, were set to the lower limit (serum ferritin, <100 ng/mL; TSAT, <20%) for intravenous iron administration under the Korean NHIS. This is consistent with the 2006 Kidney Disease Outcomes Quality Initiative [32] and the 2017 NICE guideline, which recommend iron therapy to maintain ferritin levels at >100 ng/mL and TSAT at >20% and defined iron repletion as ferritin levels >100 ng/mL and TSAT >20%, respectively. However, owing to the lack of evidence for the specific ferritin and TSAT levels at which iron therapy should be initiated, the 2012 KDIGO guidelines suggested only the upper limits of ferritin and TSAT levels for iron therapy. As there is no clear definition of iron deficiency for initiating iron therapy in patients who have started ESA therapy, each center’s and physician’s strategy for iron therapy may differ from the design of this study. The results of this study fully reflect Korea’s actual clinical practice; however, there are limitations to applying these findings to patients treated using other anemia treatment strategies or guidelines.
We attempted to compare the DA and CERA groups under the same conditions as much as possible, but there were two major differences. First, the correction duration, frequency, and method used during the correction period differed between the two groups. Regarding the approval of the DA dosing interval in Korea, to administer DA as Q4W, the Hb level should be evaluated 2 weeks after the initial administration. Because the study design followed this guideline, the correction period in the DA group was 2 weeks shorter and the dose correction was less than once compared with the CERA group. Second, the CERA group tended to have higher baseline serum ferritin levels and showed higher mean serum ferritin levels than the DA group during the study period. One participant in the CERA group had significantly high ferritin values (1,824–3,569 ng/mL). We could not identify any clinical factors that could elevate ferritin levels in this participant, who had no infection event or C-reactive protein elevation for 3 years from the time of study enrollment to the present. As this participant was properly registered in accordance with the inclusion and exclusion criteria, we believed that it would be inappropriate to exclude this participant’s data. Despite these two major differences between the two groups, these factors may disadvantage the DA group in terms of efficacy endpoints; therefore, it would not affect the finding that DA was non-inferior to CERA.
The current study has several limitations. First, the small sample size is a critical issue that can be considered a major limitation of this study. We calculated the sample size based on previous studies [16,20–23]. Unfortunately, in the CERA group, one more participant dropped out, and the target PP population included 15 participants. The drop-out rate was higher than expected because more patients dropped out due to the initiation of dialysis. Although the sample was one less than the target number of participants, the sample size may be sufficient to compare the efficacy outcomes because the SD was set conservatively when calculating the sample number. Second, as mentioned above, the current study was conducted as an RCT; however, the interventions during the correction period and serum ferritin levels during the study period differed between the two groups. Third, the protocol for iron supplementation in this study, which incorporated the reimbursement criteria of the Korean NHIS, did not reflect the recent trend recommending active iron replacement to reduce ESA use in patients with CKD [33,34]. Therefore, additional study reflecting the recent recommendations for iron replacement in patients with CKD is needed. Fourth, because the price of each ESA is different in different countries, the results of this study cannot be generalized. However, when calculated arithmetically, DA may be more cost-effective than CERA in countries where the price of the same dose, considering the DCR, is similar. Finally, the current study could not explain how DA, which has a shorter half-life, was comparable to CERA for anemia correction under Q4W administration. The administration interval of ESA depends both on the duration of the circulating ESA level above the erythropoiesis threshold, and the duration of the biological cascade resulting from the interaction between ESA and its receptors [11,29]. As the former is determined by half-life, it can be confirmed through pharmacokinetic studies and is generally used as an indicator of the ESA administration interval. However, the exact ESA administration interval remains unclear in that the latter is not yet known precisely [11,29]. It can be assumed that the unknown pharmacodynamic properties of each ESA agent may induce erythropoietic effects that offset the differences in the half-lives. We hypothesized that, when the level of circulating ESA surpasses the threshold required for erythropoiesis activation, erythropoiesis may be initiated, which may persist to some extent even when the concentration of circulating ESA falls below the threshold necessary for erythropoiesis. However, as this study did not intend to reveal causality, additional experimental studies are required to confirm this hypothesis.
In conclusion, our findings verified the hypothesis that DA Q4W is non-inferior to CERA Q4W for anemia correction. DA Q4W successfully and safely corrected anemia in ESA-naïve patients with CKD ND and is more cost-effective than CERA Q4W in a real-world setting in Korea.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print






")









