


Introduction
Preeclampsia is a pregnancy-specific disorder that affects 4% of pregnancies and is routinely diagnosed when a pregnant woman presents with increased blood pressure and proteinuria [1]. Preeclampsia is one of the main causes of maternal, fetal, and neonatal mortality, especially in developing countries [2]. The acute clinical importance of preeclampsia lies in its relation to maternal and neonatal mortality and morbidity. Pregnant women with preeclampsia can experience severe complications such as eclampsia, HELLP syndrome, pulmonary edema, or kidney failure [3]. The disease is also related to fetal growth restriction and preterm delivery. An increase in blood pressure can develop into renal dysfunction, and worsening of renal function will result in salt and water retention, which further complicate the hypertensive state. This vicious cycle can ultimately lead to severe pre-eclampsia, followed by poor obstetric outcome. Children born to mothers with preeclampsia have an increased risk of bronchopulmonary dysplasia and cerebral palsy caused by preterm birth and being small for gestational age [4,5].
The most common causes of acute kidney injury (AKI) in pregnancy are preeclampsia and eclampsia, which can ultimately lead to an increase in both fetal and maternal mortality rates [6]. Many biomarkers are available for the detection of kidney damage, and early AKI detection may be a potential predictor of preeclampsia [7–11].
Chapman et al [12] documented early rises in glomerular filtration rate (GFR) and kidney blood flow by inulin and p-aminohippurate clearance in association with systemic and kidney vasodilation in a series of 10 pregnant women [12]. However, as inulin and p-aminohippurate levels are determined by invasive investigation, these biomarkers are not suitable for screening for AKI in the setting of preeclampsia. Serum creatinine, which is widely used as a marker of kidney damage, has been shown to be a poor biomarker of early AKI in pregnancy because of its low sensitivity [13]. Kidney Disease Improving Global Outcomes (KDIGO) specified that normal serum creatinine levels are 0.4 to 0.8 rather than 0.8 to 1.2 in pregnancy due to underestimation caused by dynamic volume status. There are also no available creatinine-based formulae to accurately calculate estimated GFR (eGFR) in pregnant patients using serum creatinine [14]. Several studies have also shown that serum creatinine is unreliable compared to inulin, even though serum creatinine is the gold standard for calculation of GFR. Kidney injury molecule-1 and neutrophil gelatinase-associated lipocalin are other promising biomarkers of AKI. However, because the levels of these markers increase rapidly and normalize within 48 hours, they are not appropriate for use as screening biomarkers [15].
Cystatin C (CysC) has been studied intensively in pregnant women because it is independent of body weight, muscle mass, and other pregnancy-related changes [16]. CysC is a 13 kDa proteinase inhibitor from the cystatin superfamily of cysteine protease inhibitors that play important roles in intra-cellular catabolism of proteins and peptides. Some studies have shown that this biomarker is a better indicator of kidney function than creatinine [17,18], but there are no widespread recommendations for its use, even in pregnancy [19]. More intensive studies will have to be conducted before it can become a routinely used clinical biomarker. Several researches have described the utility of CysC as a biomarker in pregnancy. However, no prior study has investigated whether this biomarker is a predictor of poor obstetric outcomes [20–24].
In this study, we used serum creatinine and serum CysC to calculate eGFR using various formulae, and investigated if serum CysC level is associated with the obstetric complications of preterm delivery and low-weight babies in patients with severe preeclampsia.
Methods
Clinical data collection
We enrolled a prospective cohort of pregnant women diagnosed with severe preeclampsia who were receiving antenatal care at Her Royal Highness Princess Maha Chakri Sirindhorn Medical Center (MSMC), Thailand during August 1st, 2014 and September 30th, 2016. All women voluntarily signed a consent form before participating in our study. Data were collected from pregnant women with a maternal age more than 18 years and in the second half of pregnancy (gestational age, > 20 weeks). However, we included only severe preeclampsia cases with a gestational age of more than 28 weeks in our cohort. Those with a history or diagnosis of chronic hypertension, placenta previa, gestational diabetes, or chronic kidney disease with serum creatinine levels ≥ 0.8 mg/dL were excluded. Sample size was calculated using a power of 80%, alpha value of 0.05, and a dichotomous endpoint formula. Using data from a pilot project involving 10 pre-eclamptic patients (unpublished data), we found that the sensitivity and specificity of serum CysC for predicting preterm deliveries was 0.75 and 0.60, respectively. Using the Buderer approach and a severe preeclampsia prevalence of 1.3%, we calculated that we needed a minimum sample size of 25 [25,26].
A clinical study registration number for this study is TCTR20180730002. The protocol for patient participation was approved by the Human Research Ethics Board of Srinakharinwirot University (Issue #SWUEC/E-038/2557), and fulfilled the tenants of the 1964 Helsinki declaration and its amendments.
Clinical assessment of obstetric outcomes
Severe preeclampsia was defined as a systolic blood pressure (SBP) ≥ 160 mmHg or a diastolic blood pressure (DBP) ≥ 110 mmHg on two occasions at least 4 hours apart in a previously normotensive patient with a positive urine protein result (at least 1+ of dipstick urine protein), impaired hepatic function, progressive renal insufficiency, or new onset cerebral/visual disturbance, pulmonary edema, or thrombocytopenia (platelet count, < 100,000/mm3) [27]. Preterm labor was defined as babies born alive before 37 weeks of pregnancy [28] and low birth weight as a weight at birth of less than 2,500 g (5.5 pounds) or a fetus in the lowest 10th percentile of the fetal growth chart (gestational age confirmed by both date and ultrasound in all patients) [29,30]. Teenage pregnancy was defined as births to mothers aged 15 to 19 years and elderly pregnancy was defined as birth by mothers older than 35 [31,32].
Patients with severe preeclampsia received a magnesium infusion based on MSMC guidelines if their gestational age was more than 28 weeks and the obstetrician had ensured lung maturity of the neonate. Within 24 hours after infusion of magnesium, termination was considered. All patients had blood samples taken for investigation of complete blood count, liver function tests, and creatinine and CysC level determination for initial admission before receiving a magnesium infusion. Clinical parameters such as blood pressure, volume of fluid intake, urine output, and blood loss were monitored routinely until end of delivery.
Laboratory evaluation
Serum creatinine was measured by the enzymatic method using a Cobas® 6000 analyzer (Roche Diagnostics, Mannheim, Germany). Serum CysC was analyzed by an immunoturbidimetric method using an ARCHITECT ci8200 instrument (Abbott Laboratories Ltd., Bangkok, Thailand). All formulae were adjusted for non-black female patients. The eGFR based on CysC was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) CysC equation (2012) [33]. The eGFR based on creatinine was calculated using the CKD-EPI creatinine equation (2009) [34], Modification of Diet in Renal Disease Study (MDRD) creatinine equation (2006) [35], and Cockcroft and Gault creatinine equation. Individual eGFR was assessed using a web-based calculator (https://www.kidney.org/professionals/kdoqi/gfr_calculator) [36] after entering serum creatinine or CysC, age, and standardization assay without body surface adjustment. The Cockcroft and Gault creatinine equation (eGFR-CG) [37] was expressed as follows:
Urine protein level was assessed semi-quantitatively using the colorimetric method of tetrabromophenol blue reagent in urine dipstick [38]. The threshold used to define a positive test result was 300 mg/24 hours, 300 mg/dL, or a dipstick proteinuria reading of more than 1+ defined based on the diagnostic criteria of preeclampsia [39]. Only patients diagnosed with preeclampsia based on hypertension and persistently high thresholds (> 1+ proteinuria) were included in the study.
Statistical analyses
IBM SPSS statistical software package ver. 23.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Continuous data were evaluated to determine whether they followed a normal distribution. Parametric data were evaluated using parametric tests and Pearson correlation coefficients. Non-parametric data were evaluated using non-parametric tests and Spearman’s coefficient was calculated to assess the associations between various parameters and obstetric outcomes. Mean values and standard deviations were compared among groups using Student’s t test. Pearson correlation and logistic regression analyses were used to determine the significance of correlations between the various clinical parameters and obstetric outcomes. The area under the receiver operating characteristic (ROC) curve was used to assess diagnostic accuracy and to perform cross-validation analysis. P values less than 0.05 were considered statistically significant.
Results
Patient characteristics
Twenty-six pregnant women with severe preeclampsia who delivered at MSMC were analyzed in the present study. All patients had a normal serum creatinine level (0.40 to 0.80 mg/dL), and serum CysC ranged from 0.99 to 1.86 mg/L (1.43 ± 0.24 mg/L, mean ± standard deviation). Ten (38.5%) women who experienced preeclampsia were teenage or elderly pregnancies. The average gestational age at delivery was 37.07 ± 2.30 weeks. The incidence of preterm delivery was 38.5% (gestational age was confirmed by date and ultrasound). Incidence of low birth weight corrected by gestational age was 19.2% in this cohort (Table 1). Other complications often associated with preeclampsia like hepatitis or HELLP were not found in the present study. Other demographic data are presented in Table 1.
Association between eGFR calculated using various creatinine or CysC-based formulae
Four formulae were used to calculated eGFR: the CKD-EPI CysC equation (2012), CKD-EPI creatinine equation (2009), MDRD equation (2006), and Cockcroft and Gault equation. A significant directional correlation was found among all eGFR values. However, GFR estimated using the CysC-based calculation was drastically different from that estimated using the creatinine-based equations, with the CysC-based eGFR less than half of the creatinine-based eGFR values (Table 2, 3). Additionally, we found that up to 46.2% of severe pre-eclamptic patients had an eGFR < 60 mL/minute when calculated with CysC, whereas their serum creatinine levels were in the normal range. This implies that the creatinine-based equation may overestimate the real GFR, or that the CysC-based formula may underestimate the GFR. If the former is correct, CysC may potentially be more sensitive as an early AKI biomarker than creatinine.
CysC-based GFR and clinical outcomes
Binary logistic regression analysis was employed to predict risk of the adverse obstetric outcomes of preterm delivery and low birth weight body adjusted for maternal age and systolic and DBP. Only serum CysC was a significant predictor of preterm delivery (odds ratio, 32.52; P < 0.01). The eGFR calculated by creatinine- or CysC-based formulae did not predict preterm delivery. Neither renal function biomarkers (creatinine and CysC) nor eGFR could predict a low birth weight (Table 4). Proteinuria (protein dipstick) and systolic and DBP were also not predictive of low birth weight or preterm delivery.
Accuracy of serum CysC for predicting preterm birth in preeclampsia patients
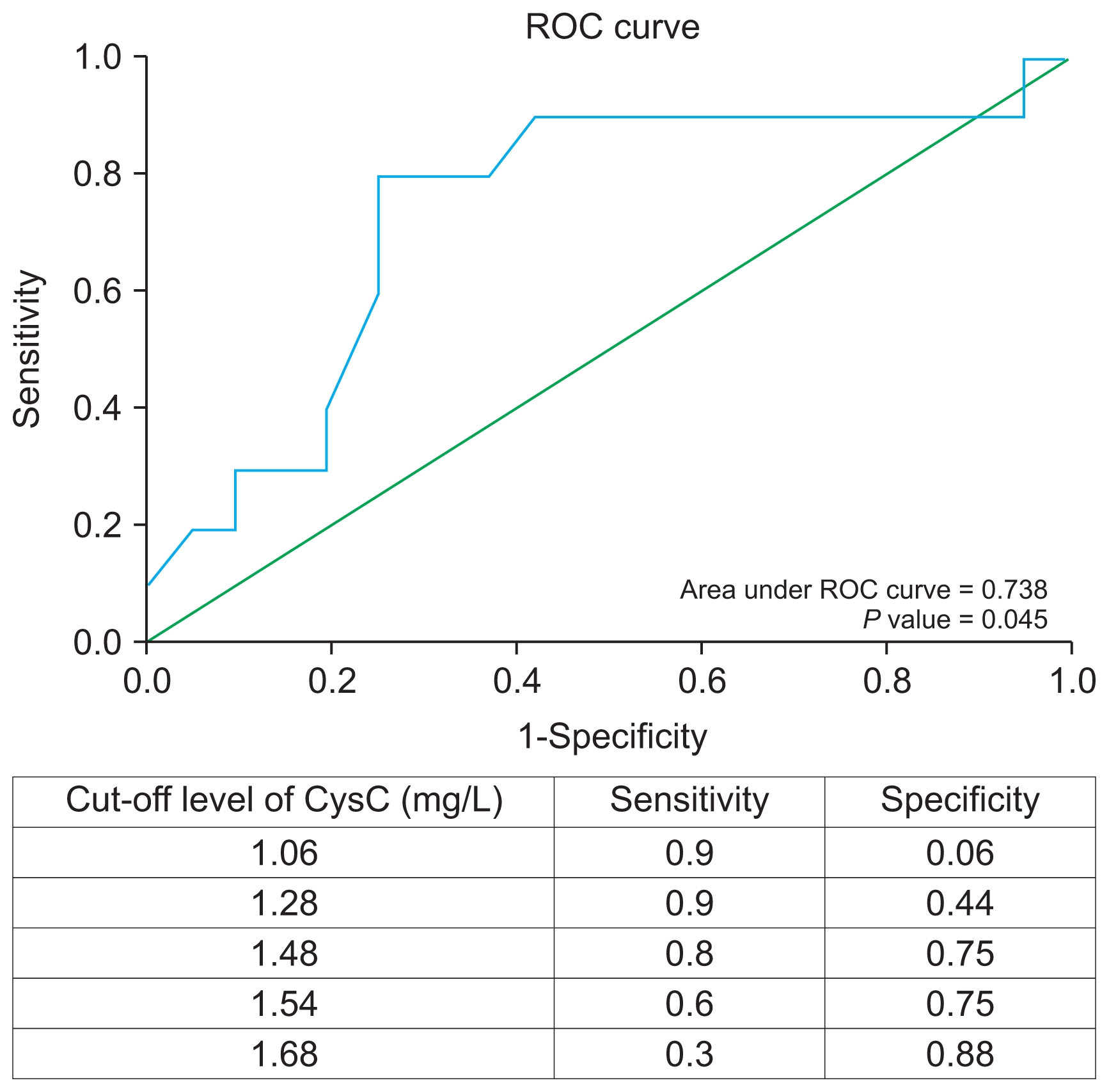
We further used ROC curve analysis to evaluate the accuracy of serum CysC for predicting preterm birth in our preeclampsia cohort. Analysis showed that the area under the curve was 0.738 with P = 0.045, indicating a high degree of discrimination.
ROC curve analysis suggested that the cut-off serum CysC level of > 1.48 mg/L was the best threshold for screening for the risk of preterm delivery in patients with preeclampsia with a sensitivity and specificity of 80% and 75%, respectively. Thus, a pregnant woman with in pre-eclampsia with a serum CysC level > 1.48 mg/L would be considered at risk for preterm delivery and require close monitoring and constant medical attention (Fig. 1).
Discussion
Renal function is often closely monitored in pre-eclamptic patients as it is a major concern [40,41] with the primary goal of timely delivery before irreversible kidney injury develops. Serum creatinine, serum CysC, and uric acid concentration are parameters that have been used previously to monitor renal function in hypertensive disorders of pregnancy [42–45].
Hemodynamic adaptations in pregnant women is crucial for healthy pregnancy outcomes [46]. These adaptations include a reduction in vascular resistance, increase in cardiac output, and increase in intravascular volume via sodium and water retention [47]. These changes also affect other organs. For instance, there will be an increase in GFR and effective renal plasma flow within the kidney, which are essential for maintenance of electrolyte balance [48]. Poor pregnancy outcomes are often observed in pregnancies where these physiological changes have failed to occur [49]. A study by Piccoli et al [50] in 2015 demonstrated a worse prognosis in mothers with stage 1 CKD.
CysC is produced by nucleated cells at a constant rate, and is then filtered and excreted by nephrons. Despite early enthusiasm, however, CysC has not been shown to have obvious superiority compared to creatinine [51]. The reason for this is that even though CysC levels are relatively constant in individuals under normal circumstances, it can be affected by several factors including smoking, liver disease, thyroid disease, diabetes mellitus, extreme age, and obesity [52–57]. Additionally, the higher cost associated with measuring CysC and lack of availability of tests has hindered its acceptance as a creatinine replacement to estimate renal function, even in pregnant patients [58].
We found that GFR values estimated using both creatinine and CysC were directionally and proportionally correlated. However, CysC-based GFR was approximately half the value of the creatinine-based eGFR estimates, suggesting that CysC underestimates the true GFR value. This also indicates that there are uninvestigated components in the CysC formula that makes it unsuitable for accurate estimation of GFR in pregnant women. Interestingly, none of the eGFR values were correlated with a poor obstetric outcome.
CysC may nevertheless have prognostic importance. CysC, in addition to being a biomarker of AKI, is also a known marker of inflammation [58]. There is mounting evidence that CysC may be a predictor of adverse outcomes independent of renal function. A study by Koenig et al [59] examined the association between plasma CysC and risk of secondary cardiovascular (CV) events in a cohort of over a thousand individuals who had a history of coronary heart disease. Creatinine and estimated creatinine clearance were not significantly associated with risk of a cardiovascular event. In contrast, higher plasma CysC was associated with an increased risk of a CV event, even after adjusting for well-known risk factors, including C-reactive protein. Compared with individuals in the lowest quintile of CysC, those in the highest quintile had a more than a two-fold increase in risk, even after adjusting for estimated creatinine clearance [59]. In this study, we found a correlation between serum CysC level and preterm delivery. Serum creatinine, semi-quantitative urine protein level, and hypertension showed no ability to predict obstetric outcomes in patients with severe pre-eclampsia.
In normal pregnancy, serum CysC levels are high (0.89 ± 0.12 mg/L) in the first trimester, decrease significantly (0.65 ± 0.14 mg/L) during the second trimester (P < 0.001 compared to first trimester), and increase again (0.82 ± 0.19 mg/L) in the third trimester.
In this study, the average serum CysC levels during the third trimester in pre-eclamptic patients was 1.43 ± 0.24 mg/L (Table 1), which is significantly higher than in normal pregnancy. This suggests that CysC may have adequate sensitivity to detect abnormal renal function even when serum creatinine levels are within the normal range. This has clinical significance because even small reductions in renal function are associated with adverse pathophysiologic consequences. By plotting a ROC curve, we found that a serum CysC concentration of higher than 1.48 mg/L has a sensitivity of 80% and specificity of 75% to detect preterm delivery in patients with preeclampsia (Fig. 1).
In conclusion, although CysC is a biomarker for detection of early AKI, eGFR using CysC during pregnancy is unlikely to be accurate, suggesting unexplored inflammatory processes that cause preterm delivery in mothers with preeclampsia. Our results indicate that CysC is a valid inflammatory marker that can predict preterm delivery in addition to being a biomarker of AKI. Serum CysC level therefore has the potential to predict preterm delivery in patients with severe preeclampsia.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






")









